Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
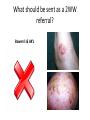
Dermatology GP Education & Networking Event 24th September 2014 Dr James Halpern Consultant Dermatologist Requested Topics • What should be sent as a 2WW referral? • Which patients should be referred to secondary care dermatology? • Allergy testing • How to use a Dermatoscope 2WW Referrals What should be sent as a 2WW referral? Melanoma & Lentigo Maligna What should be sent as a 2WW referral? SCC & Keratoacanthoma What should be sent as a 2WW referral? Rare skin cancers* *Cutaneous sarcomas, DFSP, angiosarcoma, KS, Merckle Cell, Cutaneous mets of internal malignancy What should be sent as a 2WW referral? BCC What should be sent as a 2WW referral? Bowen’s & AK’s What should be sent as a 2WW referral? Cutaneous Lymphoma Improving 2WW Referrals • Avoid referring BCC’s • Mole checks, dysplastic naevi • Children • Multiple naevi • Inflammatory referrals Referrals to Secondary Care What not to refer • Cosmetic removal of benign skin lesions – moles, SK’s, cysts etc. • Laser hair removal • Treatment of acne scarring • Molluscum Contagiosum • ‘Simple’, low grade or minor rashes What to refer • All suspected skin cancers: – – – – Melanoma, SCC, BCC, rare skin cancers Cutaneous lymphomas Cutaneous deposits of internal malignancy Pre-malignant skin disease • simple AK’s can be treated in primary care – Paraneoplastic rashes What to refer • Surgical referrals: – All skin cancers and pre-malignant disease requiring a biopsy or excision – Lesions that are to large to remove in primary care – All inflammatory rashes which require a biopsy – Paediatric biopsies – Patients on Warfarin, with pacemakers or other CI’s eg. Myasthenia Gravis What to Refer • Moderate or severe inflammatory rashes that: – require systemic therapy, patch testing, phototherapy etc. – Have not responded to topical therapies – Are having a significant impact of patients quality of life • All bullous disorders except insect bites What to Refer • Acne that: – Is scarring – Failed on standard therapies – Significant psychological impact • Hyperhidrosis that: – Has failed antiperspirants – Significant psychological impact What to Refer • Rare skin disorders: – – – – – Genetic skin disease Tropical skin disease Photodermatoses Psychiatric skin disease HIV & immunosuppression related skin disease – Pregnancy related rashes – Cutaneous manifestations of connective tissue disease and vasculitis – Genital skin disease • Disorders of the hair and nails Urgency of Referrals • 2WW – Cancer only • Routine / C&B – 12 Weeks: • BCC • Inflammatory referrals eg. eczema, psoriasis • Very Urgent / Life Threatening referrals: • We do not offer a same-day / urgent / On-call / Advice referral service • If you have a life or limb threatening skin problem eg. TEN – Within working hours call dermatology secretaries – OOH send to A&E / MAU – 24/7 on-call dermatologist at Birmingham Skin Centre (City Hospital) • Please Note – A&E if only for those with life threatening skin disease associated with systemic upset. A&E does not have access to dermatologists and can not expedite dermatology appointments Semi-Urgent referrals • The most challenging group of patients to know what to do with: – Not sick enough to justify admission to hospital or same day referral – Can not wait 12 weeks to be seen • From my perspective: – Very difficult to ‘ring-fence’ slots for – Great variability in number and quality of referrals – Causes a lot of frustration for GPs and us! • Good examples: New diagnosis bullous pemphigoid, stable suberythrodermic rashes, vasculitic rashes • Bad examples: Patients with stable skin disease who keep consulting yourself / A&E, ‘unknown’ rashes in systemically stable well patients • Send urgent fax and we will triage – we will try our best! Example of a Good Referral • Concise • Relevant • Appropriate Allergy Testing When do you Allergy Test? • Type 1 (immediate reactions) • Suspected allergic contact dermatitis •Atopic eczema •Urticarias •Generalised itching •Unknown rashes Atopic Eczema and Allergy • 99% of atopic eczema in not due to allergy • Serum specific IgE’s (RAST) and prick testing is of no use in atopic eczema • Dermatology does not offer allergy testing for children with eczema – Do NOT refer for this Atopic Eczema and Food Allergy • Very rare • Presents at weaning • ‘All over’ eczema, not confined to flexural areas • Best test is an exclusion diet and food diary +/dietician input • No role for allergy ‘testing’ Urticaria and Allergy • 99% of urticaria is idiopathic in nature • There is no role for allergy testing in the investigation of urticarial rashes Type 1 Allergic Reactions - Anaphylaxis • Immediate (within 2 hours) • Often due to food • May be life threatening • Investigated with Prick Testing • NOT Dermatology • Refer children to Dr Ferdinand & adults to clinical immunology Type IV – Allergic Contact Dermatitis • Occurs 72 hours after exposure of a substance on the skin and presents as an eczematous reaction • Commonly Nickel, Hair Dye (PPD) or Occupational • Investigated by Dermatology with patch testing Dermoscopy What is Dermoscopy? • The use of a dermatoscope to diagnose skin lesions • A dermatoscope gives 10x magnification and polarised light What is Dermoscopy? • Used to diagnose melanoma • Can distinguish naevi from dysplastic naevi and melanoma • Used to diagnose benign skin lesions • Can distinguish naevi from seb keratosis and vascular lesions Diagnosing skin lesions 90% History 5% Examination 5% Dermoscopy Reticular Pattern • Most common pattern in melanocytic naevi • Also seen in melanoma, lentigo simplex & dermatofibroma Typical regular reticular network seen in a benign naevus Reticular Pattern Atypical reticular network seen in a melanoma-in-situ Note: Asymmetry Variable thickness of network Variability of colour Globular Pattern • Numerous, variously sized, round/oval structures with brown/gray/black colour • Seen in benign naevi, atypical naevi, congenital naevi and seborrhoeic keratosis Note variation in size and colour of globules in this atypical compound naevus Cobblestone Pattern • Similar to the globular pattern, numerous closely aggregated, larger, angular globules resembling a cobblestone • Often seen in papillomatous naevi Typical cobblestone pattern in this very benign looking compound naevus Homogenous Pattern • Diffuse brown/gray/blue/black colour with an absent network • Seen in blue naevi, benign naevi, atypical naevi, melanoma, haemangiomas, tattoos and pigmented BCC A very typical pattern seen in a benign blue naevus Homogenous Pattern Dark red/black homogenous seen in subcutaneous haemorrhage Homogenous pattern with reddish halo seen in a melanoma metastasis Starburst Pattern • Pigmented streaks in a radial pattern at the edge of the lesion • Classical of Spitz naevi, occasionally melanomas can present with this pattern Starburst pattern seen in a spitz naevus Parallel Pattern • Seen with naevi on acral skin Typical parallel pattern seen in a benign acral naevus Parallel Pattern Parallel-ridge pattern seen in acral melanoma in situ Note the pigmentation crossing the ridges and variability within the pigmented ridges Multicomponent Pattern • Combination of 3 or more other patterns previously described • Suggestive of melanoma but also seen in benign naevi, BCC and non-melanocytic lesions Highly atypical network with multiple colours, asymmetry, central white halo and multiple network types seen in a melanoma Lacunar pattern • Several to numerous smooth bordered, round red structures • Seen in haemangiomas and angiokeratomas Typical haemangioma Should you buy a dermatoscope? • Useful in diagnosing benign skin lesions • May reduce unnecessary referrals to secondary care • Good ones cost ~£1000 • Difficult learning curve and easy to become deskilled • Overconfidence/reliance can be dangerous Questions?