Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
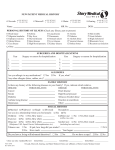
Medical History Questionnaire Name:_____________________________________________________________ Date of Birth: _____/_____/________ The reason for your visit: _____________________________________________________________________________ How long has this been present? _________________What have you tried to treat it? ____________________________ Drug Allergies: ______________________________________________________________________________________ PERSONAL DERMATOLOGIC HISTORY *Please check if you have a history of: ☐ Skin Cancer Which Type? ☐ Melanoma - When? ______________ Location? ___________________ ☐ Basal Cell Cancer - When? ______________ Location? ___________________ ☐ Squamous Cell Cancer - When? ______________ Location? ___________________ ☐ Actinic Keratosis (Precancerous Skin Growth) ☐ Eczema ☐ Psoriasis ☐ Lupus ☐ Scarring Acne ☐ Other dermatologic condition(s) ____________________________________________________________ MEDICAL HISTORY *Please check if you have a history of: ☐ Allergies/Sinusitis ☐ Artificial Heart Valve ☐ Asthma ☐ Bleeding Disorder ☐ Cancer (other than skin cancer) Which type? ______________ ☐ Cataracts ☐ Cold Sores (Herpetic Infection) ☐ Congestive Heart Failure ☐ Depression ☐ Diabetes ☐ Diabetes Mellitus ☐ Emphysema/COPD ☐ Epilepsy ☐ GERD/(Reflux Disease) ☐ Glaucoma ☐ Heart Arrhythmia ☐ Heart Disease ☐ Hepatitis ☐ High Cholesterol ☐ HIV or AIDS ☐ Hypertension ☐ Irritable Bowel Syndrome ☐ Mitral Valve Prolapse ☐ Organ Transplant ☐ Osteoarthritis ☐ Osteoporosis ☐ Rheumatic Fever ☐ Rheumatoid Arthritis ☐ Stomach Ulcer ☐ Thyroid Disease ☐ Tuberculosis ☐ Other _______________________ SOCIAL HISTORY Do you wear sunscreen regularly? Yes No Do you smoke? Yes No FAMILY HISTORY Use tanning beds? Yes No Drink alcohol? Yes No Use drugs? Yes No *Do any family members suffer from the following? Condition: Family Member (Relationship) Skin Cancer (other than melanoma) Melanoma Asthma/Eczema/Seasonal Allergies Psoriasis For Women: Are you currently pregnant OR actively trying to get pregnant OR breastfeeding? Are you interested in cosmetic products or procedures? Have you had any cosmetic procedures in the past? Yes Yes No No Yes No Anything specific? ________________________________ Were you happy with the results Yes No