Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
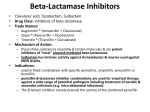
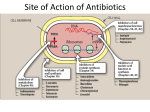
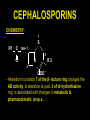
PENICILLINS CEPHALOSPORINS & OTHER β-LACTUM ANTIBIOTICS Dr. Rajendra Nath Professor PENICILLINS CEPHALOSPORINS & OTHER β-LACTUM ANTIBIOTICS • Useful & frequently prescribed AM agents . • Share a common structure & mech. of action i.e. – inhibition of synth. of the bact. peptidoglycan cell wall . PENICILLINS CEPHALOSPORINS & OTHER β-LACTUM ANTIBIOTICS • β- lactums - include Cephalosporin antibiotics which are classified by generations . PENICILLINS CEPHALOSPORINS & OTHER β-LACTUM ANTIBIOTICS • β- lactamase inhibitors e.g.Clavulanate , Sulbactum etc. are used to extend the spectrum of Penicil. against β- lactamase prod. organisms. PENICILLINS CEPHALOSPORINS & OTHER β-LACTUM ANTIBIOTICS • Other β- lactums include – - Carbapenems including Meropenem & Imipenem which have broadest AM spect. of any antibiotics . • Monobactums – e.g.- Aztreonam has G-ve spect. resembling that of Amino -glycosides . PENICILLINS CEPHALOSPORINS & OTHER β-LACTUM ANTIBIOTICS Bact. resist. against the β- lactum antb.s continues to ↑at high rate. Mech. - by β –lactamase that destroy the antb - alteration in or acquisition of novel penicil. binding proteins ( PBPs) . - Decreased entry & / or efflux of antb.s . PENICILLINS -One of the most important gp of antibiotics. - However numerous other AM agents have been prod. since the first penicil. become available. - These are still used widely & many of these are currently the DOC for a large no. of infectious diseases . PENICILLINS - In 1928 in laboratory of St mary’s hosp. London , A. Fleming observed that a mold contaminating one of the bact. cultures caused the bact. in its vicinity to undergo lysis. Because the the mold belonged to the genus Penicillium , Fleming named the antb. PENICILLINS substance as Penicillin . Chemistry : Basic struct. consists of 1. Thiazolidine ring (A) connected to 2. β- lactum ring (B) to which attach 3. Side chain (R) . PENICILLINS O R C 2 S NH CH CH B O= C Amidase CH3 C A N 1 CH3 CH COOH Penicillin Penicillinase site of action PENICILLINS A. Thiazolidine ring B. β- lactam ring 1. Site of action of penicillinase 2. Site of action of amidase PENICILLINS - The penicillin nucleus itself is the chief struct. requirement for biologic. activity . Metabolic transformation/ chem. alteration of this portion of the mol. causes loss of all sig. AB activity - Side chain determine many of the AB & pharmacol. character of a particular PENICILLINS type of Penicillin. - Penicil. G ( benzyl penicil. ) has the greatest AM activity of these & is the only natural penicil. used clinically. Semi-synthetic Penicillins : It has been discovered that 6- aminopenicillanic acid could be obtained from PENICILLINS cultures of P. chrysojenum lead to the dev. of the semi-synth. Penicil.s .by adding different side chains in this . -6-aminopenicillanic acid is now prod. in large quantities with the aid of the amidase from P. chrysojenum . PENICILLINS Unitage of Penicillin : - one Int. unit ≡ 0.6 μg of the cryst. sod. salt of Penicil. G. -1mg of pure Penicil. G ≡ 1667 units. Mech. of Penicillins : -The cell walls of bact. are essential for their normal growth & development. PENICILLINS - Peptidoglycan is a heteropolymeric component of the cell wall that provides rigid mech. stability . - Cell wall is 50-100 mols thick in G+ve & ½ molecule thick in G-ve bacteria . - Peptidog. is composed of glycan chains having linear strands of two PENICILLINS alternating amino sugar (N-acetyl – glucosamine & N- acetyl muramic acid) & they are cross-linked by peptide chain . Biosynth. of Peptidoglycan : involves three stages PENICILLINS Final stage involves completion of the cross link .This accomplished by a transpeptidation react. that occurs outside the cell memb.( with the help of Transpeptidase enz. which is memb. bound ). These enz.s & related proteins are now called as Penicillin Binding Proteins ( PBPs). PENICILLINS It is this last step in peptidoglycan synth. that is inhibited by the β- lactum antb.s & glycopeptide antb.s (e.g.Vancomyc.) PENICILLINS - Main target for the action of penicil.s & cephalosporins are these Penicil. Binding Proteins (PBPs) .All bact. have such entities e.g.