Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
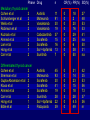
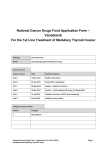
Recent progress of targeted kinase inhibitors in thyroid cancer A/Prof Rory Clifton-Bligh Kolling Institute of Medical Research, University of Sydney Department of Endocrinology Royal North Shore Hospital, St Leonards, NSW Royal North Shore Hospital 10th Asia and Oceania Thyroid Association Congress, Bali 23rd October 2012 Overview Scope of problem for thyroid cancer Molecular targets for thyroid cancer Data Success of kinase inhibitors in other cancers Pharmacogenomics Conclusions Thyroid cancer subtypes 15% DTC 85% cured with treatment 25% 35% 100% 7% “Unmet need” …10-year mortality Tuttle et al J Natl Compr Canc Netw 2010;8:1228-1274 15% recurrent/metastatic disease ~1/3 controlled by I-131, T4 and/or local Rx Metastatic Disease: existing therapies Brain Regional LNs -surgery -Surgery -XRT -RAI Lung -RAI Bone -RAI -XRT -Bisphosphonates Challenge in designing clinical trials in DTC: (sometimes) indolent natural history ! Waterfall plot of best percentage change in target lesion size from baseline, placebo group from Vandetanib trial in DTC, phase II Leboulleux et al Lancet Oncol 2012;13:897–905 Growth signalling: targets for new drugs RET RET/PTC RAS Somatic mutations in papillary thyroid cancer: BRAF PI3K Cell proliferation Differentiation BRAF RAS RET/PTC 30-70% 0-20% 20-50% PI3-kinase pathway also involved (PIK3CA copy number gain and mutation; PTEN): FTC PTC ATC Gild et al Nat Rev Endocrinol 2011; Hou et al Clin Cancer Res 2007;13:1161-70. 55% 24% 58% Growth signalling: targets for new drugs VEGF PDGF-β RET RET/PTC VEGFR-2 RAS PDGFR-β BRAF PI3K DTC tumor cell Adapted from Brose et al BMC Cancer 2011;11:349 Tumor endothelial cell Rationale for targeting growth factor signalling cascades in thyroid cancer - Preclinical studies conditional expression of BRAFV600E in adult mice causes PTC Treatment with MEK inhibitor resulted in partial tumor regression Charles et al Cancer Res 2011;71:3863-71 Rationale for targeting growth factor signalling cascades in thyroid cancer - Clinical data Medullary thyroid cancer in MEN2: RET genotype/activity determines biological aggressiveness Papillary thyroid cancer: BRAFV600E connotes risk of death Cote et al., 2003 N Engl J Med 2003;349: 1566-1569 BRAFV600E and immunohistochemistry mouse monoclonal antibody, clone VE1 (Capper and von Deimling) BRAFV600E positive by IHC positive by sequencing BRAFV600E positive by IHC negative by sequencing 58% 10% (32% negative for both IHC and sequencing) Bullock et al Endocr Rel Cancer 2012 Kinase inhibitors mimicking ATP within catalytic sites pseudosubstrate alteration of kinase stability Wan et al Cell 2004;116:855-867 sorafenib BRAF kinase Phase Medullary thyroid cancer Cohen et al 2 Schlumberger et al 2 Wells et al 2 Robinson et al 2 Kuzrock et al 1 Ahmed et al 2 Lam et al 2 Hong et al 1 Carr et al 2 Differentiated thyroid cancer Cohen et al 2 Sherman et al 2 Gupta-Abramson et al 2 Kloos et al 2 Ahmed et al 2 Carr et al 2 Hong et al 1 Bible et al 2 Drug n CR(%) PR(%) SD(%) Axitinib Motesanib Vandetanib Vandetanib Cabozantinib Sorafenib Sorafenib Sor’+tipifarnib Sunitinib 11 91 30 19 37 15 16 13 7 0 0 0 0 0 0 0 0 0 18 2 20 16 29 25 6 38 50 27 48 53 53 41 na 50 31 na Axitinib