Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Discovery and development of cephalosporins wikipedia , lookup
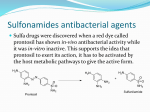
SULFONAMIDES Sulfonamides introduced in 1930s. They are bacteriostatic. Their usefulness is limited by: Bacterial resistance Formation of crystaluria Development of effective antibiotics A sulfonamide alone is not the drug of first choice for any bacterial pathogen. They act by interfering with bacterial synthesis of folic acid. Sulfamethoxazole- Trimethoprim (SMX) (TMP) Co-trimoxazole ( Bactrim, Septra ) Introduced in mid 1970s Alone, each agent is bacteriostatic Together they are bactericidals The ratio of TMP to SMX in vivo is 1:20 Currently, sulfonamides are used most frequently in this combination TMP-SMX act on 2 sequential steps of the enzymatic pathway for the synthesis of folic acid by the bacteria. MECHANISM OF ACTION P-Aminobenzoic Acid Dihydropteroate synthetase Dihydrofolate Dihydrofolate reductase Tetrahydrofolate Sulfonamides Trimethoprim Nucleic acid synthesis Absorption, Metabolism& Excretion Sulfonamides Mainly given orally Rapidly absorbed from stomach and small intestine. Widely distributed to tissues and body fluids ( including CNS, CSF ), placenta and fetus. Absorbed sulfonamides bind to serum protein ( approx. 70% ). Metabolized in the liver by the process of acetylation. Eliminated in the urine, partly as such and partly as acetylated derivative and in the feces. Trimehoprim ( TMP ) Usually given orally, alone or in combination with SMX Well absorbed from the gut Widely distributed in body fluids & tissues ( including CSF ) More lipid soluble than SMX Protein bound ( approx.40 % ) 60% of TMP or its metabolite is excreted in the urine TMP concentrates in the prostatic fluid. CLINICAL USES A.TOPICAL 1. Opthalmology- ocular infections Sulfacetamide 10- 30% 2. Ulcerative colitis Sulfasalazine ( sulfapyridine+ 5amino salicylate )-( orally, not absorbed ) 3. Infected burns Mafenide acetate ( sulfamylon cream ) Silver sulfadiazine Effective against p.aeruginosa Less effective against staphyllococci CLINICAL USES ( CONT. ) B. ORAL 1. Pneumocystis carinii pneumonia ** 2. Nocardiosis** 3. Toxoplasmosis** 4. UTIs – limited cases 5. RTIs ( H. influenza; S. pneumonia ) 6. Acute otitis media in children- L. cases 7. Prostatitis 8. Shigellosis 9. Falciparum malaria Fansidar ( sulfadoxine+ pyrimehamine ) ADVERSE EFFECTS 1.Gastrointestinal- Nausea, vomiting 2. Allergy Skin rash, urticaria,erythema multiform 3. Hematologic Acute hemolytic anemia a) hypersensitvity b) G6PD deficiency Megaloblastic anemia, leukopenia or thrombocytopenia 4. HIV patients Drug- induced fever, rashes & diarrhea 5. Drug interactions Displace bilirubin- if severe – kernicterus Potentiate warfarin, oral hypoglycemics, methotrexate CONTRAINDICATIONS 1. Pregnancy 2. Nursing mother 3. Infants under 6 weeks 4. Renal or hepatic failure 5. Blood disorders