Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
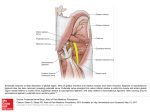
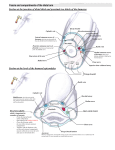
Gross Anatomy Unit 1 Clinical Correlation Surgical neck of humerus typically broken here Breast cancer when invading retromammary space and attaching to deep fascia overlaying p. major, breast becomes less moveable o Infiltration of suspensory ligaments will cause dimpling of skin causes skin to invaginate o Interference/blockage of lymph draining produces leathery skin o Intercostal vein connects to vertebral venous plexus route for cancer from breast to brain Sternoclavicular joint costoclavicular ligament is most important in preventing displacement (a type of fibrous joint) Acromioclavicular Joint coracoclavicular ligament is main support rupture causes clavicle to be driven superior to acromion o Acromioclavicular ligament rather weak and usually breaks when shoulder separates Glenohumeral joint weakest inferiorly o Stabilizing structures include coracohumeral ligament, glenohumeral ligaments, and rotator cuff Subacromial (subdeltoid) and subscapular bursa allow smooth motion Lateral epicondylitis tennis elbow Medial epicondylitis golfer’s elbow Surgery on ulnar collateral lig. From medial epicondyle to medial edge of trochlear notch Tommy John surgery Carpal tunnel syndrome decrease in size of carpal tunnel compression of median nerve numbness/sensory loss/motor weakness Dupuytrens contracture progressive fibrosis of palmar aponeurosis results in shortening/thickening of palmar aponerousis pull digit and MCP joint toward palm Ulnar nerve dmg common lies superficially in distal part of forearm o Sensory impair of ant/post aspect of medial part of hand o Deceased ab/adduction of fingers (interossei) o Adductor pollicis paralysis o Two med. Lumbrical paralysis Wrist fracture distal end of radius if abducted wrist scaphoid fracture Wrist slash dmg to artery and nerves Compartment syndrome of hand nerves are damaged due to increase pressure in capillaries Recurrent branch of median n. vulnerable to cuts on thenar eminence Primary curvature of VC thoracic and sacral evident in fetal dev. Secondary curve of VC cervical and lumbar as child develops Superior articular surf of axis forms synovial joint with occipital condyle nodding “yes” Dens process of axis and anterior arch of atlas “no” movement Cruciate lig holds alantoaxial joint in place prevents dens process from hitting spinal cord Cervical enlargement and lumbosacral enlargement of spinal cords Abdominal curvature of VC o Kyphosis hunchback o Lordosis swayback o Scoliosis Spina bifida non fusion of neural arch (lamina) at midline opening to VC Spondylolisthesis most common between LV5 and SV1 --> LV5 displaced from centrum and fuses with SV! pinching of nerve rootlets loss of sensation/pain/motor function Herniation of intervertebral disc in lower thoracic/lumbar impinges on next exiting spinal nerve Lumbar cisternal puncture btwn LV3-4 or LV4-5 avoids spinal cord btwn supraspinous and interspinous lig. Epidural anesthesia through sacral hiatus Tetraethyl ammonium (TIA) blocks nicotinic receptor of ACH in autonomic ganglion nerve signal can’t be forwarded Dopamine module Ach transmission KNOW ALL THE NERVE LESIONS Testing for nerve damage o Sensory loss C5 – lateral side of cub fossa C6 – Thumb C7 – Middle finger C8 – Pinky T1 – medial side of cub fossa o Motor loss C5 - Arm abduction (supraspinatus and deltoid) C6 – forearm flexors (brachialis and bicep brachii) C7 – forearm extensors (triceps) C8 – digital flexors (FDP ulnar side) T1 – digital abduction/adduction (dorsal/palmar interossei)