Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
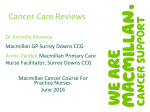
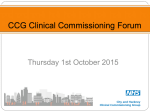
• Dr Jaimin Patel • Macmillan GP- Croydon • GP Appraiser and Referral triager, • Prostate Cancer Project lead GP Time Subject Speaker 13.30 - 14.00 Registration and light lunch 14.05 - 14.20 Welcome Setting the scene-Macmillan Resources, Croydon Priorities Dr Jaimin Patel, Croydon Macmillan GP 14.20 - 14.55 Early Detection of Cancer- NICE NG12 Changes in Suspected Cancer : recognition and referral, Pan London Strategy Dr Ishani Patel 14.55- 15.25 Acute Oncology Services at CUH with Q&A Dr Tuck-Kay Loke Clinical Head of Service for Cancer & Dr Nicola Beech Acute Oncology Service at CHS NHS Trust 15.25 - 15.40 COFFEE 15.40 – 16.25 Colorectal - New Nice Update on Lower G.I. and direct access proctology Q&A Mr Muti Abulafi Lead Colorectal Surgeon at CHS 16.25 – 16.50 Urology- NICE changes & and local pathway update- PSA & Haematuria Mr Babbin John Urologist at CHS 16:50-17.00 Electronic referral update Omar Ali & Jill Anderson CHS Transforming Cancer Services Team, Healthy London Partnership Early Diagnosis of Cancer and Quality Improvement FACTS 2 million people living in the UK with cancer, this number will double by 2030 Around 25% people in the UK face poor health or disability after cancer treatment Half of people diagnosed with cancer now survive their disease for at least 10 years These figures highlight the importance of primary care health care professionals being equipped to support these groups As of the end of 2010, around 9,100 people in Croydon CCG were living with and beyond cancer up to 20 years after diagnosis. This could rise to an estimated 17,700 by 2030 The Importance of early Detection of Cancer and Screening Why is Improving Cancer Survival Important? •Cancer is leading cause of premature mortality for ) many CCGs •Under 75 mortality for all cancers part of CCG Indicator Pack • 1 year survival included in CCG 2015/16 Delivery Dashboard -QUIPP • As people living longer the proportion of people getting cancer is increasing •Emergency presentations costly & poorer outcomes •Improve Patient Experience “ Safety Netting • The government has set a target for saving 5,000 lives a year through earlier diagnosis of cancer by 2014. Diagnosis of cancer in primary care is beset by three interrelated challenges – the relative infrequency of cancer, initial nonspecific presentation of symptoms which occur relatively commonly, and variable time course of evolution of clinical features. Safety netting is one of the most important “tools” that GPs and their practices can use for patients whose presentation is not initially recognised as cancer, ensuring that they are re-evaluated in a timely and appropriate manner. Cancer Strategy Development and Implementation Group • • Quality Premium: For 2015/16 the CCG agreed a local Quality Premium relating to increasing the % of cancers detected at stages 1 and 2. The data available at the time showed the following performance of the CCG against national performance 2012 Performance CCG 31.6% (HSCIC : CCG Indicator:1.18) National 41.6% (HSCIC: CCG Indicator 1.18) The earlier detection of cancers improves the outcomes for patients in terms of treatments that can be provided at early stages so increasing positive outcomes for patients in success of treatment outcomes and increased levels of survivorship so decreasing the levels of mortality. Cancer Strategy Development and Implementation Group • In place for Croydon CCG - CHS, TCST, Croydon CCG, Macmillan GP , CRUK , Public Health. • Key Areas defined in the strategy are : • Early Detection • Prevention • Cancer Screening • • • • Reducing Inequalities and variations Patient Experience Living with and beyond cancer End of life care Early stage cancer treatment significantly less expensive Treatment Costs Stage 1 Stage 4 Colon Cancer Rectal Cancer Lung Cancer Ovarian Cancer £3,372 £4,449 £7,952 £5,328 £12,519 £11,815 £13,078 £15,081 Macmillan GPs influence change rather than provide a ‘cancer service’ 5.6 Cancer 5.6.1 Prevalence and incidence Indicator MD Y TNH WS S NAS PRY ECR Cro Lon Eng N Ad Sels Cancer diagnosed (since 1st April 2003) (all ages) 1.26 % 1.46 % 1.62 % 1.95 % 2.21 % 1.34 % 1.62 % 1.46 % 2.10 % 1.12 % 2.56% New cancer cases (incidence per 1,000) 2.77 2.96 4.19 5.22 5.06 3.47 3.89 3.28 4.90 4.98 5.38 Indicator MD Y TNH WS S NAS PRY ECR Cro Lon Eng Targ et N Ad Sels Cervical screening coverage (last 5 yrs) (ages 25-64) 73.3 % 77.5 % 79.1 % 79.3 % 80.6 % 73.2 % 76.7 % n/a n/a 80 77.7 % Cervical screening coverage (excl exceptions) (CS002) 78.9 % 80.0 % 80.9 % 84.8 % 80.4% 83.8 % 79.2 % 81.0 % 80.1 % 81.9 % 80 80.7 % Breast screening coverage (last 3 years) (age 50-70) 59.3 % 59.8 % 63.8 % 87.7% 67.4 % 68.2 % 60.3 % 63.4 % 64.1 % 72.1 % 80 59.2 % Bowel screening coverage (last 2.5 years) (age 60-69) 43.7 % 43.9 % 71.4% 54.0 % 55.5 % 58.9 % 45.7 % 51.2 % 49.5 % 58.8 % 39.9 % 62.1% MD Y TNH WS S NAS PRY ECR Cro Lon Eng N Ad Sels Total two-week wait referrals (per 1,000) Referrals with suspected breast cancer 13.7 18.1 18.1 23.2 22.8 16.0 18.3 17.0 21.7 16.8 28.0 1.8 3.1 2.7 3.4 3.5 2.4 2.8 3.6 4.0 3.6 3.3 Referrals with suspected lower GI cancer 3.1 2.8 3.9 4.6 4.0 2.4 3.4 3.1 4.0 5.0 4.3 Referrals with suspected skin cancer 2.0 2.5 3.4 6.0 4.1 2.9 3.4 3.4 4.0 4.0 7.1 8.9% 6.7% 10.5 % 8.7% 9.2% 10.4 % 9.1% 8.0% 10.2 % 6.4% 8.9% 50.6 % 41.0 % 54.6 % 46.2 % 51.2 % 54.1 % 50.2 % 49.1 % 48.6 % 31.6 % 48.0% Targ et 5.6.2 Cancer screening The targets shown are the national targets for coverage. 