Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
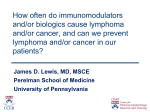
Thinking About Cancer Advances 2014 James D. Lewis, MD, MSCE Fernando Velayos, MD, MPH CCEB Case #1 • 35 y.o. male recently diagnosed with ileocolonic CD • Now steroid dependent • Treating physician recommends infliximab + azathioprine • Patient is concerned about risk of cancer, and particularly lymphoma Questions • Does immunosuppressant therapy increase the risk of lymphoma? • Do the benefits outweigh the risks? • Is there a way to minimize the risk? AZA/6-MP & Lymphoma: Meta-analysis Author Observed Expected Connell 0 0.52 Kinlen 2 0.24 Farrell 2 0.05 Lewis 1 0.64 Fraser 3 0.65 Korelitz 3 0.61 Total 11 2.71 SIR = 4.06, 95% CI 2.01 – 7.28 CCEB Kandiel A et al. Gut. 2005:54:1121-25 CESAME - Lymphoma At cohort entry N Never exposed to thiopurines 10,810 6 Reference On therapy with thiopurines 5,867 16 5.3 (2.0 – 13.9) Previously discontinued thiopurines 2,809 2 1.0 (0.2 – 5.1) CCEB # HR (95% CI) Lymphomas Beaugerie L. Lancet 2009 DOI:10.1016/S0140-6736(09)61302-7 Anti-TNF Therapy and Any Cancer Accumulate d doses Any 1-3 Personyears 19,559 6694 Cases 81 31 Adjusted Rate Ratio (95% CI) 1.07 (0.85-1.36) 1.02 (0.71-1.47) 4-7 8+ 4664 7083 18 32 0.89 (0.55-1.42) 1.29 (0.90-1.85) Anderson NN. JAMA 2014;311:2406-13 Combination Therapy and Risk of Lymphoma Therapy # Lymph SIR 95% CI Never thiopurine or TNF (1) 6 1.5 0.5 – 3.2 Never thiopurine or TNF (2) 33 1.0 0.96 – 1.1 Current thiopurine w/out TNF (1) 13 6.5 3.5 – 11.2 Current thiopurine w/out TNF (2) 4 1.4 1.2 – 1.7 Current TNF w/out thiopurine (2) 0 0 -- Current TNF + prior thiopurine (2) 1 5.2 3.5 – 6.8 Current thiopurine + TNF (1) 2 10.2 1.2 – 36.9 Current thiopurine + TNF (2) 1 6.6 4.4 – 8.8 (1) Beaugerie L. Lancet 2009 DOI:10.1016/S0140-6736(09)61302-7 (2) Herrinton L. Am J Gastroenterol 25 October 2011; doi: 10.1038/ajg.2011.283 Contribution of Thiopurines and TNF to Cancer Risk Osterman MT et al. Gastroenterology 2014;146: 941-9 Clinical Questions • Does immunosuppressant therapy increase the risk of lymphoma? – Thiopurines – yes, but risk may revert after discontinuation – TNF – Possibly but appearing less likely with more data – Combination – Yes and possibly more than thiopurine monotherapy • Do the benefits outweigh the risks? Relationship of Age and Outcome with Azathioprine Therapy Gain in Quality Adjusted Years 0.09 0.08 0.07 0.06 0.05 0.04 0.03 0.02 0.01 0 -0.01 0 20 40 60 80 Age (years) CCEB Lewis et al. Gastroenterology 2000;118(6): 1018-24 Combination versus Anti-TNF Monotherapy • Modeled across age ranges from 25 to 75 and across duration of therapy from 1 to 9 years • Assumes naïve to both drugs • Allows for second anti-TNF in case of LOR • Key effectiveness assumptions derived from SONIC, GAIN and CHARM • Key lymphoma assumptions derived from CESAME Scott FI. CGH 2014 One Year Outcomes 100% 90% 24.4% 26.3% 80% Active 70% 60% 25.5% 30.1% 50% 40% 26.8% 30% 22.5% Post-operative remission Response Remission 20% 10% 22.9% 20.7% Combination Therapy IFX Alone 0% Scott FI. CGH 2014 Age-Dependent Incidence of Lymphoma Scott FI. CGH 2014 Age and Duration Influence Preferred Strategy *** ***HSTCL (or HLH due to acute EBV infection) - Monotherapy becomes the preferred strategy if incidence in 25 year old male exceeds 36 per 100,000 per year Scott FI. CGH 2014 Clinical Questions • Does immunosuppressant therapy