Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
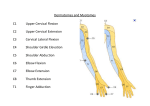
15_CH01_FINAL.indd 1 c h a p te r Normal Values and Assessments 1 ASIA Classification of Spinal Cord Injury •• The American Spinal Injury Association (ASIA) has developed a spinal injury classification system based on specific motor and sensory assessments as depicted in the figure on page 2. •• Motor function is determined by manual muscle testing of 10 key muscles. Results of manual muscle tests are expressed numerically. • Dermatomal sensation assessment for pinprick and light touch is performed and scored numerically. • The ASIA Impairment Scale, using letters A to E, represents the overall classification of the spinal injury. 1 4/23/12 12:28:49 P 2 Chapter 1 Normal Values and Assessments STANDARD NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY C2 C3 C4 C5 C6 C7 C8 T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 L3 L4 L5 S1 S2 S3 S4-5 R Totals (Maximum 50 L MOTOR Key muscles Elbow flexors Wrist extensors Elbow extensors Finger flexors (distal phalanx of middle finger) Finger abductors (little finger) 0 = total paralysis 1 = palpable or visible contraction 2 = active movement, gravity eliminated 3 = active movement, against gravity 4 = active movement, against some resistance 5 = active movement, against full resistance NT = not testable Hip flexors Knee extensors Ankle dorsiflexors Long toe extensors Ankle plantar flexors Voluntary anal contraction (Yes/No) + = 50 Motor score function (Maximum 56 100) NEUROLOGICAL LEVEL R The most Sensory caudal segment Motor with normal C2 C3 C4 C5 C6 C7 C8 T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 L3 L4 L5 S1 S2 S3 S4-5 Totals LIGHT TOUCH R L L Complete or incomplete? Incomplete = Any sensory or motor function in S4-S5 ASIA IMPAIRMENT SCALE + 56 P R = 5 ZONE OF PARTIAL PRESERVATION Caudal extent of partially innervated segments Figure 1.1 Standard Neurological Classification of Spinal Cord Injury Source: Reproduced with permission of the American Spinal Injury Association (2005). This form may be copied freely but should not be altered without permis sion from the American Spinal Injury Association. 15_CH01_FINAL.indd 2 ASIA Standard Neurological Classification of Spinal Cord Injury Chart4/23/12 12:28:50 P ASSIFICATION OF TOR uscles halanx of middle finger) finger) ble contraction nt, ed nt, nt, esistance nt, tance ction (Yes/No) plete or mplete? plete = Any sensory or unction in S4-S5 IMPAIRMENT LE 3 ASIA Classification of Spinal Cord Injury C2 C3 C4 C5 C6 C7 C8 T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 L3 L4 L5 S1 S2 S3 S4-5 Totals LIGHT TOUCH R L (Maximum 56 SENSORY Key sensory points PIN PRICK R L 0 = absent 1 = impaired 2 = normal NT = not testable = Key sensory point C2 C3 C4 T2 T2 T3 T4 T5 T6 T7 T8 T9 T10 C5 T1 C6 C5 T1 C6 T11 Palm L1 L1 C8 C8 Dorsum Palm T12 L2 C6 L2 C6 C7 C7 Dorsum L3 L3 S3 S3 S4-5 L4 L4 L5 L2 L5 L2 L3 L3 S2 S2 S1 S1 S1 C2 L4 S1 S1 L5 L5 C3 C4 Any anal sensation (Yes/No) + + 56 = 56 ZONE OF PARTIAL PRESERVATION Caudal extent of partially innervated segments = 56) Pin prick score (Max 112) Light touch score (Max 112) R L Sensory Motor Figure 1.1 continued tion of Spinal Cord Injury 15_CH01_FINAL.indd 3 Chart 4/23/12 12:28:50 P 15_CH01_FINAL.indd 4 4 Chapter 1 Normal Values and Assessments A = Complete: No motor or sensory function is