Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Blood–brain barrier wikipedia , lookup
History of neuroimaging wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Endocannabinoid system wikipedia , lookup
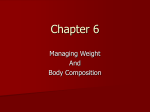
Molecular neuroscience wikipedia , lookup
Metastability in the brain wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Neuroanatomy wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Circumventricular organs wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Eating disorder wikipedia , lookup
Selfish brain theory wikipedia , lookup
Haemodynamic response wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
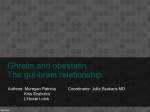
Ingestive Behavior Chapter 12 1 COPYRIGHT © ALLYN & BACON 2012 Physiological Regulatory Mechanisms: Drinking • Regulation of the fluid that bathes our cells is part of a process called homeostasis (“similar standing”). • Homeostasis (home ee oh stay sis) • the process by which the body’s substances and characteristics (such as temperature and glucose level) are maintained at their optimal level • System Variable • a variable that is controlled by a regulatory mechanism; for example, temperature in a heating system • Set Point • the optimal value of the system variable in a regulatory mechanism 2 3 Eating: Some Facts about Metabolism • The short-term reservoir is located in the cells of the liver and the muscles, and it is filled with a complex, insoluble carbohydrate called glycogen. • For simplicity, I will consider only one of these locations: the liver. • Glycogen (gly ko jen) • a polysaccharide often referred to as animal starch; stored in liver and muscle; constitutes the short-term store of nutrients 4 Eating: Some Facts about Metabolism • Cells in the liver convert glucose (a simple, soluble carbohydrate) into glycogen and store the glycogen. • They are stimulated to do so by the presence of insulin, a peptide hormone produced by the pancreas. • Insulin • a pancreatic hormone that facilitates entry of glucose and amino acids into the cell, conversion of glucose into glycogen, and transport of fats into adipose tissue 5 Eating: Some Facts about Metabolism • The fall in glucose is detected by cells in the pancreas and in the brain. • The pancreas responds by stopping its secretion of insulin and starting to secrete a different peptide hormone: glucagon. • Glucagon (gloo ka gahn) • a pancreatic hormone that promotes the conversion of liver glycogen into glucose 6 Eating: Some Facts about Metabolism • The effect of glucagon is opposite that of insulin: It stimulates the conversion of glycogen into glucose. (Unfortunately, the terms glucose, glycogen, and glucagon are similar enough that it is easy to confuse them. Even worse, you will soon encounter another one: glycerol.) (See Figure 12.11.) • Thus, the liver soaks up excess glucose and stores it as glycogen when plenty of glucose is available, and it releases glucose from its reservoir when the digestive tract becomes empty and the level of glucose in the blood begins to fall. 7 8 Eating: Some Facts about Metabolism • Our long-term reservoir consists of adipose tissue (fat tissue). • Adipose tissue is found beneath the skin and in various locations in the abdominal cavity. • This reservoir is filled with fats or, more precisely, with triglycerides. • Triglyceride (try gliss er ide) • the form of fat storage in adipose cells; consists of a molecule of glycerol joined with three fatty acids 9 Eating: Some Facts about Metabolism • Triglycerides are complex molecules that contain glycerol (a soluble carbohydrate, also called glycerine) combined with three fatty acids (stearic acid, oleic acid, and palmitic acid). • Glycerol (gliss er all) • a substance (also called glycerine) derived from the breakdown of triglycerides, along with fatty acids; can be converted by the liver into glucose • Fatty Acid • a substance derived from the breakdown of triglycerides, along with glycerol; can be metabolized by most cells of the body except for the brain 10 11 What Starts a Meal? Signals from the Stomach • The gastrointestinal system (especially the stomach) releases a peptide hormone called ghrelin (Kojima et al., 1999). • Ghrelin (grell in) • a peptide hormone released by the stomach that increases eating; also produced by neurons in the brain • The name ghrelin is a contraction of GH releasin, which reflects the fact that this peptide is also involved in controlling the release of growth hormone, usually abbreviated as GH. 12 •Ghrelin is a potent stimulator of food intake, and it even stimulates thoughts about food. •Schmid et al. (2005) found that a single intravenous injection of ghrelin not only enhanced appetite in normal subjects—it also elicited vivid images of foods that the subjects liked to eat. 13 What Starts a Meal? Signals from the Stomach • Ghrelin secretion is suppressed when an animal eats or when an experimenter infuses food into the animal’s stomach. • Injections of nutrients into the blood do not suppress ghrelin secretion, so the release of the hormone is controlled by the contents of the digestive system and not by the availability of nutrients in the blood (Schaller et al., 2003). 