- E .coli PENICILLINS PENICILLINS has 7 & S. aureus has 4 PBPs . The PBPs vary in their affinity for diff. β – lactum antb.s , although interact. become covalent . - ↓ of transpept.( PBP-I) causes formation of spheroplast & rapid lysis. - ↓ of PBP-II & III ( Carboxypeptidase & endopeptidase enz.s) cause delayed lysis or production PENICILLINS of spherical cells & large filamentous form of bacterium. Penicil.↓ synth. of cell wall & thereby expose the org.s to the lethal external environment which is not matching with internal osmotic –pressure & bact . swells & lysis occurs . PENICILLINS Death of the bact. also occurs due to activation of autolysing enz.s called autolysins or murein -hydrolase . -Lethality of penicil. involve both lysis or nonlytic mech. PENICILLINS Mech. of bact . Resist. to penicillin ( & Cephalosporins ) : 1.Micro-org may be intrinsically resist. because of structural diff. in the PBPs that are the targets of these drugs (A sensitive strain may acquire resist. of this type by the dev. of high mol. PENICILLINS wt. PBPs that have ↓ affinity for the antb. e.g.- Penicil. resistance in Streptococcus gp. emerged as a result of replacement of its PBPs with resist. PBPs from S. pneumoniae. PENICILLINS 2. Other way of bact. resist. is caused by the inability of the agent to penetrate to its site of action e.g.G-ve bact. PENICILLINS - in G+ve bact . the peptidoglycan polymer is very near the cell surface , some G+ve bact. have polysacch. capsule that are external to the cell wall but they are not the barrier to the diffusion of β- lactums . PENICILLINS - In G-ve bact. the inner memb. is analog. to the cytoplasmic memb. of G+ve bact. & is covered by outer memb. of Lipopolysaccharide & capsule ,it functions as a impermeab. barrier for some antb.s PENICILLINS Some small hydrophilic antb.s diffuse through aqueous channels in the out. memb. that are formed by protein called porins . -Broad spect. Penicil.s e.g. – Ampicill. & Amoxycill. & most of the Cephalosporins diff. through the pores in the PENICILLINS E.coli outer memb. more rapidly than can Penicill. G ( the no. & size of the pores vary e.g.- Pseudomonas aeru. lack the classical high permeability porins .) 3. Active efflux pumps serve as another mech. of resist. removing the antb.s PENICILLINS PENICILLINS from its site of action before it can act e.g.-β- lactum resist. in P.aerug. ,E.coli & N. gonorrheae . 4.Bact. can also destroy β- lactum antb. enzymatically by β- lactamases which inactivates certain of these antb.s . PENICILLINS -diff. micro-orgs elaborate a no. of distinct β- lactamase which often are described as Penicillinases or Cepha linases . These are grouped into 4 clases ( A-D) . - Class A β- lactamases include the extend. spect. β –lactamases which PENICILLINS degrade Penicil.s , some Cephalospor. and in some instances ,Carbapenems. -Class B: β-lactamases are Zn++ dep. enz. that destroy all β- lactams except Aztreonam . - Class C: β- lactamases are active against Cephalosporins. PENICILLINS -Class D : include Cloxacillin deg. enz.s - G+ve bact. prod. & secrt. a large amount of β- lactmases . Most of these are Penicillinases . The information for Staphylococcal penicillinase is encoded In a plasmid & this may be transferred by bacteriophage to other bact. PENICILLINS - - In G-ve bact. β-lactamases are found in relatively small amounts . they are encoded either in chromos. or in plasmids & may be constitutive or inducible . The plasmids can be transferred between bact. by conjugation . PENICILLINS - - Other factors : micro-org.s adhering to implanted prosthetic devices ( e.g.- catheters , artific. Joints , prosth. heart valves etc.) prod. biofilms & are much less sens. to antb.s . The presence of proteins & other PENICILLINS constituents of pus, low pH or low oxyg. tension does not appreciably ↓ the ability of β-lactum antb.s to kill bact. However bact. that survive inside visible cells of the host gener. are protected from the action of the β- lactum antb.s . PENICILLINS Classification : According to their spectrum of AM act. I Narrow spectrum A. Penicillinase sensitive i) Penicillin G ( parenteral ) – highly active against sensitive strains of G+ve cocci hydrolyzed by PENICILLINS penicillinase , not effective against most strains of S. aureus e.g.