increase the risk of lymphoma? – Thiopurines – yes, but risk may revert after discontinuation – TNF – Possibly but appearing less likely with more data – Combination – Yes and possibly more than thiopurine monotherapy • Do the benefits outweigh the risks? – In most scenarios • Is there a way to minimize risk? Prevalence of EBV • • • • 20% to 40% of college freshmen >60% of recent college graduates >70% of young adults Possibly even higher rates in other countries Niederman JC et al. NEJM 1970:282:361-5 Prevention of Immunosuppression Related Lymphoma • Avoiding treatment in EBV infected often not feasible • Consider avoiding thiopurines in young, EBV-negative patients to avoid fulminant infection and HLH • Consider discontinuation of medications that are not effective for IBD, particularly in young males and elderly Case #2 • • • • • • 50 year old male 30 year history of small bowel Crohn’s 1 prior bowel resection Current meds – 6MP + Adalimumab 3 BM per day Colonoscopy – few scattered aphthous ulcers in the neo-TI Clinical Scenario (cont) • 2 years prior diagnosed with NMSC (BCC) • 2 weeks ago newly diagnosed with SCC • Questions – Is skin cancer risk increased by therapy? – If so, does the risk of continuing therapy outweigh the benefits? Non-melanoma Skin Cancer • Increased incidence in immunosuppressed – Transplant patients – • 65-250 x increase in SCC • 10 x increase in BCC – HIV/AIDS – Proportional to degree of immunosuppression • Increased severity of SCC in immunosuppressed Euvrard S. N Eng J Med 2003;348:1681-91 Maddox JS. Inflamm Bowel Dis 2008;14:1425–1431 Immunosuppression & Skin Cancer Ultraviolet light P53 and other mutations Immunosuppressive Medications Inhibition of Antigen Presenting Cells Skin Cancer Systemic Immunosuppression HPV Adapted from Euvrard S. N Eng J Med 2003;348:1681-91 Thiopurines and Skin Cancer NMSC MELANOMA Long M. Gastroenterology 2012:143:390-9. Singh H Gastroenterology 2011:141:1612-20 Peyrin-Biroulet L. Gastroenterology 2011:141:1621-8 Peyrin-Biroulet L. Am J Gastroenterol 2012 doi: 10.1038/ajg.2012.181 Anti-TNF and Skin Cancer NMSC MELANOMA NR Long M. Gastroenterology 2012:143:390-9. Singh H Gastroenterology 2011:141:1612-20 Peyrin-Biroulet L. Gastroenterology 2011:141:1621-8 Peyrin-Biroulet L. Am J Gastroenterol 2012 doi: 10.1038/ajg.2012.181 Duration of Immunosuppressant Therapy for IBD and NMSC Pharmetrics Database - Nested case-control study Odds Ratio and 95% CI Recent and long term are not mutually exclusive Long M et al. CGH 2010;8 268-74 SIR and 95% CI Timing of Thiopurines and NMSC: Conflicting Results CESAME Cohort VA UC Cohort 12 12 10 10 8 8 7.06 6 6 5.19 4 4 2 2 0.76 0 Current Former Never Thiopurine Thiopurine Thiopurine 0 2.1 0.7 Current Former Thiopurine Thiopurine Peyrin-Biroulet L. Gastroenterology 2011:141:1621-8 Khan N. Am J Gastroenterol 2014: doi: 10.1038/ajg.2014.298 Clinical Questions • Is skin cancer risk increased by therapy? – Thiopurines – yes – Biologics - probably • If so, does the risk of continuing therapy outweigh the benefits? Maintenance of Remission After Withdrawal of Thiopurine Percent in Remission Continue Discontinue 100 80 60 40 20 0 0 24 48 72 96 Week Adapted from Van Assche et al. Gastroenterology 2008;134:1861–1868. CCEB Percent Continuing Infliximab Continuation of Infliximab After Withdrawal of Thiopurine Continue Discontinue 100 80 60 40 20 0 0 24 48 72 96 Week Adapted