preserved in the sacral segments S4–S5. B = Incomplete: Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4–S5. C = Incomplete: Motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3. D = Incomplete: Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more. E = Normal: Motor and sensory function are normal. Clinical Syndromes Central Cord Brown-Séquard Anterior Cord Conus Medullaris Cauda Equina Figure 1.2 ASIA Impairment Scale Source: Reproduced with permission of the American Spinal Injury Association (2005). 4/23/12 12:28:50 P 15_CH01_FINAL.indd 5 Table 1.1 Blood—Complete Blood Count (CBC) continues Infants: 30–60% Children: 30–49% Men: 37–49% Women: 36–46% Hematocrit (HCT) Hematocrit is the percent of whole blood composed of erythrocytes. Exercise may be restricted at values of ≤25%. The ESR is the rate at which erythrocytes settle out of blood plasma in 1 hour. A high rate is indicative of infection or inflammation Children: 1–13 mm/h Men: 0–17 mm/h Women: 1–25 mm/h Erythrocyte Sedimentation Rate (ESR/Sed. Rate) Description/Implications/Red Flag Values Individuals with lower-than-normal values have anemia. Anemia symptoms: fatigue, weakness, SOB, dizziness, tachycardia Individuals with higher-than-normal values have polycythemia. Polycythemia symptoms: SOB, headache, dizziness, itchiness. Values Red Blood Cells (RBCs) (erythrocytes) Infants: 5.5–6.0 million/mm3 Children: 4.6–4.8 million/mm3 Men: 4.5–5.3 million/mm3 Women: 4.1–5.1 million/mm3 Assessment Component Note: Normal values may vary from one laboratory to another. The values presented in these charts should not be considered absolute. Table 1.1 Blood—Complete Blood Count (CBC) 5 4/23/12 12:28:50 P 15_CH01_FINAL.indd 6 Table 1.1 Blood—Complete Blood Count (CBC), continued Values Infants: 17–19 g/dL Children: 14–17 g/dL Men: 13–18 g/dL Women: 12–16 g/dL Units: cells/mm3 Infants: 200,000– 475,000 Children: 150,000– 400,000 Adults: 150,000–400,000 Units: cells/mm3 Children: 4,500–14,500 Adults: 4,500–11,000 Assessment Component Hemoglobin (HGB) Platelets White Blood Cells (WBCs) White blood cells play a crucial role in the body’s immune reaction. Exercise may not be permitted at values of ≤5,000 cells/mm3. Platelets play a key role in the initiation of the clotting process within damaged blood vessels. Exercise may be cautiously performed with values of 21,000– 50,000 cells/mm3. Exercise may be contraindicated at values of ≤20,000 cells/mm3. HGB measures the oxygen-carrying capacity of RBCs. Low values between 8 and 10 g/dL are associated with poor exercise tolerance, increased fatigue, and tachycardia. Description/Implications/Red Flag Values Note: Normal values may vary from one laboratory to another. The values presented in these charts should not be considered absolute. 6 Chapter 1 Normal Values and Assessments 4/23/12 12:28:50 P 15_CH01_FINAL.indd 7 Differential WBC Count Neutrophils: 1,800–7,000 cells/mm3 Lymphocytes: 1,500–4,000 cells/mm3 Monocytes: 0–800 cells/mm3 Eosinophils: 0–450 cells/mm3 Basophils: 0–200 cells/mm3 The various white blood cells play different roles in the immune process. They exist in stereotypical proportions. Table 1.1 Blood—Complete Blood Count (CBC) 7 4/23/12 12:28:50 P 15_CH01_FINAL.indd 8 Table 1.2 Blood—Electrolytes Values Children: 3.5–5.5 mEq/L Adults: 3.5–5.3 mEq/L 135–145 mEq/L Children: 98–105 mEq/L Adults: 95–105 mEq/L Children: 