-Crystalline or Benzyl Penicil. or Penicil. G. - Procaine Penicil. - Benzathine Penicil. ii) Phenoxy methyl Penicil. or Penicil. V PENICILLINS ( orally active ) B. Penicillinase resist. Penicil. -e.g.Methicillin , Naficillin , Cloxacillin Oxacillin , Flucloxacillin etc. have less potent AM activity against micro-org. sensitive to Penicil. G . but agent of first choice for PENICILLINS penicillinase prod. S. aureus & S. epid -ermidis . C. Penicillinase inhibitors . e.g.- Clavulanic acid ( comb. with Amoxycil.) - Sulbactum ( + Ampicillin ) - Tazobactum ( + Piperacillin) PENICILLINS They are given with broad spectrum antb.s to prevent hydrolysis by broad spect. β- lactamases ( in G-ve bact. e.g. E.coli .) II Broad spect. Penicillins : A. Carboxypenicil. e.g.- Carbenicillin Carbenicil. Indanyl ,Ticarcillin . PENICILLINS their AM activity is extended to include Pseudomonas , Enterobacter & Proteus gp. (inferior to Ampicil.against G+ve cocci & L.monocytogenes & less active than Piperacil. against Pseudomonas.& also known as antiPseudomonal penicillins ) PENICILLINS B. Aminopenicillins : e.g.- Ampicillin , Amoxycillin, etc.. They are also effective against G- ve org.s e.g. – H. influenzae , E. coli , Proteus mira bilis . etc. . But they are sensitive to penicillinase enzyme. (They are used now with β- lactamase inhib.s e.g. Clavulanic acid which further extends their spectrum ) PENICILLINS C. Uriedopenicillins ( extended spect. penicil.) : e.g.- Azlocillin , Mezlocillin & Piperacillin . Excellent activity against Pseudomonas ,Klebsiella & other G-ve org.s PENICILLINS Pharmacological propert. in general: - Following abs. of orally administered penicil. these agents are distributed widely through out the body. - Therapeutic conc. attain readily in tissues & in secret. e.g. joint fluid , pleural fluid ,pericardial fluid & bile PENICILLINS -Low conc. in prostatic fluid ,brain tissue ,intra-ocular fluid & in CSF (conc of penicil. is < 1% of those in plasma , but in inflammed meninges conc. may ↑ upto 5% of plasma ) . - Eliminated rapidly by glomerular filtr. & renal tubular secrt. (t½ -30-90 min.) PENICILLINS Penicil.G & Penicil. V : The AM spect. of penicil. G &V are very similar for aerobic G+ve microorg. (but penicil. G is 5-10 times more active against Neisseria sp. & against certain anaerobes). They are narrow spect. & enz. sens. Penicil.s PENICILLINS Spectrum : effective against Pneumococci. streptococci, Meningococci , non βlactamase prod. gonococci & staphy. (> 90% strains of staphyl. Isolated from individuals inside or outside hospitals are now resist.) PENICILLINS - Treponima pallidum , bacil. anthracis & vast majority of strain of C. diphther. are senst. but some are resist. - Actinomyces , Clostridium sp. (anaer. micro-org.) are highly senst. PENICILLINS ( Bact. fragilis is exception ) . - None of the Penicil.s are effective against Amoeba , Plasmodium , Rikettsia , fungi or viruses . Absorption : Oral about ⅓rd of oral dose is absorbed in favorable cond. not destroyed by PENICILLINS gastric juice ( 2/3rd destroyed by GJ) . Penicil. V is more stable in acid hence better absorbed . -Food may interfere with abs. of all Penicil.s -Parenteral – after I.M. inj. peak conc. of Penicil.G reached with in 15-30 mins . PENICILLINS ( vol. declines as half life of Penicil. G is 30 mins ) . Different measures are there to prolong its existence in body e.g. 1. Repository prep. -Procain Penicil. & Benzathine Penicil. they release PENICILLINS penicil. G. slowly from the area in which they are injected & prod. relativ. low but persistent conc. of antb. in blood . Penicil.G. Procaine susp. is an aquous prep. of the crystalline salt ( H/S test is done by I.D. test of 0.1 ml of proc.) PENICILLINS - It is a painless inj. Benzath. Penicil. susp. of the salt obtained by the comb. of 1 mol. of an ammonium base & 2 mol. of penicil. G. . The long persistence of penicil. conc. in blood after I.M. inj. reduces cost , need for repeated inj. PENICILLINS and local trauma. benz. penicil. has got longest duration of detectable antb. A dose of 1.2 mill. unit I.M. → conc. of 0.09 μg/ml on the 1st , 0.02 μg/ml on 14th & 0.002 μg/ml on 32nd day (avg. duration is 26 days) 2. Use of Probenecid that blocks renal PENICILLINS tubular secr. of penicil. & thus exct. ,is also used to increase the dur. of action - It also ↑ the conc. of penicil. in CSF as it does not readily enter the CSF normally (increase abs. in meningitis) - Penicil. is secrt. rapidly from the CSF into blood stream by an active PENICILLINS transport process & probenecid compe -titively ↓ this transport & thus↑ the conc. of penicil. in CSF. Excretion : Penicil. G. is eliminated rapidly from the body mainly by the kidney ,but small part in the bile & other routes . PENICILLINS Therapeutic Uses : 1.Pneumococcal inf.