Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Jatene procedure wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
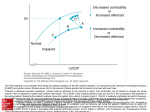
The Cardiac Cycle Work Output of the Heart Preload, Afterload and Contractility Regulation of Heart Function – The Frank Starling Mechanism Measurement of Cardiac Output During systole, blood accumulates in the atria. At end systole, the higher pressure forces open the AV valves causing rapid ventricular filling. This lasts about 1/3. In the middle 1/3, there is minimal flow. In the last 1/3, the atria contracts to deliver up to 20% of the total ventricular volume. At the start of systole, the intraventricular pressure rises which closes the AV valves. For approximately 0.02 to 0.03 seconds, the pressure continues to rise but is less than that required to open the semilunar valves. This is called isovolumic contraction because the ventricular volume does not change. Once the semilunar valves open the ejection phase begins. About 70% of the total blood ejected occurs in the first 1/3. This is called the rapid ejection period The final 30% empties in the next 2/3 and is called the slow ejection period. At end-systole, ventricular relaxation begins suddenly and causes intraventricular pressure to fall rapidly. The semilunar valves close once its pressure is greater than intraventricular pressure. For 0.03 – 0.06 seconds the muscle continues to relax, pressure continues to fall but no filling occurs because the AV valves are still closed. This is the period of isovolumic relaxation. After the aortic valve opens, blood enters the aorta, stretching it and causes the pressure to rise to 120 mmHg. An incisura occurs just before the aortic valve closes from a short backward flow of blood. During diastole, the aortic pressure slowly falls as blood flows out to the venous side. The stroke work output of the heart is the amount of energy converted to work per beat. Two forms of work output: Volume pressure (external) work: moving blood from the low pressure veins to high pressure arteries. Kinetic energy of blood flow: accelerate the blood to its velocity of ejection. RV external work is 1/6 of the LV because of the six fold difference in systolic pressure. Understand how the systolic and diastolic pressure curves are derived. By combining the end diastolic and systolic curves, the volumepressure diagram can be defined. The area inside the VP diagram is the EW. Preload can be described as the stress experienced at end-diastole Preload=(EDP x EDR)/2w Thus, preload represents all the factors that contribute to passive ventricular wall stress (or tension) at end diastole. This means that EDP (P) or EDV (R) contribute to, be should not be equated to preload. Laplace’s Law can be used to describe afterload as ventricular stress during systolic ejection. Therefore, stress=TP x R/2w Afterload represents all the factors that contribute to total myocardial wall stress (or tension) during systolic ejection. Arterial pressure and TPR contribute to afterload but should not be equated with afterload. Focusing on wall stress is important Metabolic cost is related to the wall tension The greater the tension, the greater the oxygen demand. Physiological and therapeutic regimens reduce wall stress and restore oxygen supply and demand. The relationship among P, R and w provides a clear physiological explanation for the different patterns of hypertrophy and remodelling. Contractility is the peak isometric force generated at a given preload and afterload. A increase in contractility causes incremental increases in developed force and velocity of contraction. Results from different degrees of binding between myosin and actin filaments. This is dependant on the intracellular calcium concentration. The amount of blood pumped by the heart is determined by the rate of blood flow from the veins (venous return). The intrinsic ability of the heart to adapt to increasing volumes of blood is the FrankStarling mechanism. With the extra delivery of blood, the cardiac muscle contracts with greater force because of improved actin/myosin interaction. The ventricular function curve is a way of expressing the Frank-Starling mechanism. Increases in atrial pressure causes an increase volume and strength of contraction which causes an increase in cardiac output. Suppose blood flow is Q (ml/s) and q mg of dye is injected. If the concentration of dye is continually measured farther downstream, a curve of the dye concentration, c, is recorded as a function of time, t. The amount of dye at point B between the time t1 and t2 will be q = cQ(t2-t1). Therefore, Q = q/(t2-t1)c c is properly defined as an integral with limits of t1 to t2. Clinically, we use the temperature as the indicator instead of a dye. Therefore, we can adjust the equation to: Q V (TB TI ) K 1 K 2 t2 TB(t )dt t1 What would the curve look like in a high cardiac output state? Low? What is the effect of tricuspid regurgitation? The Cardiac Cycle Work Output of the Heart Preload and Afterload and Contractility Regulation of Heart Function – The Frank Starling Mechanism Measurement of Cardiac Output Wall Stress An increase in wall stress achieved by either increasesd LV size or intraventricular pressure will increase myocardial oxygen uptake. This is because a greater rate of ATP use is required as the myofibrils develop greater tension. Wall Stress, Preload and Afterload Preload can now be defined as the wall stress at the end of diastole and therefore at the resting maximal resting length of the sarcomere. Afterload, being the load on the contracting myocardium, is also the wall stress during LV ejection. Preload The stretch of the individual sarcomere regulates the performance of the heart. Afterload Peak systolic wall stress reflects the three major components of the afterload-peripheral resistance, arterial compliance, and peak intraventricular pressure. This is the force against which muscle contracts. Contractility This is the intrinsic ability of the heart muscle to generate force and to shorten. It is manifest as the rate of pressure development and shortening from any preload. Ventricular Function Curve The dependancy of stroke volume on preload was described more than 100 years ago by Otto Frank and E.H. Starling and since then has been called the Frank-Starling mechanism. Using this relationship between preload and stroke volume or stroke work, a ventricular function curve can be consructed by plotting stroke work at various levels of preload.