5.6.3 Cancer waiting times Indicator Targ et 5.6.3.1 Two-week wait (TWW) referrals The rates are not age standardised, and are per 1,000 population per year. 5.6.3.2 Conversion rate Conversion rate (% of TWW referrals with cancer) 5.6.3.3 Detection rate Detection rate (new cases which are TWW referrals) 43.9 New cancer risk thresholds Most significant change :are much better grounded on epidemiological evidence from primary care, rather than the old guidelines that relied predominantly on secondary care data. This new evidence enabled the guideline developers to identify the patterns of symptoms, signs, and simple investigations associated with specific levels of risk of an undiagnosed cancer. It recognises the importance of combinations of symptoms in predicting risk of cancer. The guidelines also account better for age and smoking as the most important underlying risk factors when considering certain common symptoms. For example, someone aged >40 years with abdominal pain and weight loss should be investigated urgently for colorectal cancer. If they are aged >60 years, they should also be investigated for pancreatic cancer by CT or ultrasound. There is a section relating to non-specific features of cancer including appetite loss, weight loss, and fatigue. Weight loss is associated with a 7% overall risk of cancer but this includes colorectal, gastrooesophageal, lung, prostate, pancreatic,and urological cancers. Leadership Commissioning Service redesign What do Macmillan GPs do? Education Communication Variation in Awareness of Increased Risk Early Diagnosis is a complex, multifaceted challenge The NAEDI hypothesis Developing practical solutions… Developing practical solutions… Starting different conversations… “ What could Primary Care be doing to Reduce Cancer Risk? •Delivery of Very Brief Advise for Smoking (VBA) •Delivery of Alcohol Advise opportunistically & at all Health Checks •Signpost & increase uptake of smoking & weight management services •Implement Primary Care Cancer Screening Best Practice Guidance to Promote Uptake What can Primary Care do to Improve Access? • •Support national BCOC & locally tailored campaigns & encourage presentation of symptomatic population • •Patient Participation Groups & User Groups supporting national, local & tumour specific campaigns • •Case Finding & Review High Risk Patients (Proactive Care) • •Increase awareness of Cancer Screening Programmes to over 70s when delivering Flu and Shingles vaccines ...BIG POTENTIAL Small commuity 20 GPAs & 150+ Mac GPs Reaching around 16,000 GPs in the UK Influencing better cancer care for half the UK population Reducing Delays in Primary Care Education •Annual Audit & share outcomes at Practice Meeting •All PCHT attend cancer training to include non-clinical staff •Use of Practice Profiles to reduce variation in cancer outcomes Raising Awareness •Cancer regular agenda item at Practice Meetings •Endorse screening communications, clean lists, flag & ensure DNAs followed up •Use of Decision Support Tools •Agree & implement Safety Netting Protocols Developing Practice •Practice Nurses to raise cancer awareness at LTC appointments •Upload revised 2ww referral forms •Use pan-London ED colorectal, gynaecological & lung pathways •Agree & Implement Safety Netting Protocols Resources & Data Revalidation Toolkit • http://www.macmillan.org.uk/Documents/AboutUs/Health_professionals/RevalidationToolkit.p df Rapid Referral Guidelines • http://www.macmillan.org.uk/Aboutus/Healthandsocialcareprofessionals/Macmillansprogramm esandservices/Earlydiagnosisprogramme/Earlydiagnosisprogramme.aspx Detecting Cancer Earlier in Primary Care: Using Cancer Decision Support Tools to improve the management of cancer in primary care • [email protected] • •Primary Care Facilitator Programme http://www.cancerresearchuk.org/health-professional/early-diagnosis-activities/primary-careengagement-facilitator-project • •Talk Cancer http://www.cancerresearchuk.org/health-professional/prevention-and-awareness/talk-cancer • •Cancer Data Cancer Commissioning Toolkit - http://www.ncin.org.uk/cancer_information_tools/cct • Public Health Profiles - http://fingertips.phe.org.uk/profile/ • http://www.cancerresearchuk.org/cancer-info/cancerstats/local-cancer-statistics/