14 What Starts a Meal? Signals from the Stomach • Williams et al. (2003) operated on rats and installed devices similar to miniature blood-pressure cuffs around the pylorus, the junction between the stomach and the duodenum. • The duodenum is the uppermost part of the small intestine. • Duodenum • the first portion of the small intestine; attached directly to the stomach • When a cuff was inflated, it would compress the pylorus and prevent the contents of the stomach from leaving. • Surprisingly, Williams and her colleagues found that an infusion of food into the stomach would not suppress the secretion of ghrelin when the cuff was inflated. • However, when the pylorus was open, an infusion of food into the stomach, which could then reach the small intestine, did suppress ghrelin secretion. • Thus, although the stomach secretes ghrelin, its secretion appears to be controlled by receptors present in the upper part of the small intestine, not in the stomach itself. 15 What Starts a Meal? Metabolic Signals • When (nonradioactive) 2-DG is given in large doses, it interferes with glucose metabolism by competing with glucose for access to the mechanism that transports glucose through the cell membrane and for access to the enzymes that metabolize glucose. • Both hypoglycemia and 2-DG cause glucoprivation; that is, they deprive cells of glucose. • And glucoprivation, whatever its cause, stimulates eating. • Glucoprivation • a dramatic fall in the level of glucose available to cells; can be caused by a fall in the blood level of glucose or by drugs that inhibit glucose metabolism 16 What Starts a Meal? Metabolic Signals • Hunger can also be produced by causing lipoprivation—depriving cells of lipids. More precisely, they are deprived of the ability to metabolize fatty acids through injection of a drug such as mercaptoacetate. • Lipoprivation • a dramatic fall in the level of fatty acids available to cells; usually caused by drugs that inhibit fatty acid metabolism 17 What Starts a Meal? Metabolic Signals • Novin, VanderWeele, and Rezek (1973) suggested that receptors in the liver can stimulate glucoprivic hunger; when these neurons are deprived of nutrients, they cause eating. • The investigators infused 2-DG into the hepatic portal vein. • Hepatic Portal Vein • the vein that transports blood from the digestive system to the liver 18 What Starts a Meal? Metabolic Signals • This vein brings blood from the intestines to the liver; thus, an injection of a drug into this vein (an intraportal infusion) delivers it directly to the liver. (See Figure 12.14.) • The investigators found that the intraportal infusions of 2-DG caused immediate eating. • When they cut the vagus nerve, which connects the liver with the brain, the infusions no longer stimulated eating. • Thus, the brain receives the hunger signal from the liver through the vagus nerve. 19 20 What Stops a Meal? Intestinal Factors • The duodenum controls the rate of stomach emptying by secreting a peptide hormone called cholecystokinin (CCK). • Cholecystokinin (CCK) (coal i sis toe ky nin) • a hormone secreted by the duodenum that regulates gastric motility and causes the gallbladder (cholecyst) to contract; appears to provide a satiety signal transmitted to the brain through the vagus nerve • This hormone receives its name from the fact that it causes the gallbladder (cholecyst) to contract, injecting bile into the duodenum. (Bile breaks fats down into small particles so that they can be absorbed from the intestines.) • CCK is secreted in response to the presence of fats, which are detected by receptors in the walls of the duodenum. • In addition to stimulating contraction of the gallbladder, CCK causes the pylorus to constrict and inhibits gastric contractions, thus keeping the stomach from giving the duodenum more food. 21 What Stops a Meal? Intestinal Factors • CCK does not act directly on the brain; instead, it acts on receptors located in the junction between the stomach and the duodenum (Moran et al., 1989). • South and Ritter (1988) found that the appetite-suppressing effect of CCK was abolished by the application of capsaicin to the vagus nerve. • Capsaicin, a drug extracted from chili peppers, destroys sensory axons in the vagus nerve. • This finding indicates that signals from CCK receptors are transmitted to the brain via the vagus nerve. 22 What Stops a Meal? Intestinal Factors • As we saw earlier in this chapter, secretion of ghrelin by the stomach provides a signal that increases hunger. • Once a meal begins and food starts to enter the duodenum, the secretion of ghrelin is suppressed. • The suppression of a hunger signal could well be another factor that brings a meal to its end. • Investigators have discovered an chemical produced by cells in the gastrointestinal tract that appears to serve as an additional satiety signal. • This chemical, peptide YY3–36 (PYY), is released by the small intestine after a meal in amounts proportional to the calories that were just ingested (Pedersen-Bjergaard et al., 1996). 