Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
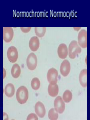
Anemia Dr.Sana Delawer Jalal Lecturer /Sulaimani College of Medicine/ Dept.of Pathology M.B.Ch.B, F.I.C.M.S. Red Cell Indices Mean Cell Volume (MCV) ► It is calculated from PCV and red cell count as follows: ► MCV = PCV/RBC ( fl) ► Normal value: 80-95 fl ► It decrease in iron deficiency anaemia and haemoglopinopathies ► It is increase in megaloblastic anaemia and chronic haemolytic anemia Mean Cell Haemoglobin Concentration (MCHC) ► It is calculated from the haemoglobin and PCV as follows: ► MCHC ► Normal = Hb/PCV g/dl value: 32-35.5 g/dl ► It is usually decreased in iron deficiency anaemia (microcytic hypochromic anaemia) Mean Cell Haemoglobin (MCH) ► It is calculated from the haemoglobin and erythrocyte count as follows: ► MCH = Hbx10/RBC ► Normal ► It pg value: 27-32 pg is decrease in iron deficiency anemia and thalassaemia (microcytic hypochromic anemia) ► It is recognized by the pale colour of the red cell in the peripheral blood film ► It is increase in macrocytic anemia (vitamin B 12 and folic acid) Red Cell Distribution width (RDW) ► RDW reflects the variation of RBCs volume it is usually performed by modern analysers ► Normal RDW varies between 12 to 17 ► Severe iron deficiency anemia is associated with increased RDW ► Thalassemia and anemia of chronic disease are associated with normal RDW Definition Anemia is a decrease in the number of RBCs, Hb content, or Hematocrit below the lower limit of the normal range for the age and sex of the individual ► In adults, the lower extreme of the normal haemoglobin is taken as 13.0 g/ dl for males and 11.5 g/dl for female ► Newborn infants have higher haemoglobin level and, therefore, 15 g/dl is taken as the lower limit at birth Classification of Anemia ► Several types of classifications of anemia's have been proposed ► Two of the widely accepted classifications are based on : ► The pathophysiology ► The morphology The Pathophysiological Classification Depending upon the pathophysiologic mechanism, anemias are classified into 3 groups: ► I. Anemia due to increased blood loss. ► II. ► III. Anemias due to impaired red cell production. Anemias due to increased red cell destruction .(Haemolytic ) The Morphological Classification Based on: 1. Red cell size, 2. Haemoglobin content 3. Red cell indices Anaemias are classified into 3 types: ► I. Microcytic, hypochromic ► II. Normocytic, normochromic ► III. Macrocytic, normochromic Simplified Classification Of Anemias 1. Deficiency anemias 2. Aplastic anemia 3. Hemolytic anemias 4. Secondary anemias The Pathophysiological Classification Impaired Red Cell Production A. Disturbance of proliferation and differentiation of stem cells ( aplastic anemia, pure red cell aplasia) B. Disturbance of proliferation and maturation of erythrocytes: 1.Defective DNA synthesis (megaloblastic anemias) 2.Defective Hb synthesis: a/. Deficient heme synthesis (iron deficiency) b/. .Deficient globin synthesis (thalassemia) 3. Unknown or multiple mechanisms (anemia of chronic disease, anemia of marrow replacement) Increased Rate Of Destruction Intrinsic abnormalities Hereditary 1. Red cell membrane defects (Hereditary spherocytosis, Hereditary eliptocytosis) 2. Red cell enzyme deficiencies a/. Glycolytic enzymes: pyruvate kinase, hexokinase b/. Enzymes of hexose monophosphate shunt: G-6PD, glutathione synthetase. 