Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
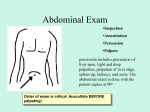
ABDOMINAL EXAMINATION Zhu Liangru Division of Gastroenterology, Union Hospital Range of Abdomen Superior:diaphragma Inferior: pelvis Lateral: lateral abdominal wall Anterior: anterior abdominal wall Posterior: back bone,psoas Abdominal Mark & Area Abdominal Mark Midabdominal Upper abdominal angle Xiphoid process line Costal margin umbilicus Lateral border of rectus muscles Anterior superior iliac spine Inguinal ligament Abdominal Mark • Costal margin composed of 8th-10th costal cartilage; abdominal area liver measure • Xiphoid process elongation of breast bone; measurement of liver • Epigastric angle included angle of costal arch; judge body type measurement of liver • Umbilicus center in abdomen;abdominal area • Anterior superior iliac spine the outstanding place of anterior of spine iliac • Lateral border of rectus muscles elongation of midclavicular line;operative incision • Midabdominal line elongation of anterior of median line; abdominal area • Inguinal ligament mark of femoral artery,femoral vein • Costalspinal angle included angle of 12th costal bone and back bone Abdominal Area region region epigastric region right lumber region umbilieal region left lumber right iliac region hypogastric region region left iliac region Abdominal Area: Nine regions left hypochondriac right hypochondriac stomach gallbladder ascending colon transverse colon small intestine ileum sigmoid colon urinary bladder Nine regions & Projection spleen left upper quadrant right lower quadrant Left lower quadrant Abdominal Area: Four regions right upper quadrant Right upper abdominal region Left upper abdominal region Umbilieal region Right lower abdominal region Left lower abdominal region Hypogastric region Abdominal Area: Seven regions Epigastric region Secquence of Abdominal Examination Examination secquence inspection, auscultation, palpation , percussion Recording secquence inspection, palpation, percussion, auscultation Inspection Attention of Inspection The patient is relaxed and in a proper position. The patient is in a supine position, the head should be elevated on a pillow, abdomen is thoroughly exposed (from nipple to symphysis pubic). Proper time to examination. Light is adequate and soft, and comes from one side of head. Inspector stands on the patient’s right side, secquence is from upper to lower. examination in tangent direction. Method of Inspection Abdomial Shape Normal:flat 、full、low xiphoid process umbilicus symphysis pubic low flat full Abdominal bulge whole abdominal bulge: ascites frog belly apical belly pneumatosis macrosis mass part abdominal bulge: organ intumesce (liver intumesce) tumor (stomach.liver,pancrease) inflammatory mass (tuberculous peritonitis) distension (stomach distension) mass in abdominal wall hernia ( umbilical hernia, indirect hernia) Inspection in Ascites Differential Diagnosis in mass in abdominal wall and mass in abdominal cavity Abdominal Retraction whole abdominal retraction athrepsy dehydration cachexia (boat-belly) part abdominal retraction : postoperative scar Boat shaped-abdomen Respiratory Movement Abdominal breathing: adult male, children Costal breathing: adult female attenuated in abdominal breathing : acute abdomen, ascites, macrosis mass, pregnancy reinforcement in abdominal breathing : diseases in thoracic cavity(hydrothorax), hysteria Abdominal Vein • Generally we can’t find distended abdominal vein in normal people. • Prominence of distended veins indicates increased collateral circulation as a result of obstruction in the portal venous system or in the vena cava • The normal direction of blood flow is away from umbilicus. The upper abdominal veins carry blood upward to the superior vena cava, the lower abdominal veins carry blood downtoward to the inferior vena cava. Portal hypertension Inferior vena cava obstruction Method to Judgement the Direction of Blood Flow Gastrointestinal pattern & Peristalsis Generally we couldn’t find gastrointestinal pattern and peristalsis in normal people. Gastrointestinal obstruction: gastral pattern intestinal pattern peristalsis Small bowel obstruction colon obstruction Others Information skin rash: infection diseases, drug allergy, herpes zona pigments: Addison disease, Grey-Turner sign, Cullen sign ventral stripe: striae albicantes, purple striae (hypercortisolism) scar: operation, trauma, infection hernia: umbilical hernia, oblique inguinal hernia, direct hernia umbilicus: evection, depression, secrection hairs: disposition, increase, decrease pulsation: abdominal aneurysm, increasing in right ventricle of heart Palpation Method of Palpation The patient is relaxed position The patient is in a supine position, the head should be elevated on a pillow, genuflex, slowly abdominal respiration Inspector stands right beside patient Start from left iliac region, anti-clock wise, “S” shape Commence palpation at a site remote from the area of pain All areas of abdomen must be palpated systematically Abdominal Palpation • Light palpation • Deep palpation Tensity Increase of tensity Intestinal distension, ascites, artificial pneumoperitoneum rigidity(board-like rigidity) acute diffuse peritonitis dough kneading sensation tuberculous peritonitis, carcinomatous peritonitis Decrease of tensity Chronic wasting disease, multipara, aged, dehydration Tenderness & Rebound tenderness tenderness rebound tenderness 1. Gastritis or gastric ulcer 2. Duodenal ulcer 3. Pancreatitis or tumor 4. Cholecystitis cholelithiaisis 5. appendicitis 6. Disease of intestine 7. Disease of urinary bladder,uterus 8. Ileocecal junction 9. sigmoid 10.spleen,splenic flexure of colon 11.liver,hepatic flexure of colon 12.pancreatitis McBurney point ant. Sup. spine Palpation of Organs One hand palpation Bimanual palpation Hooking technique Ballottement palpation Knee-elbow Position Palpation Attention in palpation of liver • Anterior-lateral finger pulp to palpate organs • Place your hand flat with fingers pointing towards the patients’s head • position of palpation at exterior margin of rectus abdominis • palpate deeply while asking the patient breathe in and out deeply • start in the right iliac fossa when examining macrosis liver Differential Diagnosis • Transverse colon • rectus abdominis tendon • Lower lobe of right renal Technique of Liver Palpation lung liver Projection of Liver Perpendicula distance 4-8cm Perpendicula distance 9-11cm Measurement Description of liver Size :below right costal margin 1cm, below xiphoid porcess 3cm Texture:three grade---soft,moderate, hard Surface:slick, nodus Edge:thickness, regularity Tenderness:no tenderness in normal liver hepatojugular reflux Pulsation:conduct pulsation, expansile pulsation Scrape:inflammatory surrounding liver Liver thrill:ballottement ---hepatic echinococcosis Manipulation of palpation of spleen Measurement of spleen Line I:distance from the across point of left medioclavicular line and costal border to inferior margin of splee Line II: distance from the across point of left medioclavicular line and costal border to ultima thule of spleen Line III: distance from right border of spleen to anterior median line Enlarged spleen mild acute hepatitis, typhoid,acute malaria, septicemia moderate cirrhosis, chronic lymphocytic leukemia, chronic hemolytic jaundice, lymphoma severe chronic granulocytic leukemia, myelofibrosis Description of spleen Size Texture Surface Edge Tenderness Pulsation Scrape Palpation of gallbladder manipulation one hand slipping palpation or hook Murphy sign Courvoisier sign Palpation of Kidney (A) Place left hand in the right or left loin posteriorly. (B) Place the right hand on the abdomen anteriorly and press gently dowmwards. Push the left hand upwards. A palpable kidney can be balloted between the two hands. The kidney may be palpable in thin normal individuals. The right kidney lies lower than the left, so it is more likely to be palpable. Nephroptosis enlarged kidney is found in nephrydrosis, empyema, tumor of kidney, polycystic renal disease Tenderness Point of nephric duct and Kidney Costa-carinal point hypochondrium Costa-lumbar 肋腰点 Upper nephric duct point point middle nephric duct point ventral aspect Back side Mass in Abdomen “Mass” in normal abdomen rectus muscle belly & tendinea body of lumbar vertebra cochlear of sacral bone stoolmass in sigmoid colon transverse colon caecum Abnormal Mass • • • • • • • Location Size