23 What Stops a Meal? Long-Term Satiety: Signals from Adipose Tissue • Researchers in several laboratories reported the discovery of the cause of the obesity (Campfield et al., 1995; Halaas et al., 1995; Pelleymounter et al., 1995). • A particular gene, called OB, normally produces a peptide hormone that has been given the name leptin (from the Greek word leptos, “thin”). • Leptin • a hormone secreted by adipose tissue; decreases food intake and increases metabolic rate, primarily by inhibiting NPY-secreting neurons in the arcuate nucleus • Leptin is normally secreted by well-nourished fat cells. Because of a genetic mutation, the fat cells of ob mice are unable to produce leptin. 24 What Stops a Meal? Long-Term Satiety: Signals from Adipose Tissue • Leptin has profound effects on metabolism and eating, acting as an antiobesity hormone. • If ob mice are given daily injections of leptin, their metabolic rate increases, their body temperature rises, they become more active, and they eat less. • As a result, their weight returns to normal. Figure 12.18 shows a picture of an untreated ob mouse and an ob mouse that has received injections of leptin. (See Figure 12.18.) 25 26 Brain Mechanisms Hypothalamus • Melanin-Concentrating Hormone (MCH) • a peptide neurotransmitter found in a system of lateral hypothalamic neurons that stimulate appetite and reduce metabolic rate • Orexin • a peptide neurotransmitter found in a system of lateral hypothalamic neurons that stimulate appetite and reduce metabolic rate • Researchers refer to MCH and orexin as orexigens, “appetite-inducing chemicals.” Injections of either of these peptides into the lateral ventricles or various regions of the brain induce eating. • If rats are deprived of food, production of MCH and orexin in the lateral hypothalamus increases (Qu et al., 1996; Sakurai et al., 1998; Dube, Kalra, and Kalra, 1999). • Of these two orexigenic hypothalamic peptides, MCH appears to play the more important role in stimulating feeding 27 28 Brain Mechanisms Hypothalamus • An empty stomach, glucoprivation, or lipoprivation arises from detectors in the abdominal cavity and brain stem. • How do these signals activate the MCH and orexin neurons of the lateral hypothalamus? • Part of the pathway involves a system of neurons that secrete a neurotransmitter called neuropeptide Y (NPY), an extremely potent stimulator of food intake (Clark et al., 1984). • Infusion of NPY into the hypothalamus produces ravenous, almost frantic eating. 29 Brain Mechanisms Hypothalamus • In addition, NPY neurons send a projection of axons to the paraventricular nucleus (PVN), a region of the hypothalamus where infusions of NPY affect metabolic functions, including the secretion of insulin (Bai et al., 1985). • Paraventricular Nucleus (PVN) • a nucleus of the hypothalamus located adjacent to the dorsal third ventricle; contains neurons involved in control of the autonomic nervous system and the posterior pituitary gland 30 Brain Mechanisms Hypothalamus • The terminals of hypothalamic NPY neurons release another orexigenic peptide in addition to neuropeptide Y: agouti-related peptide, otherwise known as AGRP (Hahn et al., 1998). • Agouti-Related Protein (AGRP) • a neuropeptide that acts as an antagonist at MC-4 receptors and increases eating • Infusion of a very small amount of this peptide into the third ventricle of rats produces an increase in food intake that lasts for six days (Lu et al., 2001). 31 Brain Mechanisms Hypothalamus • I should briefly mention one other category of orexigenic compounds: the endocannabinoids. (See Di Marzo and Matias, 2005, and Bellocchio, 2010, for reviews of the evidence cited in this section.) • One of the effects of the THC contained in marijuana is an increase in appetite— especially for highly palatable foods. • The endocannabinoids—whose actions are mimicked by THC—stimulate eating, apparently by increasing the release of MCH and orexin. 32 33 Obesity • Obesity is a widespread problem that can have serious medical consequences. • In the United States, approximately 67 percent of men and 62 percent of women are overweight, which is defined as body mass index (BMI) of over 25. • In the past twenty years, the incidence of obesity, defined as a BMI of over 30, has doubled in the population as a whole and has tripled for adolescents. 34 35 Obesity Possible Causes • Indeed, obese people already have elevated blood levels of leptin, and additional leptin has no effect on their food intake or body weight. • However, several investigators have suggested that a fall in blood levels of leptin should be regarded as a hunger signal. • That is, a low level of leptin increases the release of orexigenic peptides and decreases the release of anorexigenic peptides. • And as Flier (1998) suggests, people with a thrifty metabolism should show resistance to a high level of leptin, which would permit weight gain in times of plenty. • People with a spendthrift metabolism should not show leptin resistance, and should eat less as their level of leptin rises. 36 Obesity Treatment • Obesity is extremely difficult to treat; the enormous financial success of diet books, health spas, and weight reduction programs attests to the trouble people have in losing weight. • More precisely, many programs help people to lose weight initially, but then the weight is quickly regained. • Kramer et al. (1989) reported that 4 to 5 years after participating in a 15-week behavioral weight-loss program, fewer than 3 percent of the participants managed to maintain the weight loss they had achieved during the program. 