3. Disorders of globin synthesis a/. Deficient globin synthesis (thalassemia) b/. Structurally abnormal globin synthesis (sickle cell anemia, unstable hemoglobins) Acquired 1. Membrane defect: paroxysmal nocturnal hemoglobinuria Increased Destruction Extrinsic Abnormalities 1. Antibody Mediated a/. Autoantibodies (idiopathic, drug-associated, SLE, malignancies) b/. Alloantibodies (transfusion reactions, erythroblastosis fetalis) 2. Mechanical Trauma of RBCs a/. Microangiopathic hemolytic anemias (thrombotic thrombocytopenic purpura,hemolytic –uremic syndrome ) b/. Cardiac traumatic hemolytic anemia 3. Chemicals and Micro organisms 4. Sequestration in mononuclear phagocytic system - hypersplenism Morphologic Classification Of Anemias Type MCV MCHC Common cause ____________________________________________________ ► Macrocytic anemia Microcytic anemia - hypochromic - normochromic Normocytic anemia - normochromic increased decreased decreased or normal normal normal Vitamin B12 deficiency Folic acid deficiency decreased Iron deficiency Thalassemia normal Spherocytosis normal Aplastic anemia Chronic renal failure Some hemolytic anemia Microcytic Anemia Normocytic Macrocytic Classification of anemias using MCV Iron Deficiency Anemia Thalassemia Sideroblastic Anemia Microcytic Anemia MCV<80 fl Anemia of Chronic Disorder Lead Poisoning Stem cells defects/ Reduced Erythropoiesis Normocytic Anemias 80-95 fl Intrinsic Hemolytic Anemias Extrinsic Causes Intrinsic Defects Extrinsic Megaloblastic anemia Hypothyrodisim Alcoholism Macrocytic Anemias MCV> 95 fl Drugs Myelodysplastic syndrome Liver Disease Hypochromic Microcytic Normochromic Normocytic Laboratory Investigation ► Anemia is not a diagnosis, but a sign of underlying disease ► The objective of the laboratory is to : determine the type of anemia as an aid in discovering the cause Laboratory Investigation-cont. ► Screening is usually done with the CBC or "complete blood count" ► Most laboratories now use automated, multiparameter instruments which will provide results for the following parameters: ► Hemoglobin Hematocrit Red cell count MCV , MCH ,MCHC RDW White cell and platelet count Differentia WBC count. ► ► ► ► ► ► l Laboratory Investigation of Hemolytic anemia ► These are dividing into 4 groups: I-Tests show increased red cell breakdown II- Tests show increased red cell production III- Tests show damage to red cells IV- Tests show shortened red cell life span Tests Show Increased Red Cells Breakdown ► Serum bilirubin-unconjugated (indirect)bilirubin is raised ► Urine Urobilinogen is raised ► Faecal Stercobilinogen is raised ► Serum haptoglobin ( α globulin binding protein) is reduced or absent ► Plasma lactic acid dehydrogenase is raised ► Evidence of intravascular haemolysis in the form of haemoglobinaemia, haemoglobinuria, haemosiderinuria Tests Show Increased Red Cells Production. ► Reticulocyte count reveals reticulocytosis which indicate marrow erythroid hyperplasia ► Routine blood film shows macrocytosis, polychromasia, and normoblasts ► Bone marrow show erythroid hyperplasia ► X ray of bones shows evidence of expansion of marrow spaces especially in tubular bones and skull Tests Revealing Damages To RBCs ► Routine blood film shows a variety of abnormal morphological appearances of red cells ► Osmotic fragility is increased ► Autohaemolysis test ► Coomb's antiglobulin test ► Electrophoresis for abnormal haemoglobin ► Estimation of HbA2 Tests Show Shortened Red Cell Life Span by Cr51 labeling method normal RBC life span of 120 days is shortened to 20-40 days in moderate haemolysis and 5-20 days in severe haemolysis ► Tested Special Investigations ► Biochemical Tests biochemical tests are aimed to identifying: 1-Depleted cofactors necessary for normal hematopoiesis (iron, ferritin, folate, B12). 2-Abnormally functioning enzyme (glucose-6-phosphate dehydrogenase, pyruvate kinase), or 3-Abnormal function of the immune system (the direct antiglobulin [Coombs'] test). Thank you