Motesanib Sorafenib Sorafenib Sorafenib Sunitinib Sor’+tipifarnib Pazopanib 45 93 30 41 19 28 22 39 0 0 0 0 0 3 0 0 31 14 23 15 18 28 4.5 49 42 35 53 56 73 37 36 nr Data from randomized, placebocontrolled studies Typical inclusion criteria Measurable disease at least one measurable lesion as measured by CT or MRI Disease progression (RECIST) (RAI-refractory disease: for DTC trials) Medullary Thyroid Cancer Vandetanib Cabozantinib Vandetanib RET, VEGF receptor, and EGFR tyrosine kinases MTC: approved for patients with unresectable locally advanced or metastatic disease (US, Canada, Europe) Vandetanib in MTC: phase III Vandetanib n = 231 Placebo n = 100 HR/OR p value 30.5 mo 19.3 mo 0.46 (0.31-0.69) 0.0001 Objective response rate 45% 13% 5.48 (2.99-10.79) <0.001 Disease control rate 87% 71% 2.64 (1.48-4.69) 0.001 Calcitonin response rate 69% 3% 72.9 (26.2-303.2) <0.001 CEA response rate 52% 2% 52.0 (16.0-320.3) <0.001 1°endpoint Progression free survival 2°endpoints Wells et al J Clin Oncol 2012;30:134-141 Vandetanib in MTC: phase III- PFS Wells et al J Clin Oncol 2012;30:134-141 Vandetanib in MTC: phase III- OS Overall survival data immature (HR 0.89; 0.48-1.65) A final survival analysis planned when 50% pts dead Wells et al J Clin Oncol 2012;30:134-141 Side-effects: vandetanib Diarrhoea (16%) Palmar-plantar erythrodysethesia (13%) Hypertension (8%) Prolonged QT Headache Nausea Leukopenia Discontinued therapy because of AE: Vandetanib 12% Placebo 3% Wells et al J Clin Oncol 2012;30:134-141 Cabozantinib (XL184) in MTC: phase III MET, VEGFR2, RET EXAM trial, international multicentre 330 pts, median age 55 y Cabozantinib n = 219 Placebo n = 111 PFS: Cabo 11.2 mo Placebo 4.0 mo (HR 0.28, 0.19-0.4, p < 0.0001) ORR: 28% Schoffski et al J Clin Oncol 2012;30: suppl abstr 5508 0% (p, ns) Side-effects: cabozantinib Diarrhoea (16%) Palmar-plantar erythrodysethesia (13%) Hypertension (8%) Differentiated thyroid cancer Vandetanib (Lenvatinib) (Sorafenib) Vandetanib in DTC: phase II 16 medical centres in Belgium, Denmark, France, Norway, Spain, Sweden, and Switzerland Vandetanib n = 72 Placebo n = 73 HR/OR p value 11.1 mo 5.9 mo 0.63 (0.54-0.74) 0.008 Objective response rate 8% 5% 1.57 (0.42-5.81) 0.501 Disease control rate 57% 42% 1.79 (0.93-3.46) 0.082 1°endpoint Progression free survival 2°endpoints Leboulleux et al Lancet Oncol 2012;13:897–905 Progression-free survival Vandetanib in DTC: phase II - PFS Leboulleux et al Lancet Oncol 2012;13:897–905 Vandetanib in DTC: phase II - OS (crossover from placebo to vandetanib allowed, confouding assessment of the effects of treatment on overall survival) Leboulleux et al Lancet Oncol 2012;13:897–905 Vandetanib in DTC: phase II - OS Two patients in the vandetanib group and one in the placebo group died from “treatmentrelated” serious adverse events (haemorrhage from skin metastases and pneumonia in the vandetanib group and pneumonia in the placebo group) Leboulleux et al Lancet Oncol 2012;13:897–905 Lenvatinib (E7080) VEGFR1-3, FGFR1-4, RET, KIT, PDGFRβ Phase II RAI-refractory DTC (papillary, follicular or Hurthle Cell) and disease progression demonstrated by RECIST during the prior 12 months 58 pts: PR 50% (CI, 37-63%) 35% required dose reduction for management of toxicity, and 23% were withdrawn Sherman et al, J Clin Oncol 29: 2011 (suppl; abstr 