9–11.5 mg/dL Adults: 9–11 mg/dL Children: 1.6–2.6 mEq/L Adults: 1.5–2.5 mEq/L Assessment Component Potassium Sodium Chloride Calcium Magnesium Hypocalcemia: paresthesias, muscle spasms Hypercalcemia: lethargy, muscle weakness, flaccidity, bone pain Hypomagnesemia: muscle cramping, tetany, confusion Hypermagnesemia: decreased reflexes, muscle weakness, lethargy Hypokalemia: dizziness, muscle weakness, fatigue, leg cramps Hyperkalemia: muscle weakness, flaccid paralysis, paresthesias Hyponatremia: muscle twitching, weakness Hypernatremia: fever, convulsions Chloride shifts are most often associated with shifts in sodium. Description/Implications/Red Flag Values Note: Normal values may vary from one laboratory to another. The values presented in these charts should not be considered absolute. 8 Chapter 1 Normal Values and Assessments 4/23/12 12:28:50 P 15_CH01_FINAL.indd 9 Table 1.3 Blood—Prothrombin Time Values 12–15 sec 30–40 sec Assessment Component Prothrombin Time (PT) Partial Prothrombin Time (PTT) This assessment measures the clotting ability of blood. Measures of 1.5 to 2.5 times the reference range are considered therapeutic. Physical therapy may be contraindicated at values of ≥2.5 times the reference range in individuals not taking anticoagulants and values of ≥2.5–3.0 times the reference range for those taking anticoagulant medications. Description/Implications/Red Flag Values Note: Normal values may vary from one laboratory to another. The values presented in these charts should not be considered absolute. Table 1.3 Blood—Prothrombin Time 9 4/23/12 12:28:50 P 10 Chapter 1 Normal Values and Assessments SENSORY Key sensory points = Key sensory point C2 C3 C4 T2 T1 C6 L1 Palm Dorsum C8 C6 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 C5 C5 T1 C6 T12 L1 L2 L2 L3 L3 Palm C6 C8 C7 C7 Dorsum S3 S3 S4-5 L4 L4 L5 L5 L2 L2 L3 L3 S2 S2 S1 S1 S1 C2 L4 S1 L5 S1 L5 C3 C4 Figure 1.3 Key Sensory Points Source: Reproduced with permission of the American Spinal Injury Association (2005). ASIA Standard Neurological Classification of Spinal Cord Injury Chart Jones and Bartlett Publishers Elizabeth Morales Illustration Services Figure 38115_CH01_0103.eps Date 04-13-06 15_CH01_FINAL.indd 10 4/23/12 12:28:51 P 15_CH01_FINAL.indd 11 Range of Motion—Lower Extremity Percentages 11 Table 1.4 Range of Motion—Lower Extremity and Spine Note: Values are according to the American Academy of Orthopedic Surgeons. Joint Hip Hip Flexion Extension Adduction Abduction Lateral rotation Medial rotation Flexion Dorsiflexion Plantar flexion Inversion Eversion Flexion Extension Rotation Lateral flexion Flexion Extension Rotation Lateral flexion Knee Ankle Cervical Thoracolumbar Range of Motion (in degrees) 0–120 0–30 0–30 0–45 0–45 0–45 0–150 0–20 0–50 0–35 0–15 0–45 0–45 0–60 0–45 0–80 0–25 0–35 0–45 Range of Motion—Lower Extremity Percentages In some instances, it may be preferable to report measured range of motion as a percentage of normal values. This may be especially true when setting or interpreting long- and short-term goals and for report ing to third-party payers or nonphysical therapy personnel. The chart on page 16 provides percentage approximations in 5% intervals. An approximate percentage can be determined by choosing the number from the chart that is closest to the measured joint range (e.g., 95° of knee flexion represents an approximate 30% deficit). 