-Penicil. G (DOC) -Pneumococcal Pneumonia – (Penicil. G- 24 million U daily Penicil. V – 500 mg orally 6 hrly). -Pneumococ. mening. – until it is established that penicil.G .is sens. PENICILLINS it is treated with Vancomycin + III gen Cephalosporin ( if sensitive - penicil. G is given -20-24 mill. U/day x 14 days) 2. Streptococ. Inf. – in scarlet fever ( Streptococ. pharyngitis ) – penicil. V. -500 mg 6 hrly x 10 days penicil. G. – 6 lacks U OD x 10 days PENICILLINS or single inj. of Benz. Penicil. 1.2 mill U stat.) also effective in –Streptococcal pneumonia , arthritis , meningitis & endocarditis . 3. Inf. with Anaerobes : mixt . of org.s most are sens. to penicil. G. exception is B. fragilis gp. , PENICILLINS -Penicil.G. + Metronidazole or Chlora - mphenicol . 4. Staphylococ inf. – penicil. resist penicil. e.g.Naficillin or Oxacillin 5. Meningococ. Inf. – Penicil G. ( DOC) given I.V. high dose PENICILLINS 6. Gonococ. Inf. – resist. to penicil. G & they are no longer the therapy of choice ( IIIgen. Cephalosporins Ceftriaxone is given ) . 7. Syphilis – penicil.G. is highly effective in primary, second. & latent syphilis of < 1 y dur. PENICILLINS (Proc. Penicil. -2.4 mill. U /day I.M. + Probenecid 1 gm/ day orally x 10 days or Benz. Penicil. G. 2.4 mill. U I.M. 1 -3 weekly ). Pts with late latent syph., neurosyph , cardiovas. syph. – 20 mill. U of penicil G. daily x10 days (child.-50,000 U/kg of Penicil. G . in two div. doses.) PENICILLINS most pts dev. Jerisch Herxheimer reac. (several hrs after the 1st inj of penicil. G) Chills with fever, headach, myalgia & arthralgia may dev. & syph. lesion may become more prominent . It fades with in 48 hrs & does not recur with 2nd PENICILLINS inj. ( due to Spirochaetal antigens ). 8. Actinomycosis – Penicil. G. – DOC ( 12 -20 mill. U I.V. /day x 6 wks) 9. Diphtheriaspecific antitoxin (antidiphtheritic serum) is the only effective tt. however penicil. G eliminate the carrier state - PENICILLINS ( Proc. Penicil. 2-3 mill. U / day x 10-12 days.) 10. Anthrax -now resist. in most of the cases 11. Clostridial inf. – penicil. G. is DOC in (i) Gas gangrene (by C.perfringens,12-20 mill. U/day), debridement of inf. area is necessary apart from the drug . (ii) No effect on ultimate outcome of PENICILLINS Tetanus ( C. tetani ) ,hence tetanus immunoglob. (ATS ) is indicated along with debridement of dead tissue + Penicil G (10-20 mill. U /day I.M.) to eradicate the bact. - Fusospiroch. Inf. - Gingivo-stomatitis e.g.-Trench mouth (Penicil. V.-500 mg 6 hrly x7 d) 12. Rat bite fever : by Spirillium minor senst. to penicil.( G -12-15 mill. U/d x 3-4 wks) PENICILLINS 13. Listeria inf. – Ampicillin 1-2 gm 4 hrly. ( +Gentamycin in immuno -comp. host & pt with meningitis.) & penicil.G(15-20 mill. U/d) are DOC. 14. Erysepilas –Pasteurella multocida wound inf. after dog / cat bite . senst. to penicil. & Ampicil.s PENICILLINS Prophylactic use – was effective in previous inf.s but still used in 1. Streptococcal inf. & cases of deep burn. Single inj. of Benz. Penicil.-1.2 mill.U 2.Recurence of Rheumatic fever – oral –penicil. V or PENICILLINS Benz. Penicil. G – (1.2 mill. U once a month.) 3. Syphilis – prophyl. for contacts . 4. Surg. procedure in pts with valvular heart dis.( Dental extractions ). PENICILLINS 2. Penicillinase resist penicil.: This type of penicil. is resist. to hydrolysis by Staphy. penicillinase (their use should be restricted to the tt of inf. which are caused by staphy. that secrete this enz.) -these are less sens. than is penicil. G PENICILLINS against other penicil. senst. micro-org -Methicil. resist. micro-org.s are resist. to all the penicil. resist.Penicil.s & Cephalosp.s . -Hospital acquired inf. are also resist to these penicil. PENICILLINS e.g.Isoxazolyl Penicil.: Oxacillin , Cloxacillin & Dicloxacillin – -These are congeneric semi –synth. Penicil.s . - These are similar pharmacologically, abs. adequately after oral administ. PENICILLINS ( abs. is more effective on empty stomach) . Naficillin : This semisynth. Penicil. is highly resist. to penicillinase & effective against