from Van Assche et al. Gastroenterology 2008;134:1861–1868. CCEB Risk of Second NMSC 2751 Medicare Beneficiaries with 1st NMSC 376 with 2nd NMSC Never use Thiopurines HR (95% CI) Reference 0.72 (0.31-1.70) Recent use <1 year current use 1.55 (0.88-2.75) >1 year current use 1.41 (0.92-2.16) Anti-TNF HR (95% CI) Reference 0.96 (0.34-2.70) 1.32 (0.63-2.78) 1.32 (0.74-2.34) Adjusted for other drug class, age, sex, median latitude, cumulative steroid exposure, and number of dermatology encounters in the year following surgery for the incident NMSC Scott FI. ACG 2014 Clinical Questions • Is skin cancer risk increased by therapy? – Thiopurines – yes – Biologics - probably • If so, does the risk of continuing therapy outweigh the benefits? – In this case – consider stopping thiopurine • Uncertain if risk will decline – Annual skin exam and regular use of sunscreen and hat Case #3 • 28 y.o. female with small bowel CD has been managed with azathioprine for the last 8 years suddenly develops abdominal pain and dysuria • CT demonstrates new inflammation of the jejunum that is abutting the bladder and pulmonary nodules • At surgery she is found to have a B cell non-Hodgkin lymphoma Questions • How would you manage her CD during therapy for NHL? • What is the prognosis of IBD during and following chemotherapy? • How will you manage her disease if she has a relapse after completing chemotherapy? Treatment of Lymphoma • EBV associated lymphoma can be initially managed with reduction in immunosuppression • Rituximab monotherapy is effective but with relatively high relapse rate • R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone) often employed Trappe R. Lancet Oncology 2012 Feb;13(2):196-206. Saha A. Clin Cancer Res May 15, 2011 17; 3056 Murukesan V. Drugs. 2012 Aug 20;72(12):1631-43. Course of Crohn’s Disease Following Treatment of Lymhoma 9 Patients Treated for NHL Chemo (n=7) Pred / Bud (n=3) AZA / 6MP (n=2) Ritux (n=1) MTX (n=1) Unk (n=1) 6/9 Relapse (2 w/in 1 year) 1/9 New Dx 9 years later SSA (n=1) No Rx (n=1) No Rx (n=1) 2/9 No Relapse Mourabet MA. Inflamm Bowel Dis 2011;17:1265-9 Clinical Course During Chemotherapy for Cancer 15 Patients with Active IBD at Time of Cancer Diagnosis Cytotoxic Chemo Cytotoxic + Hormonal Chemo Hormonal Chemo 5/5 IBD in Remission 4/4 IBD in Remission 1/6 IBD in Remission Axelrod JE. Clin Gastroenterol Hepatol 2012:10:1021-7 Course of IBD Following Chemotherapy for Cancer 69 patients in remission at time of initiation of therapy Axelrod JE. Clin Gastroenterol Hepatol 2012:10:1021-7 Questions • How would you manage her CD during therapy for NHL? – Stop immunosuppression if possible – Antibiotics, prednisone or budesonide if needed, in discussion with oncologist • What is the prognosis of IBD during and following chemotherapy? – Fairly favorable, particularly if receiving cytotoxic chemotherapy Questions • How will you manage her disease if she has a relapse after completing chemotherapy? CESAME Cancer diagnosed >2 years prior to cohort entry 50 59 Cancer diagnosed <2 years prior to cohort entry 40 26 Total with cancer prior to cohort entry Uterine Prostate NMSC 19 16 12 13 9 9 32 25 21 All sites 268 153 421 Colorectal Breast 90 85 Beaugerie L. Gut 2014;63:1416–1423. CEESAME Incident Cancer No immunosupressant Immunosuppressant 40 40.0 Incidence among 405 patients with history of cancer 30.0 19.4 20.0 16.3 9.3 10.0 4.8 3.1 0.0 Incidence