Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
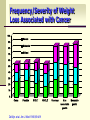
Nutrition in Cancer Pranithi Hongsprabhas MD. Weight Loss in Cancer Patients 50% of CA pt lose wt ~ 70% of terminal stage CA pt Wt loss is prognostic significant Kondrup AJCN 2002, De Wys et al. Am J Med 1980, Andreyev et al. Eur J Cancer 1998 Frequency/Severity of Weight Loss Associated with Cancer 100 Severe 90 Moderate 80 Minimal 70 60 50 40 30 20 10 0 Colon Prostate SCLC DeWys et al. Am J Med 1980;69:491 NSCLC Pancreas Non measurable gastric Mesurable gastric Cancer Cachexia: Myth Anorexia-cachexia syndrome is due to the host lack of appetite and or starvation Anorexia-cachexia happens because of tumor consumes the host nutrients Progression of Cancer-induced Weight Loss Initiating Factors Normal Mild Weight Loss/ Anorexia Metabolic Changes Moderate Weight Loss/ Reduced activity Below IBW Severe Weight Loss/ Cachectic State Muscle Wasting Obvious Death Reduced Survival Cancer Cachexia Syndrome of combined physiologic, metabolic and psychological factors Manifestations: anorexia progressive involuntary wt loss, wasting, tissue depletion Fatigue, poor performance Anemia More advance disease: higher risk of wt loss Metabolic Response to Starvation Hormonal Response Starvation Energy Expenditure in to Starvation Nitrogen Excretion (g/day) Hormone 12 Source Change in Secretion Norepinephrine Sympathetic Nervous System Norepinephrine Adrenal Gland Epinephrine 8 Thyroid Hormone T4 Normal Range Adrenal Gland Thyroid Gland (changes to T3 peripherally) Partial Starvation 4 Total Starvation 0 10 20 Days 30 40 Long CL et al. JPEN 1979;3:452-456 Landberg L, et al. N Engl J Med 1978;298:1295. Cancer Cachexia Anorexia Syndrome (CACS) Abdominal pain Malabsorption Taste alteration Depression Cachexia Constipation Radio/chemotherapy, surgery side effects Intestinal obstruction Derangement of Metabolism Increased Decreased • Lipolysis/lipid metabolism • Lipogenesis • Proteolysis • LPL activity • REE • Protein synthesis Lipolysis TNF-, IFN- LIF, TGF-β increase of leptin & altered orexegenic and anorexegenic signals Does cancer influence energy expenditure? Cancer itself does not have consistent effect on REE Increased ~ ¼ had 10% higher than predicted Unchanged Decreased ~¼ had 10% lower than predicted Carbohydrate Metabolism 1925 Cori & Cori demonstrate decreased glucose level High anaerobic glycolysis Glucose to lactate Increased lactate level Lactate Oxidized 15 % Regenerate to glucose 85% CHO Metabolism Gluconeogenesis: increased Lactate, glycerol, alanine Cannot be suppressed by glucose supplement Decreased glucose tolerance: insulin resistance Lipid Metabolism Depletion of fat store The proportion of wt loss: fat loss Associated with hypertriglyceridemia Mechanism Increased lipolysis Increased FFA and glycerol turnover Normal or increased lipid oxidation Decreased lipid clearance Decreased activity lipoprotein lipase (LPL) Protein Metabolism Increased protein metabolism Whole body protein turnover: unchanged Muscle tissue: largest pool Muscle protein loss, muscle wasting Decreased protein synthesis Cancer induced weight loss vs. other types of weight loss Cancer induced Caloric deficiency Lean body mass Body fat Caloric intake TEE REE Protein degradation Acute phase response Body weight Proteolysis inducing factors (PIF) Adapt from Kolter DP, Ann Int Med 2000;133:622 - Does nutritional status influence the clinical course and the prognosis? Reduce QOL Lower activity level Increase treatment related adverse reactions Reduce tumor response to treatment Reduce survival What are specific nutritional goals in cancer patients? Prevent and treating undernutrition Enhancing anti-tumor treatment effects Reducing adverse effects of antitumor Rx Improve QOL Energy requirement If REE cannot be measured, use rule of thumb Ambulant pt: 30-35 kcal/kg/d Bedridden pt: 20-25 kcal/kg/d Oncological Rx may modulate EE Do cancer patients require a distinct nutrient composition? Standard formula are recommended for EN of cancer pt Protein 1 g/kg/d (minimum) 1.2-2 g/kg/d Supplement with electrolyte, vitamins and trace element acording to RDA When should EN be started? If undernutrition already exists If it is anticipated that Pt will be unable to eat for > 7 d If an inadequate food intake (<60%) to eat for > 10 d Can EN maintain or improve nutritional status in cancer patients? Yes : In wt lost patients from insufficient intake: Gain more wt, lost less wt1 improve or maintain nutritional status2 maintain QOL 1. Systematic review of ONS, counceling Baldwin et al, 2004 2. Cancer cachexia and GI cancer Bozzetti F1989 and Lindh A 1986. 