37 Obesity Treatment • Surgeons have become involved in trying to help obese people lose weight. • The procedures they have developed (called bariatric surgery, from the Greek barys, “heavy,” and iatrikos, “medical”) are designed to reduce the amount of food that can be eaten during a meal or interfere with absorption of calories from the intestines. • Bariatric surgery has been aimed at the stomach, the small intestine, or both. • The most effective form of bariatric surgery is a special form of gastric bypass called the Roux-en-Y gastric bypass, or RYGB. • This procedure produces a small pouch in the upper end of the stomach. • The jejunum (the second part of the small intestine, immediately “downstream” from the duodenum) is cut, and the upper end is attached to the stomach pouch. 38 Obesity Treatment • One important reason for the success of the RYGB procedure appears to be that it disrupts the secretion of ghrelin. • The procedure also increases blood levels of PYY (Chan et al., 2006; Reinehr et al., 2006). • Both of these changes would be expected to decrease food intake: A decrease in ghrelin should reduce hunger, and an increase in PYY should increase satiety. 39 40 41 Obesity Treatment • Some serotonergic agonists suppress eating. However, a drug used for this purpose, fenfluramine, was found to have hazardous side effects (including pulmonary hypertension and damage to the valves of the heart), so the drug was withdrawn from the market in the United States (Blundell and Halford, 1998). • Fenfluramine acts by stimulating the release of 5-HT. Another drug, sibutramine, has similar therapeutic effects on eating—but a study of people who were taking the drug found increased incidence of heart attacks and strokes, so this drug, too, was withdrawn from the market (Li and Cheung, 2011). 42 43 Anorexia Nervosa/Bulimia Nervosa • Most people, if they have an eating problem, tend to overeat. • However, some people, especially among adolescent women, have the opposite problem: They eat too little, even to the point of starvation. • This disorder is called anorexia nervosa. • Anorexia Nervosa • a disorder that most frequently afflicts young women; exaggerated concern with being overweight that leads to excessive dieting and often compulsive exercising; can lead to starvation 44 Anorexia Nervosa/Bulimia Nervosa • Another eating disorder, bulimia nervosa, is characterized by a loss of control of food intake. (The term bulimia comes from the Greek bous, “ox,” and limos, “hunger.”) • People with bulimia nervosa periodically gorge themselves with food, especially dessert or snack food, and especially in the afternoon or evening. • These binges are usually followed by self-induced vomiting or the use of laxatives, along with feelings of depression and guilt. • Bulimia Nervosa • bouts of excessive hunger and eating, often followed by forced vomiting or purging with laxatives; sometimes seen in people with anorexia nervosa 45 Anorexia Nervosa/Bulimia Nervosa • Episodes of bulimia are seen in some patients with anorexia nervosa. • The incidence of anorexia nervosa is estimated at 0.5–2 percent; that of bulimia nervosa at 1–3 percent. • Women are ten to twenty times more likely than men to develop anorexia nervosa and approximately ten times more likely to develop bulimia nervosa. (See Klein and Walsh, 2004.) 46 Anorexia Nervosa/Bulimia Nervosa Possible Causes • Anorexia is a serious disorder. • Five to ten percent of people with anorexia die of complications of the disease or of suicide. Many anorexics suffer from osteoporosis, and bone fractures are common. • When the weight loss becomes severe enough, anorexic women cease menstruating. • Some disturbing reports (Artmann et al., 1985; Herholz, 1996; Kingston et al., 1996; Katzman et al., 2001) indicate the presence of enlarged ventricles and widened sulci in the brains of anorexic patients, which indicate shrinkage of brain tissue. 47 Anorexia Nervosa/Bulimia Nervosa Possible Causes • Blood levels of NPY are elevated in patients with anorexia. Nergårdh et al. (2007) found that infusion of NPY into the cerebral ventricles further increased the time spent running in rats on a restricted feeding schedule. • Normally, NPY stimulates eating (as it does in rats with unlimited access to food), but under conditions of starvation, it stimulates wheel-running activity instead. • The likely explanation for this phenomenon is that if food is not present, NPY increases the animals’ activity level, which would normally increase the likelihood that they would find food. 48 Anorexia Nervosa/Bulimia Nervosa Treatment • Anorexia is very difficult to treat successfully. • Cognitive behavior therapy, considered by many clinicians to be the most effective approach, has a success rate of less than 50 percent and a relapse rate of 22 percent during a 1-year treatment period (Pike et al., 2003). • A meta-analysis by Steinhausen (2002) indicates that the success rate in treating anorexia has not improved in the last fifty years. 49