length,broad,deep Shape skeleton,edge,surface Texture Tenderness Pulsation Degree of excursion Fluid thrill (Fluctuation) Manipulation of fluid thrill patient assistant inspector fluctuation Assistant places his hand vertically at the anterior median line, Examiner places hand flat at both side of lateral abdominal wall, One hand percuss one side abdominal wall, fluctuation can be sensed in another hand Succussion Splash Succussion splash can exist in people after meal or drinking Succussion splash exists in fast or 6-8 hours after meals suggests pyloric obstruction or gastric dilatation Percussion Percussion is used to demonstrate the presence of gaseous distension and fluid or solid masses. Light percession is preferable, since it produced a clearer tone. Abdomen Percussion Sound All four quadrant of abdomen are evaluated by percussion Tympany is the most commom percussion note in abdomen presence of gas within the stomach,small bowel,colon. Dullness exists in liver (right hypochondrium region) spleen (left hypochondrium region) distended urinary bladder (suprapubic area) enlarged uterus (suprapubic area) psoas (back side) Increasing in Dullness region organ swell tumor ascites Increasing in tympany gaseous distension perforation Percussion of Liver upper border of liver right midclavicular line right anterior axillary line right scapular line relative dullness area resonance dullness absolute dullness area dullness flatness lower border of liver right midclavicular line Anterior median line tympany dullness Normal Liver Border upper border right midclavicular line the fifth interspace right axillary line the senenth interspace right scapular line the tenth interspace lower border right midclavicular line right costal margin Measurement Size right midclavicular line 9-11cm anterior median line 4-8cm Change of Liver Border Increasing in liver dullness area liver carcinoma, liver abscess, hepatitis, polycystic Decreasing in liver dullness area acute hepatic necrosis, cirrhosis, gaseous distension Absence of liver dullness area acute perforation of hollow viscus Percussion Tenderness of Liver and Gallbladder Traube Area Traube area 9.5cm×6.0cm Percussion of Spleen route left midaxillary line normal spleen border left midaxillary line the ninth-eleventh interspace longitude 4-7cm Change of spleen border increasing enlarged spleen decreasing gastric dialation, distension Shifting Dullness The quantity of ascites is more than 1000ml Percussion of ascites tympany dullness Shifting Dullness tympany dullness supine tympany dullness lateral position Manipulation supine lateral position Place left hand on the umbilicus region, right hand percuss. note central tympany. Move left hand to one side of abdominal wall,then rotate patient onto another side. Notice that dullness has shifted toward the umbilicus on the dependent side. Tympany area has shifted toward the superior flank. Differential diagnosis between Ovarian cyst and ascites ascites ovarian cyst Differential diagnosis between Ovarian cyst and ascites tympany tympany dullness ovarian cyst dullness ascites Ruler Pressing test Sensitive to percussion in Ridge costal angle Projection of ridge costal angle right kidney ridge costal angle Sensitive to percussion in ridge costal angle Bladder Percussion Location:suprapubic area Empty bladder tympany Filling with urinary dullness Auscultation Area of Abdominal Auscultation pancrease liver spleen abdominal aorta gurgling sound arteria renalis Bowel Sound Auscultation of bowel sounds can provide information about the motion of air and liquid in the gastrointestinal tract. Normal 4-5/min Active >10/min Hyperactive mechanic intestine obstruction Hypoactive Absent paralytic intestine obstruction Vascular Murmur Arterial murmur center of abdomen: abdominal aneurysm abdominal aorta stenosis left or right upper quadrant: renal arterial stenosis bilateral of inferior belly:arteria iliaca stenosis left lobe of liver:left lobe carcinoma Venous murmur portal hypertension:umbilicus or epigastrium continious buzz Friction Sound Splenic infarction Perisplenitis Zuckergussleber Cholecystitis Peritonitis Scratch Sound Identify lower edge of liver Small amounts of ascites:puddle sign Thank you!