per 1000-p-y Incidence per 1000-p-y 34.0 30 3.9 20 6 10 23.1 Recurrent cancer New cancer 13.2 0 <50 50-65 >65 HR = 1.7 (1.3 – 2.1) Any IS No IS (N=93) (N=312) HR NR (P>.05) Beaugerie L. Gut 2014;63:1416–1423. Anti-TNF Therapy for RA after Curative Breast Cancer Treatment Biologic Anti-TNF naïve (n=120) exposed (n=120) Total person-years Individuals with recurrent breast cancer 550 9 592 9 Rate/1000 p-y HR of recurrence cancer Adjusted HR 16 (7-31) Ref Ref 15 (7-29) 0.8 (0.3 – 2.1) 1.1 (0.4 – 2.8) Cohorts matched on age at diagnosis, county of residence, stage at diagnosis Adjusted for nodal status, surgery type, chemothrapy, comorbidities Raaschou P. Ann Rheumatol Dis. 2014:205745 Questions • How will you manage her disease if she has a relapse after completing chemotherapy? – Limited data on which to base recommendations – Intuition tells us to avoid chronic immunosuppression if possible – Role of vedolizumab to be determined Case #4 • 20 y.o. female was diagnosed with Crohn’s disease of the ileum. Presents to your ED complaining of increasing discomfort in the RLQ that is worse with meals. Mild bloating with meals. No fever. Mild-moderate RLQ tenderness. Prior colonoscopy had stenotic IC valve. Questions • Would you recommend an imaging test and if so, which test? • Does the risk of cancer influence your decision? • Would your decision be different if the patient was 60 y.o. rather than 20 y.o.? Comparison of sensitivity/specificity of imaging tests in IBD Herfarth H and Palmer L. Dig Dis 2009; 27: 278 Horsthuis K et al. Radiology 2008; 247: 64 Radiation dose associated with common medical imaging tests Herfarth H and Palmer L. Dig Dis 2009; 27: 278 Diagnostic Medical Radiation and Cancer Risk • CT is major source of diagnostic ionizing radiation – 63 million CT performed in USA in 2006 • Effects of radiation – DNA breaks, point mutations, chromosomal translocations • CT’s estimated to be responsible for 0.5-2% all cancers in USA Brenner DJ et al NEJM 2007; 357: 2277 Doll R et al. J Natl Cancer Inst 1981; 66: 1191 Radiation and IBD • 271 male, 280 female pts UC/CD – 13.6% CD, 4.5%UC > 40 mSV radiation – 70% radiation due to abdominal CT – Increased risk men, CD, IBD related surgery • 399 patients with CD – High exposure defined as CED >75 millisieverts (mSv) – an exposure level which has been reported to increase lifetime cancer mortality by 7.5%2 – CED >75 mSv is equivalent to 3750 standard X-rays – Number of CTs per patient increased from 0.3 CTs/pt (1992– 1995) to 1.3 CTs/pt (2005–2007) – 15.5% > 75 mSv radiation – Pts ileocolonic disease, steroids, infliximab, surgery at greatest risk Levi Z, et al. DDW 2008: #119; Desmond AN, et al. DDW 2008: #120; Panes J et al DDW 2008#121 Estimated Lifetime RadiationInduced Risk of Cancer on Age at Exposure Brenner DJ et al NEJM 2007; 357: 2277 Findings on APCTs in the ED Kerner C et al. Clin Gastroenterol Hepatol 2012;10(1):52-7 Questions • Would you recommend an imaging test and if so, which test? – In ED, patient will almost always will get CT. Always good to ask if CT needed • Does the risk of cancer influence your decision? – Yes-goal is to minimize long-term medical radiation exposure • Would your decision be different if the patient was 60 y.o. rather than 20 y.o.? – Same principles are relevant in both age groups (minimize medical radiation exposure), however risk of cancer is greater for the 20 year-old