inf. caused by penicillinase prod. strains PENICILLINS of S. aureus . - abs. in GIT is irregular ( inactivated in acid medium ) therefore given parenteraly ( 1 gm I.M. ) . - conc. of drug is adequate in CSF for the tt of S. meningitis . PENICILLINS Aminopenicillins : Ampicillin , Cloxacillin & their cong.s - these are known as broad spect. antb have similar AM activity . -they all are destroyed by β- lactamase - they are bactericidal for both G+ve & G-ve bact. PENICILLINS - N. gonorrhoeae , E. coli , P. mirabilis, Salmonella & Shigella were highly senst. to these when they are first used but now resist. is increasing. (Pseudomonas & Klebsiella are resist.) PENICILLINS ( however concurrent administ. of a βlactamase inhib. e.g.- Clavulanate or Sulbactum markedly expands the Spect. of activity of these drugs ) dose – 500mg QID or 0.5 – 1 gm sod. Ampicil. Inj. I.M. ( adjustment is req . in cases of renal dysf.) PENICILLINS Amoxycillin : - abs. is more complete & rapid than Ampicil. & stable in acid & given orally. - spect. similar ( except less senst. in Shigellosis ) - food does not interfere with abs. PENICILLINS - Incidence of diarrhea is less - Effective conc. of orally administ. Amoxy. are detectable in plasma twice as long as with Ampicil. - Probenecid delays exct. of drug . Uses -1. URTI against S. pyog. & S. pneumonia & H. influenzae . PENICILLINS -effective for sinusitis , otitis media & acute exacer. of chr. Bronchitis & epiglottitis - Addition of β –lactamase inhib. ( Amoxy + Clavulanate & Ampicil + Sulbactum ) extends the spect. to H. influenzae & enterobacteriaceae. PENICILLINS 2. UTI 3. Meningitis – not alone but in comb. with Vancomycin + 3rd gen. cephalo. 4. Salmonella inf. – bacteremia & enteric fever ( Typhoid) synd. respond well to these . Fluoroq. , / Ceftriaxone are DOC but Trimeth. PENICILLINS + Sulfamethoxazole or high doses of Ampicil. also are effective ( 12 gm/d for adults) . Antipseudomonal Penicil.s : Carboxypenicillins – e.g.Carbenicillin ,Carbenicillin indanyl ( indanyl ester of carbenicilin which PENICILLINS is acid stable & used orally) & Ticarcillin . - They are active against some strains of Pseudomonas aeruginosa & certain sp. of Proteus ( that are resist. to Ampicil.& congener ). - Hypokalemia may occur. PENICILLINS Ureidopenicillins : e.g.- Mezlocillin & Piperacillin have superior activity against P.aerug. - they are also used against Klebsiella - they are senst. to destruction by β – lactamases . PENICILLINS (In comb. with a β – lactamase inhib. Piperacil. &Tazobactum has the broadest AM spect. of the penicil.s ) Uses – serious inf. caused by G-ve bacteria. PENICILLINS ( esp. in pts of impaired immuno logical defenses & inf.s acquired in hospitals) so greater use in bacteremias ,Pneum. inf. following burns & UTI . ( in neutropenic pts ) PENICILLINS Side effects : 1. Hypersenst. React. – they are the most common ADRs noted in penicil.s & most comm. cause of drug allergy – include maculopap. rash ,urticarial rash fever , bronchospasm ,vasculitis PENICILLINS serum sickness ,exfol. dermatitis, St. Johnson’s synd. & anaphylaxis. - It may occur with any dosage form of penicil. - Cross allergy occur between diff. gps. of penicil.s (occurrence of untoward effects does not necessarily imply repetitions on PENICILLINS .) - H/S react. may appear in the absence of a previous known exposure to drugs (may be due to prev. unrecognized exposure to subsequent exposure penicil. in the environment e.g.- foods of animal origin or from the fungus prod. penicil.) PENICILLINS - Although H/S clears after stopping antb. but may persist for 1-2 wks or longer after therapy has been stopped . - In few instances , it is necessary to stop the future use of penicil. PENICILLINS because of risk of death ( pts should be warned for this). Mech.penicil. & their breakdown prod.s act as haptens after covalent react. with proteins . major breakdown moiety is penicilloyl moiety which is the major PENICILLINS determinant moiety ( MDM) . - IgE med. react. occur due to MDM ( in 25% other breakdown prod.s are responsible) - The most serious H/S react.s are angioedema ( marked swelling of lips , tongue ,face, peri-orbital tissue PENICILLINS frequently accomp. by asthamatic breathing.) - H/S react. can occur with small testing dose ( intradermal inj. ) 2. Serum sickness : mild fever , rash , leukopenia , arthralgia ,purpura, lymphadenopathy PENICILLINS spleenomegaly, mental changes ,ECG abnormalities , albuminuria ,hematuria. It is mediated by IgG antibodies. ( it occurs when penicil. is continued for a wk or more but is rare ). - fever may be the only symptom - eosinophilia & rarely int. nephritis PENICILLINS Management : - pts history is most practical. - Intradermal test -Desensitization is recomm.. Low dose penicil. in ICU ( 1, 5, 10, 100 & 1000 Unit / day ) - Adrenaline ( S.C. inj.) PENICILLINS Antihistaminic ( injectable) - Glucocorticoids ( inj.) 3. Other reactions – -Bone marrow depression leads to granulocytopenia -Hepatitis (Oxacil. & Naficillin.) - inj. can cause local pain & inflammation - (Intrathecal inj. can cause arachinoiditis & severe encephalopathy .) CEPHALOSPORINS History & Source – First source – Cephalosporium – acremonium isolated in 1948 by Brotzu . Crude filtrates from cultures of this fungus were found to inhibit the growth of S. aureus to cure staphylococ. inf. & Typhoid fever CEPHALOSPORINS caused by Salmonella sp. - Cultures shows three distinct antb.s which were named Cephalosp. P, N, C. - With isolation of the active nucleus of Cephalosp. C. i.e. 7 amino cephalosporanic acid & with addition CEPHALOSPORINS of the side chains it become possible to prod. synthetic comp.s having equiv. AM activity or greater activity than parent comp. Chemistry : Cephalosp. C contains a side chain derived from D-α aminoadipic acid CEPHALOSPORINS condensed with a dihydrothiazide βlactam ring syst. ( 7- aminocephalospo -ranic acid ). -- comp.s containing 7- aminocephalo. acid are relatively stable in dilute acid & are highly resist. to penicillinases . CEPHALOSPORINS CHEMISTRY: 1 S R1 C NH–7 3 O N R2 COO ˉ - Alteration in position 7 of the β- lactum ring changes the AB activity & alteration at post. 3 of di-hydrothiazine ring is associated with changes in metabolic & pharmacokinetic prop.s . CEPHALOSPORINS Mech. – ↓ cell wall synthesis ≡ Penicillins Classification : Well accepted syst. of classif. by generation is very useful based on gen. features of AM activity . ( Cephal. Having A after Cef or Ceph are Ist Gen. CEPHALOSPORINS First Generation : Name Cephazolin Dose Spectrum 1-1.5 gm 6 hrly well effective against ( t½ -2 hr ) G+ve but less active Cephalexin (O) 1 gm 6 hrly against G-ve bacterias ( t½ - 0.9 hr) Streptococ.( except Cephadroxyl (O) 1gm 12hrly Penicillin resist str.) ( t½ -1.1 hr ) Staphylococ. aureus Cephalothin ( N) (except. Methicillin. Cephaloridine (N) resist strains ) + PEK (Cephal. having A after Cef or Ceph are Ist Gen. ) CEPHALOSPORINS FIRST GENERATION Cephalexin , po Cefazolin Cephalothin Cephradine , po Active against G+ cocci ( except. enterococci & MRSA ): s. pneumoniae, s. pyogenes, s. aureus, & s. epidermidis Indicated for streptococcal pharyngitis ( e.g. cephalexin) Commonly used (eg. Cefazolin) as prophylactic for surgical procedures. Modest activity against G- bacteria ( Minimal activity against G-cocci & G +ve bacilli ) These do not cross BBB ( not suitable for treating brain abcess / meningitis ) & all are sensitive to β- lactamase enz. Degradation . CEPHALOSPORINS Second Generation : Cefoxitin (BF*) inj. -2gm 4 hrly (t½ - 0.9 hr ) Cefaclor (O) 1gm 8 hrly (t½ - 0.7 hr ) Cefamandole ( bl , A ) Cefuroxime 3gm 8hrly ( * ,BB) (t½ - 1.7hr) Cefotetan inj. 2-3gm 12hrly ( BF, bl ,A ) They are in between 1st & 3rd gen. little less effect. against G+ve & little more against G- ve ( HNPEK ) but not as active against G+ve org. as 1st gen. cephalosp. Loracarbef (O) ( Cephal. Containing PI are 4th gen. ) CEPHALOSPORINS SECOND GENERATION Cefoxitin ( mefoxin ) Cefuroxime ( zinacef ) Cef. axetil ( zinnat ) Cefaclor ( ceclor ) Cefprozil ( cefzil ) Mainly effective against G- bacteria ( cocci & bacilli ) Modest activity against G+ bacteria & anaerobes Cefoxitin active against bowel anaerobes (B. fragilis ) Cefuroxim active against H. influenzae, M. catarrhalis, S. pneumoniae crosses BBB . Cef. Axetil- oral form of cefuroxim Cefaclor active against H. influenzae, M. catarrhalis &E.coli Cefprozil- similar to cefaclor, c. axetil and augmentin - Liked by children Second Generations are used primarily for URTIs ( acute otitis media, sinusitis ) and Lower RTIs ( acute exacerbation of chronic bronchitis) (These drugs are more stable to β-lactamase degradation ) LORACARBEF: ≡ Cefaclor, can be given orally , overdose can cause seizures CEPHALOSPORINS Third Generation : Cefotaxime inj. 2gm 4-8hrly They are much more (t-½ -1.1 hr ) act. against G-ve org. Cefpodoxime 200-400mg 12hrly include. β -lactamase proxetil ( O) ( t½ - 2.2 hr ) prod. less act against Ceftriaxone inj. 2gm 12-24hrly G+ve org.