5503) Sorafenib Phase III trial ongoing (DECISION) Phase II: four trials including 168 patients with thyroid cancer treated with sorafenib Median progression-free survival (PFS) ranged from 58-84 weeks Partial responses in up to 25% Disease control rates (SD+PR) 59-100% Dose reductions due to AEs (mostly grade III) in 62% Brose et al BMC Cancer 2011;11:349 Thyroid dysfunction in patients on kinase inhibitors Elevated TSH/requirement for higher Thyroxine dose in Thyroid cancer patients: 49-78% of patients receiving vandetanib Hypothyroidism in patients with intact thyroid (eg renal cell cancer) In 36-85% pts treated with sunitinib In 18-68% pts treated with sorafenib Torino et al Hypothyroidism related to tyrosine kinase inhibitors: an emerging toxic effect of targeted therapy. Nat Rev Clin Oncol 2009;6:219–28. Other kinase inhibitors Dabrafenib selective for mutant BRAF Motesanib Axitinib Pazopanib Sunitinib I-131 Combinations Receptor tyrosine kinase + MEK inhibitor RAI + MEK inhibitor dabrafenib + MEKi Selumetinib (AZD6244)* TKI + mTOR inhibitor Temsirolimus + sorafenib* *Ho et al J Clin Oncol 2012;30:suppl abstr 5509 Sherman E et al J Clin Oncol 2012;30:suppl abstract 5514 BRAF MEK mTOR Kinase inhibitors in other malignancies Kinase inhibitors: haematologic malignancies CML: BCR-ABL Imatinib Nilotinib Dasatinib complete response for up to 8 years in 85% of patients Hairy cell leukaemia: BRAFV600E Vemurafenib Kinase inhibitors: melanoma BRAF inhibitor Chapman et al N Engl J Med 2011;364:2507-16 MEK inhibitor Flaherty et al N Engl J Med 2012;367:107-114 Kinase inhibitor combinations to overcome resistance: melanoma dabrafenib+trametinib dabrafenib Flaherty et al N Engl J Med 2012;doi: 10.1056 Pharmacogenomics BRAFV600E mutation: pharmacogenomics Clear evidence from hairy cell leukemia and melanoma that response to BRAF-targeted therapy is strongly associated with tumor genotype In vitro experience suggests that thyroid cell lines containing mutant BRAF cell lines are more sensitive to BRAF or MEK inhibitors ?no clinical evidence for pharmacogenomic effects in thyroid cancer: Motesanib (Phase 2, 93 pts) DCR BRAF+ BRAF- Leboeuf et al JCEM 2008;93:2194 60% (6/10) ns 33% (5/15) Sherman et al N Engl J Med 2008;359:31 RET mutation: pharmacogenomics In subgroup analysis, suggestion of higher response rate to vandetanib in sporadic tumors with M918T mutation in vitro, Vandetanib does not inhibit the V804 mutations in RET Wells et al J Clin Oncol 2012;30:134-141 Conclusions Thyroid cancer mortality is related to: These signalling pathways are targets for several drugs in clinical use or development Well-defined activation of growth factor signalling pathways Loss of iodine uptake (DTC) Many pts require dose reduction or drug withdrawal to manage toxicity Some treatment-related deaths reported Vandetanib has FDA approval for use in MTC Balance of risks vs benefits needs to be carefully addressed in phase III trials Need greater definition of those pts who will have survival benefit from treatment Thyroid Group at RNSH, Sydney Bruce Robinson Diana Learoyd Rory Leigh Delbridge Stan Sihdu Clifton-Bligh Endocrinologists Scientists Mark Sywak Endocrine Surgeons Pathologist PhD students Jimmy Lee Dindy Benn Anne-Louise Richardson Martyn Bullock Anthony Gill Justin Julian Gundara Ip and Matti Gild