4/23/12 12:28:51 P 15_CH01_FINAL.indd 12 Hip flex. Abd. Add. Ext. rot. Int. rot. Ext. Knee flex. Ankle dorsi. Plantar Invers. Evers. 120 114 108 102 96 90 84 45 32 41 38 36 34 32 30 29 27 26 24 23 21 45 42 41 38 36 34 32 45 42 41 38 36 34 32 30 29 27 26 24 23 21 150 143 135 128 120 113 105 20 19 18 17 16 15 14 50 48 45 43 40 38 35 35 33 32 30 28 26 25 15 14 14 13 12 11 11 78 29 20 29 29 20 98 13 33 23 10 72 27 18 27 27 18 90 12 30 21 9 66 25 17 25 25 17 83 11 28 19 8 60 23 15 23 23 15 75 10 25 18 8 54 20 14 20 20 14 68 9 23 16 7 48 18 12 18 18 12 60 8 20 14 6 42 16 11 16 16 11 53 7 18 12 5 36 14 9 14 14 9 45 6 15 11 5 30 11 8 11 11 8 38 5 13 9 4 24 9 6 9 9 6 30 4 10 7 3 18 7 5 7 7 5 23 3 8 5 2 12 5 3 5 5 3 15 2 5 4 2 6 2 2 2 2 2 8 1 3 2 1 Table 1.5 Range of Motion—Lower Extremity Percentages 95 90 85 80 75 70 65 60 55 50 45 40 35 30 25 20 15 10 5 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 % of Normal 100 % of Deficit 0 12 Chapter 1 Normal Values and Assessments 4/23/12 12:28:51 P 15_CH01_FINAL.indd 13 Table 1.6 Range of Motion—Upper Extremity 13 Table 1.6 Range of Motion—Upper Extremity Note: Values are according to the American Academy of Orthopedic Surgeons. Joint Motion Shoulder Flexion Extension Abduction Lateral rotation Medial rotation Flexion Pronation Supination Flexion Extension Radial deviation Ulnar deviation CMC flexion CMC extension CMC abduction MCP flexion IP flexion MCP flexion MCP hyperextension MCP abduction PIP flexion DIP flexion DIP hyperextension Elbow Complex Wrist Thumb 2nd through 5th digits Range of Motion (in degrees) 0–180 0–60 0–180 0–90 0–70 0–150 0–80 0–80 0–80 0–70 0–20 0–30 0–15 0–20 0–70 0–50 0–80 0–90 0–45 0–45 0–100 0–90 0–10 CMC=carpometacarpal; DIP=interphalangeal distal; IP=interphalangeal; MCP=metacarpophalangeal; PIP=posterior interphalangeal. 4/23/12 12:28:51 P 15_CH01_FINAL.indd 14 % of Normal % of Deficit Shoulder abd. Flexion Ext. rot. Int. rot. Extension Elbow flex. Pron./Supin. Wrist flexion Ext. Rad. dev. Uln. dev. 100 0 180 180 90 70 60 150 80 80 70 20 30 95 5 171 171 86 67 57 143 76 76 67 19 29 90 10 162 162 81 63 54 135 72 72 63 18 27 85 15 153 153 77 60 51 128 68 68 60 17 26 80 20 144 144 72 56 48 120 64 64 56 16 24 75 25 135 135 68 53 45 113 60 60 53 15 23 70 30 126 126 63 49 42 105 56 56 49 14 21 65 35 117 117 59 46 39 98 52 52 46 13 29 60 40 108 108 54 42 36 90 48 48 42 12 18 Table 1.7 Range of Motion—Upper Extremity Percentages (See rationale and use instructions on page 15.) 55 45 99 99 50 39 33 83 44 44 39 11 17 50 50 90 90 45 35 30 75 40 40 35 10 15 45 55 81 81 41 32 27 68 36 36 32 9 14 40 60 72 72 36 28 24 60 32 32 28 8 12 35 65 63 63 32 25 21 53 28 28 25 7 11 30 70 54 54 27 21 18 45 24 24 21 6 9 25 75 45 45 23 18 15 38 20 20 18 5 8 20 80 36 36 18 14 12 30 17 17 14 4 6 15 10 85 90 27 18 27 18 14 9 11 7 9 6 23 15 12 8 12 8 11 7 3 2 5 3 5 95 9 9 5 4 3 8 4 4 4 1 2 14 Chapter 1 Normal Values and Assessments 4/23/12 12:28:51 P 15_CH01_FINAL.indd 15 Thumb CMC flex. 15 CMC ext. 20 CMC abd. 70 MCP flex. 50 IP flex. 80 Digits 2-5 MCP flex. 90 MCP hypex. 45 MCP abd. 45 PIP flex. 100 DIP flex. 90 DIP hypetxt. 