( Enterobac (b½,ch,T,G) (t½ -8 hr ) P.aerug.exct penicilli-. Cefoperazone inj.1.5-4 gm 8hrly nase prod. ,Serratia , ( P,b,D,A,T,bl) ( t½ - 2.1 hr ) N. gonor. are more Cefexime (O) 200-400mg 12hrly sensitive to 3rd gen.) CEPHALOSPORINS Ceftazidime ( P) Cefibuten ( O ) Cefdinir ( O) inj. 2 gm 8 hrly ( t½ -1.8 hr ) 400mg 4 hrly ( t½ - 2.4 hr ) 300mg 12 hrly ( t½ - 1.7 hr ) ( Cephal. ending with ME are 3rd gen. exceptCefuroxiME ) CEPHALOSPORINS THIRD GENERATION Ceftriaxone ( rocephin ) Cefotaxime ( claforan ) Cetazidime ( fortum ) Cefoperazone ( cefobid ) Cefixime ( suprax ) These are highly active against G-ve cocci, bacilli & anaerobes They have enhanced G- activity, H. influenzae, N. meningitidis, N.gonorrhea, P. aeruginosae, M. catarrhalis, E.coli, most Klebsiella are sensitive Ceftriaxone has long half-life . Not advised in neonates (interferes with bilirubin metabolism ) Cefotaxime preferred in neonate ( does not interfere with bilirubin metabolism ), as may ceftriaxone. Ceftazidime & cefoperazone have excellent activity against p. aeruginosae. Cefixime has similar activity to amoxicillin & cefaclor for actute otitis media -These drugs are highly resist. to degradation by β- lactamases by G-ve org.s -These can penetrate BBB ( Except-Cefoperazone & Cefixime ) CEPHALOSPORINS Fourth Generation : comp. to 3rd gen. but more resist. to some β – lactmases ( induc. type I ) & not active Cefpirome against anaerobes ( Cephal. containing PI are 4th gen. ) o = orally , * = resist . to β- lactamases , BF = act. ag. B. fragilis , P = act. Ag. P. aeruginosa , T = Typhoid , G = gonorh. , A = alcohol intolerance , N = nephrotoxic Cefepime inj. 2 gm 8 hrly ( t½ -2 hr ) CEPHALOSPORINS D = Diarrhea , BB = crosses BBB , b = exc. in bile , b½ = half exct. in bile , bl = bleeding , ch = synd. mimicking cholecystitis . Now 5THGeneration has also came , although they inhibit the cell wall synthesis but in a different way , they bind to & inhibit PBP-2 produced by MRSA & Penicillin resist . S. pneumoniae which is not inhibited by majority of antb.s . -Also active against Enterococcus .& retain the activity of IV gent. against G-ve bacilli ( esp. E.coli & Pseudomonas) e.g.-Ceftaroline app. by FDA & Ceftobiprole ( phase III trial) -Used for comm. aquired bact. Pneumonia & acute Bact. Skin inf. incl. MRSA ) CEPHALOSPORINS Mechanism of Bacterial Resistance : Resist. to Cephalosp. may be related to the : -inability of the antb. to reach site of act. or - alteration in the PBPs that are targets of the cephalosp. such CEPHALOSPORINS that the antb. bind to bact. enz.s ( β – lactamases esp. inducible type I ) that can hydrolyze the β- lactum ring & inactivates the Cephalosp.s CEPHALOSPORINS General features : Cephalosp.s are excrt. primarily by the kidney , therefore dosage should be altered in case of renal insufficiency. - Probenecid slows the tubular secrt. of most cephalosporins . (Cefoperamide & Cefoperazone are mainly excrt. in bile .) CEPHALOSPORINS - Cefotaxime is deacetylated in vivo & half excrt. through kidney & half in bile . - Several of the Cephalosp.s penetrate CSF in sufficient conc. to be useful in meningitis (Cefuroxime ,2nd & 3rd CEPHALOSPORINS gen. cephalosp.s ) . - Cephalosp.s cross the placenta & also found in high conc. in synovial & pericardial fluid . - Penetr. in aq. humor of the eye is good after syst. administ. of 3rd gen. Cephalosp.s ( in vit. humor it is poor) CEPHALOSPORINS Side effects : 1. hypersenst. react. is most common immed. react. e.g. anaphylaxis , bronchospasm & urticarial rash . - most commonly maculopapular rash dev. usually after several days of CEPHALOSPORINS - therapy . Cross reactivity occurs in between Cephalosp.s & penicil.s due to the structural similarity to the Penicillins (about 20 % cases who are allergic to penicil.s are also allergic to Cephalosp.s) . CEPHALOSPORINS - Pts with mild react. to penicil. appear to be at low risk of rashes or other allergic react. following administr. of Cephalosp.s . but pts having recent severe allerg. react. or anaphylaxis to penicil. should be given Cephalosp. with great caution CEPHALOSPORINS - Rarely causes bone marrow dep. → granulocytopenia . - Nephrotoxicity occurs esp. with Cephaloridine & Cephalothin . - Diarrhea with Cephoperazone due to biliary exc. - Alcohol intolerance ( disulfiram like CEPHALOSPORINS react. in Cefamandole , Cefotetan & Cefoperazone ). - Bleeding related to hypoprothrombin – emia ( Cefotetan & Cefoperazone ) - Superinfection by 3rd ,4th & 5th gent. Therapeutic Uses : Used widely- effective prophylactically & therapeut. CEPHALOSPORINS 1st Gen. Cephalosp.s – - excellent for skin & soft tissue inf.s - colorectal surgery. - Prophylaxis for intracel. anaerobes . 