Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Behçet's disease wikipedia , lookup
Germ theory of disease wikipedia , lookup
Globalization and disease wikipedia , lookup
Infection control wikipedia , lookup
Neonatal infection wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Schistosomiasis wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
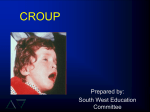
Croup and Bronchiolitis Karen D. Sawitz, MD St. Barnabas Hospital Department of Pediatrics The Pediatric Airway Croup - Epidemiology • • • • • • 15% of respiratory visits in children Most common cause of stridor in children Primarily 1 to 6 years, mean 18 months Boys > girls (1.5 to 1) Peak incidence in US 5 per 100 in 2nd yr Predominates during fall and winter Croup - Etiology • • • • • • Viral-mediated inflammatory condition AKA laryngotracheitis, laryngotracheobronchitis Affects vocal cords and subglottic airway 65% due to parainfluenza types 1, 2, 3 Most hospitalized cases are type 1 Others: adenovirus, RSV, varicella, measles, HSV, enteroviruses, Mycoplasma pneumoniae, and influenza A and B • Transmitted by inhalation via nasopharynx Croup – Clinical Presentation • Prodrome: rhinorrhea, pharyngitis, low-grade fever, +/- cough over 12-48 hours • Gradual development of barking cough, hoarseness, varying inspiratory stridor +/- fever • May develop more severe obstruction with inspiratory stridor at rest, increased HR/RR, nasal flaring, retractions, progressive hypoxia and cyanosis • Symptoms may worsen at night/with crying • Mild course 3-7 days, more severe 7-14 days Westley Croup Score Inspiratory Stridor • None (0 points) • When agitated (1 points) • On/off at rest (2 points) • Continuous at rest (3 points) Retractions • None (0 points) • Mild (1 points) • Moderate (2 points) • Severe (3 points) Air Movement/Entry • Normal (0 points) • Decreased (1 points) • Moderately decreased (2 points) • Severely decreased (3 points) Cyanosis (Color) • None (0 points) • Dusky (1 point) • Cyanotic on room air (2 points) • Cyanotic with supplemental oxygen (3 points) Level of Alertness (Mentation) • Alert (0 points) • Restless or anxious (1 points) • Lethargic/Obtunded (2 points) <4 Mild 5-6 Mild-Moderate 7-8 Moderate 9-10 Severe ©2008 UpToDate® Croup – Differential Diagnosis • Infectious – Acute epiglottitis – Bacterial Tracheitis – Retropharyngeal or peritonsillar abscess • Noninfectious – Angioneurotic edema – Foreign body aspiration Pediatrics in Review January 2001 Croup - Treatment • Home Management – Cool mist or night air – Steam (vaporizer or from shower) – Keep child calm • Primary Care/ER Setting – Cool mist (may precipitate bronchospasm) – Steroids: oral or IM dexamethasone 0.6 mg/kg single dose (half-life 36-52 hours) – Racemic epinephrine in severe cases: 0.25-0.5 ml in 2.5 ml saline by nebulizer Croup - Treatment • Criteria for discharge after Racemic Epi – Observation for 3-4 hours – No stridor at rest – Normal air entry – Normal color – Normal level of consciousness – Have received a dose of dexamethasone Croup – Indications for Admission • • • • • • • Suspected or actual epiglottitis Cyanosis/hypoxemia/pallor Stridor at rest or progressive stridor Respiratory distress Depressed sensorium Restlessness Toxic appearance Nelson Textbook of Pediatrics 16th Edition 2000 Bronchiolitis - Epidemiology • Most common lower respiratory tract infection in infants • Most common etiology is RSV, most cases between December and March (75% of cases under 2) • More common in crowded living conditions and smoke exposure • Breastfeeding appears to confer a protective advantage • Most severe symptoms in those under 2 • >50% affected by age 1, 80-90% by age 2, 40% have LRTI • No permanent RSV immunity, reinfections common • 1-2% require hospitalization • 90,000 hospitalizations annually (80% under 1 year) • Deaths 4500 (1985) 510 (1997) 390 (1999) • Cost of hospitalization infants under 1 year: $700 mil/yr • More likely to have respiratory problems when older RSV Spread • • • • Humans only source of infection Direct or close contact with secretions Large-particle droplets <3 ft or fomites May persist hours on surfaces or 30 minutes on hands • Viral shedding 3-8 days or longer • Incubation period 2-8 days (4-6) Bronchiolitis – Clinical Features • Pathophysiology – Marked inflammation, edema, necrosis of smaller airway epithelial cells – Increased mucus production – Bronchospasm • Clinical Features – – – – – – Rhinitis, tachypnea, wheezing, cough, crackles Accessory muscle use and nasal flaring Apnea, grunting, cyanosis Poor feeding, difficulty sleeping, fussiness Tachycardia and dehydration may occur Natural course 7-10 days, peak on day 4 Bronchiolitis – Diagnosis & Testing • Clinical diagnosis on basis of H & P • Laboratory and radiologic studies should not routinely be ordered per AAP • NP swab for RSV ELISA may be used eg for cohorting • CXR to exclude other Dx, or if not improving as expected • Concurrent SBI is rare, may need to be ruled out in febrile young infants (UTI) Bronchiolitis – Risk Factors for Severe Disease • Age under 6-12 weeks • History of prematurity esp < 28 weeks GA • Underlying cardiopulmonary disease – Chronic lung disease (BPD, CF) – Complex congenital heart disease – Congenital airway abnormalities • Immunodeficiency • Severe neuromuscular disease Bronchiolitis - Management • Mainstay: supportive care (hydration, oxygenation, nasal suction, respiratory support if needed) • No routine bronchodilator use – may improve symptoms short-term but no effect on length of illness or LOS; potential for harm (SE, cost) • No routine corticosteroid use – no benefit in RR, O2 sat, LOS though given to 60% of inpatients • No routine use of ribavirin – variable results, may be appropriate for severely ill infants • Antibiotics only if indication of concurrent bacterial infection Bronchiolitis – Criteria for Admission • • • • • • Persistent hypoxia Respiratory distress Inability to tolerate fluids Inability to ensure close follow-up Infants under 2 months of age - consider Premature infants - consider RSV Bronchiolitis - Prevention • Palivizumab (Synagis®) prophylaxis for selected infants under 24 months – 15 mg/kg IM monthly November-March • Hand washing • Avoiding passive smoke exposure • Promotion of breastfeeding Criteria for Passive Immunization • ≤24 mos old with – CLD on therapy in 6 mos before start of RSV season – Hemodynamically significant congenital heart disease • ≤32 weeks GA even without CLD – <28 wks GA during first season/≤12 mos at start – 29-32 wks GA up to 6 mos of age at start of season • 32-35 wks GA up to 3 mos with ≥1 risk factor: – Day care attendance or – Sibling under 5 years of age • <34 wks GA with airway abn or neuromuscular dz Source: AAP Red Book 2009 Source: AAP Red Book 2009 Source: AAP Red Book 2009