10 14 18 63 45 72 81 41 41 90 81 9 14 19 67 48 76 86 43 43 95 86 9 77 38 38 85 77 9 13 17 60 43 68 72 36 36 80 72 8 12 16 56 40 64 68 34 34 75 68 8 11 15 53 38 60 63 32 32 70 63 7 11 14 49 35 56 59 29 29 65 59 7 10 13 46 33 52 54 27 27 60 54 6 9 12 42 30 48 50 25 25 55 50 6 8 11 39 28 44 45 23 23 50 45 5 8 10 35 25 40 41 20 20 45 41 5 7 9 32 23 36 36 18 18 40 36 4 6 8 28 20 32 32 16 16 35 32 4 5 7 25 18 28 27 14 14 30 27 3 5 6 21 15 24 23 11 11 25 23 3 4 5 18 13 20 18 9 9 20 18 2 3 4 14 10 17 14 7 7 15 14 2 2 3 11 8 12 9 5 5 10 9 1 2 2 7 5 8 5 2 2 5 5 1 1 1 4 3 4 Table 1.7 Range of Motion—Upper Extremity Percentages 15 4/23/12 12:28:52 P 15_CH01_FINAL.indd 16 16 Chapter 1 Normal Values and Assessments Table 1.8 Manual Muscle Testing—Hip and Knee Gravity+ Gravity− Joint Motion Muscle(s) Fair Poor Hip Iliopsoas Rectus femoris Pectineus Tensor fas. latae Sartorius Gluteus maximus Hamstrings Sitting Side lying Prone Prone Side lying Abduction Gluteus medius Gluteus minimus Side lying Supine Adduction Adductor longus Adductor brevis Adductor magnus Gracilis Pectineus Piriformis Gemellus sup./inf. Obturator ext./int. Quadratus fem. Gluteus maximus Gluteus minimus Gluteus medius Tensor fas. lat. Quadriceps Hamstrings Gastrocnemius Side lying Supine Flexion Extension Lateral rot. Medial rot. Knee Extension Flexion Sitting Supine Sitting Supine Sitting Prone Side lying Side lying 4/23/12 12:28:52 P 15_CH01_FINAL.indd 17 Sitting Eversion Plantar flexion Inversion Plantar flexion Soleus Tibialis posterior Tibialis anterior Flex. digit. long. Flex. hal. long. Ext. hal. long. Peroneus longus Peroneus brevis Sitting Standing (with knee flexion) Sitting Standing Gravity+ Fair Tibialis anterior Peroneus tertius Ext. digit long. Ext. hal. long. Gastrocnemius Soleus Ankle Dorsiflexion Table 1.9 Manual Muscle Testing—Ankle Joint Motion Muscle(s) Sitting Prone (with 90° knee flexion) Sitting Prone Sitting Gravity− Poor Table 1.9 Manual Muscle Testing—Ankle 17 4/23/12 12:28:52 P 15_CH01_FINAL.indd 18 18 Chapter 1 Normal Values and Assessments Table 1.10 Manual Muscle Testing—Shoulder Gravity+ Gravity− Joint Motion Muscle(s) Fair Poor Shoulder Abduction Deltoid Supraspinatus Extension Deltoid Latissimus dorsi Teres major Flexion Deltoid Coracobrachialis Pectoralis major Horizon. Deltoid abd. Teres minor Infraspinatus Horizon. Deltoid add. Pectoralis major Lateral rot. Medial rot. Sitting Supine Prone Side lying Sitting Side lying Prone Sitting Supine Sitting Prone Teres minor Infraspinatus Deltoid Prone Deltoid Latissimus dorsi Teres major Pectoralis major Subscapularis Prone (with elbow ext.) Prone (with elbow ext.) 4/23/12 12:28:52 P 15_CH01_FINAL.indd 19 Wrist Elbow Complex Flexion Extension Pronation Supination Extension Flexion Biceps Supinator Pronator teres Pronator quad. Ext. c. rad. long. Ext. c. rad. brev. Ext. c. ulnaris Flex. carpi uln. Flex. carpi rad. Palmaris longus Biceps Brachialis Brachioradialis Triceps Anconeus Sitting (with 90° of elbow flex.) Sitting (with 90° of elbow flex.) Sitting (with forearm pronation and elbow flex.) Sitting (with forearm supination and elbow flex.) Prone (with 90° of shoulder abd.) Sitting Table 1.11 Manual Muscle Testing—Elbow and Wrist Joint Motion Muscle(s) Gravity+ Fair Gravity− Poor Sitting (with neutral forearm and elbow flex.) Sitting (with 45°–90° of shoulder flex. and 90° of elbow flex.) Sitting (with 45°–90° of shoulder flex. and 90° of elbow flex.) Sitting (with neutral forearm and elbow flex.) Sitting (with 90° of shoulder abd.) Sitting (with 90° of shoulder abd.) Table 1.11 Manual Muscle Testing—Elbow and Wrist 19 4/23/12 12:28:52 P 