2nd Gen. Cephalosp.s - they are displaced by 3rd gen. Cephalosp. CEPHALOSPORINS - active for URTI , for Penicil. resist. S. pneumoniae inf. - Otitis media - Diabetic foot inf. 3rd Gen. Cephalosp.s : - with or without Aminoglycosides are DOC for serious inf. caused by CEPHALOSPORINS Klebsiella , Enterobacter ,Proteus , Providencia , Serratia & haemophilus sp.s - Ceftriaxone is DOC for gonorrhea & lyme disease & also for Salmonella inf. ( Typhoid fever ) . -Meningitis ( Ceftazidime + aminoglyc. CEPHALOSPORINS for Pseudomonas meningitis ) - Ceftriaxone & Cefotaxim are good for community acquired pneumonia 4th Gen. Cephalosp.s : The Nosocomial inf.s where antb. resist. owing to extended spect. βlactamases Other β- Lactum Antibiotics With β –lactum structure that are neither penicil. nor cephalosp. Carbapenems - It contain fused β- lactum by unsaturated 5 nucleus ring syst. & containing Carbon atom instead of sulfur atom . - have broader spect. of activity than Other β- Lactum Antibiotics do most other β –lactum antb.s - These are synth. antibact. agents Imipenems : - marketed in comb. with Cilastatin a drug that ↓ degradation of imipenem by renal tubular dipeptidase . - indicated against refractory nosocom. Other β- Lactum Antibiotics infections leading to -UTI , LRTI , -Gynecological inf. -Joint inf. & -Intra abdominal inf. caused by Other β- Lactum Antibiotics Enterobacter ,Pseudomonas , Acinetobacter & anaerobic inf.( by B. fragilis & Clostr. difficil ). -orally not abs. , rapidly hydrolyzed by dipeptidase in renal tubules to nephrotoxic metabolites Other β- Lactum Antibiotics Therefore Cilastatin is combined ( it ↓ dipeptidase enz.) S/E – nausea , vomiting , seizures & cross allergy . Meropenem : It is ≡ Imipenem but is not senst. to renal dipeptidase & with less risk of Other β- Lactum Antibiotics of seizures . Ertapenem : -having longer t½ therefore given once a day . -effective in enterobacteriaceae & anaerobes . Hence useful in abdom. & pelvic inf.s. Other β- Lactum Antibiotics Monobactums : Aztreonam - it is β- lactamase resist. with spect. similar to Aminoglycoside ( G-ve aerobic bacilli ). G+ve & anaer. org. are resist. -no cross allergy to β –lactum antb. -given I.M. or I.V. dose -2 gm/d 6-8 hrly Other β- Lactum Antibiotics β – lactamase inhibitors : certain molecule can inactivate βlactamase & thus prev. the destruction of β – lactam antb. that are substrates of this enz. ( ↑ effectiveness of β – lactum antb.s ). Other β- Lactum Antibiotics -most active against Plasmid encoded β- lactamase e.g.Clavulanic acid , Sulbactum & Tazobactum . - They themselves have not any signif. AM activity . Other β- Lactum Antibiotics - They do not inhibit inducible type I β- lactamase induced in G-ve bacilli. Useful comb.s are : 1. Amoxycil. + Clavulanic acid – effective against β –lactamase prod. strains of Staphylococ. ,H. influenz. ,Gonococci & E. coli . Other β- Lactum Antibiotics - indicated in resist. Otitis media, sinusitis , animal bite wounds cellulitis & diabetic foot. 2. Ticarcillin + Clavul. Acid : ≡ Imipenem indicated in mixed nosocomial inf. along with Aminoglyc. Other β- Lactum Antibiotics 3. Ampicil + Sulbactum : indicated in mixed intra abdominal & pelvic inf.s .( exc. Pseud. & anaerobic inf.) . 4. Tazobactum + Piperacil.: activity against Pseudomonas is not enhanced but having broadest AM sp. Bibliography 1.Goodman & Gilman’s ,The Pharmacological Basis of Therapeutics (12th Edition). 2. Clinical Pharmacology by Lawrence (Latest edition )













































































































































![ch 14 remember thing[1]](http://s1.studyres.com/store/data/008375860_1-2c45a3b285ef35d04828b346253789f0-150x150.png)