Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
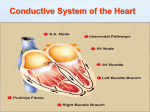
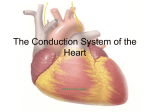
Bundle Branch and Fascicular Block Chapter 13 Robert J. Huszar, MD Instructor Patricia L. Thomas, MBA, RCIS Outline • • • • Student Demonstration of Axis Electrical Conduction system and Blood supply Physiology of the Electrical Conduction System Pathophysiology of the Bundle Branch and Fascicular Blocks • Right Bundle Branch Block • QRS Complexes • Left Bundle Branch Block A&P of the Electrical Conduction System • RBB runs down the right side of the IS to conduct the electrical impulses to the RV. • LBB short, thick, flat (main stem) conducts the electrical impulses to IS & LV. It is divided into two parts: – LAF conducts electrical impulses from the main stem to the anterior and lateral walls of LV. – LPF conducts electrical impulses to the posterior wall of the LV. Blood Supply to the Electrical Conduction System • Anterior two thirds of the interventricular septum is supplied by the left anterior descending CA. • Posterior third of the septum is supplied by the posterior descending CA. • AV Node and Proximal Bundle of His is the AV node artery. • Distal Bundle of His, RBB, Main stem of LBB and Lt Anterior Fascicle are supplied by the LAD septals. • Left Posterior Fascicle is supplied by the LAD and PDA. Intact viable vs. Not Intact or viable • IVIS-is capable of conducting an electrical impulse and depolarizing from left to right producing and initial small q or r wave in the QRS complex in V1,V2 & V6. Resulting synchronous depolarization with the smaller RV buried in that generated by the LV. • NVIS- results because of some form of Heart Disease, (MI) is unable to conduct an electrical impulse and depolarize normally ( absence of a q or r wave) Steps for Normal Depolarization The electrical impulse progress through the RBB and LBB and Fascicles simultaneously. • Depolarization of IVS • Synchronous Depolarization of RV & LV • Note: The electrical activity generated by the depolarization of the smaller RV is buried in that generated by the LV. Depolarization of Septum • Depolarization of the Interventricular Septum of the endocardial to epicardial of the ventricular wall is call the Ventricular Activation time (VAT) or the Preintrinsicoid Deflection (IDT), the duration of the Intrinsicoid Deflection or the R peak time. VAT Measurement • Onset of the QRS complex to the peak of the last R wave in the QRS complex. • Normally less than .04 second in V1 or V2 or less than .06 second in V5 and V6. • RBBB & RVH -the VAT is prolonged in leads V1 & V2 • LBBB & LVH-the VAT is prolonged in Leads V5 & V6 Pathophysiology of the BB and Fascicular Blocks • Ischemia heart disease • Acute Mi • Idiopathic degenerative disease of Conduction system • Cardiomyopathy • LVH • Aberrant ventricular conduction • Miscellaneous causes such as – Acute or chronic HF, PE, AoValve Disease, Tumors, Trauma, Potassium overdose Right Bundle Branch Block • The electrical impulses are prevented from entering the RV directly because of disruption of conduction system. • RBBB present with intact viable IVS • RBBB present without intact viable IVS • ECG characteristics of the two RBBB’s differ significantly • Compare Leads 1 & V1, V6 RBBB • Impulses travel down the LBB in to the IS & LV-(Normal) • IS to right to enter the RV after a short delay • LV depolarize in normal way: first the septum from left to right • Then the LV from right to left • LV depolarization • RV depolarizes in a normal direction • Delay results in a wide bizarre shape/appearance • .12 seconds or greater (complete) • .10 and .11 seconds (incomplete) Pathophysiology of the Left Bundle Branch Block • The electrical impulses are prevented from entering the LV directly because of the disruption of conduction of the electrical impulses through the LBB. • LBBB present with intact viable IVS • LBBB present without intact viable IVS • ECG characteristics of the two LBBB”s differ significantly • Compare Leads 1, aVL,V1, V3, V5,V6 • Complete LBBB - QRS >.12 • Incomplete LBBB - QRS .10-.11 sec. LBBB • Impulses travel down the RBB into the RV (normal) • Impulse travels slowly across IS from Right to Left (abnormal) • Depolarization of the RV (normal) • Depolarization of the LV (normal direction) • Depolarization of the LV results from the impulse from the right instead of the LBB • The LV depolarizes behind schedule • QRS > .10 seconds • .12 or greater complete THE END OF CHAPTER 13 Hauszar Robert, Basic Dysrhythmias, Interpretation & Management, Third Edition, Mosby, Inc. 2002, pp. 271-288.