3. GI and H& neck cancer. Isenring EA, 2004 Can EN maintain or improve nutritional status in cancer patients? In the presence of inflammation Extremely difficult to achieve anabolism Without effective antitumor Rx impossible to reverse process At least to maintain wt or minimize wt loss Additional intervention pharmacological effort recommended to modulate inflammatory response Therapeutic challenges Other types of weight loss (caloric deprivation) Mechanical causes Treatment related causes Pcycholocical issues Provision of energy and protein can promote weight gain Ottery FD Cancer Practice 1994;2:123 Cancer induced weight loss Metabolic abnormalities No weight gain, even when added energy and protein provided Can metabolic modulators increase nutritional intake Steroids (short term) Improve appetite Nausea Pain Mechanisim: TNF-, IL-1 ADR: PUD, osteoporosis Can metabolic modulators increase nutritional intake Progesterone Improve appetite Wt gain QOL Megestorol acetate, Medroxy- progesteone acetate ADR: fluid retention, thromboembolism Can metabolic modulators increase nutritional intake ω 3 fatty acid ω 3 fatty acid: less active pro-inflammatory midiators Improve appetite and body weight Antagonized: Lipid mobilizing factors, proteolysis inducing factors Does supplementation with ω-3 fatty acid have beneficial effect in cancer patients? RCT : contradictory/controversial Evidence level C RCT : improve survival/Non significant effect on wt Did not improve wt or appetite Non RCT: improve survival, side effect of CTX Recent RCT: high dose EPA: wt stabilization, wt gain Unlikely to prolong survival in advance cancer The result of further trials are awaited Special situation Perioperative EN Radiotherapy Chemotherapy Transplantation Advance stage/ incurable Perioperative Severe nutritional risk benefit from SNS 10-14 d prior to major surgery even if surgery has to be delayed (A) All CA pt undergoing major abdominal surgery, preop EN preferably with immune modulating substreates 5-7 d independent of nutritional status (A) ESPEN guidelines on EN Clin Nutr 2006 Radiotherapy -ve effect of XRT on oral feeding early SNS may lead to complete course of Rx reduce morbidity in Rx of head & neck cancer PN failed to improve survival, infectious complication and noninfectious complication in abd XRT EN reduce wt loss, digestive intolerance to abd and pelvic XRT Critical Reviews in Oncology:Hematology 34 (2000) 137–168 Is there indication for EN during radiotherapy (XRT)or combined radiotherapy(cXRT)? Yes, use intensive counceling and ONS to increase intake (A) to prevent Rx associated wt loss To prevent interuption of XRT in GI, head and neck area If obstructive H&N or esophageal CA interferes with swallowing: tube feeding is preferred TF is preferred if local mucositis is expected (c) Routine EN is not indicated during XRT of other body regions (c) ESPEN guidelines on EN Clin Nutr 2006 Is there indication for EN during chemotherapy? No Routine EN during CTX has no effect on tumor response nor CTX associated unwanted effects (b) ESPEN guidelines on EN Clin Nutr 2006 Bone Marrow Transplantation Nutritional consequences of BMT N&V, mucositis, diarrhea Venooclusive disease (VOD) Graft vs. host dis (GVHD) Metabolic abnormalities Increased protein metabolism Hyperglycemia Hypertriglyceridemia Electrolyte abnormalities TPN: indicated Is there an indication for EN in advanced stages of incurable cancer patients? EN should be provided in order to minimize wt loss, as long as pt consents and the dying phase has not started (c) When EOL is very close, most pt require only minimal # of food and water to reduce thirst and hunger (b) ESPEN guidelines on EN Clin Nutr 2006 Risk of EN Does EN feed the tumor? No reliable data Theoretical considerations should No influence of the decision to feed a cancer patient Conclusion Complete improvement of nutritional state is not attained in short time Cancer Rx should not be postponed until nutritional rehabilitation achieved Nutritional Rx should be incorporated in to the overall Rx as early as possible Effort to improve nutritional and metabolic status may morbidity and mortality in pts who need surgery, XRx, XR-CTx