15_CH01_FINAL.indd 20 Apprehension Test Clunk Sign Drop Arm Test Hawkins-Kennedy Impingement Test Impingement Sign Lock Test Neer Impingement Sign O’Brien Test Speed’s Maneuver Yergason’s Test Cozen’s Test Elbow Flexion Test Golfer’s Elbow Test Mill’s Test Tinel’s Sign at elbow Shoulder Elbow Table 1.12 Special Tests Listing Joint Test Lateral epicondylitis Cubital tunnel syndrome Medial epicondylitis Lateral epicondylitis Ulnar nerve entrapment Anterior glenohumeral instability Labral disorder Rotator cuff tear Supraspinatus tendon impingement Impingement of the supraspinatus and/or long head of biceps Supraspinatus tendon impingement Subacromial impingement Superior labral tear Biceps tendon instability or tendonitis Biceps tendon instability or tendonitis Assessment 20 Chapter 1 Normal Values and Assessments 4/23/12 12:28:52 P 15_CH01_FINAL.indd 21 Wrist and Hand Froment’s Sign Murphy’s Sign Phalen’s Test Tinel’s Test Allen Test Bunnel-Littler Test Carpal Shake Test Finkelstein’s Test Radial and ulnar artery circulation Tightness of intrinsic muscles Intercarpal synovitis Stenosing tenosynovitis of abductor pollicis longus and extensor pollicis brevis Ulnar nerve entrapment of elbow and wrist Lunate dislocation Carpal tunnel syndrome Carpal tunnel syndrome continues Table 1.12 Special Tests Listing 21 4/23/12 12:28:52 P 15_CH01_FINAL.indd 22 Hip Thomas Test Trendelenburg Sign 90–90 Straight Leg Raise Craig Test Ely’s Test FABER or Patrick’s Test Fulcrum Test Ober Test Hip Piriformis Test Pelvic Drop Test Quadrant (Scour) Test Table 1.12 Special Tests Listing, continued Joint Test Hamstring tightness Assess femoral anteversion or retroversion Flexibility of rectus femoris Hip, lumbar, sacroiliac joint dysfunction or iliopsoas spasm Stress fracture of the femoral shaft Tightness of iliotibial band and tensor fascia lata Tightness of the piriformis muscle Unstable hip or weak external rotators Capsular tightness, an adhesion, myofascial restriction or loss of joint congruity Decreased flexibility of rectus femoris or iliopsoas Weakness of gluteus medius Assessment 22 Chapter 1 Normal Values and Assessments 4/23/12 12:28:52 P 15_CH01_FINAL.indd 23 Ankle Knee Anterior Draw Test Apley’s Test Apley’s Distraction Test Gravity (Godfrey) Sign Hughston’s Posterolateral Drawer Test Lachman’s Test McMurray’s Test Posterior Draw Buerger’s Test Fleiss Line Gungor Test Homans’ Sign Kleiger Test Matles Test Morton’s Test Thompson Test ACL and medial and posteromedial capsuloligamentous instability Lesion of meniscus Medial or lateral collateral ligament injury PCL injury Posterolateral instability ACL injury Lesion of medial meniscus PCL injury Poor anterior circulation Height of the medial arch Anterior displacement of the talus Deep-vein thrombosis Integrity of medial (deltoid) ligament Chronic Achilles tendon rupture Presence of neuroma or a stress fracture Acute Achilles tendon rupture continues Table 1.12 Special Tests Listing 23 4/23/12 12:28:52 P 15_CH01_FINAL.indd 24 Barré’s Test Dix-Hallpike Test Modified Sharp-Purser Test Compression Test Hyperabduction Maneuver (Wright Test) Spurling’s Test Stress Test Gaenslen’s Test Yeoman’s Test ACL=anterior cruciate ligament; PCL=posterior cruciate ligament. Sacroiliac Joint Cervical Spine Craniovertebral Table 1.12 Special Tests Listing, continued Joint Test Assessment Vertebral artery insufficiency Vestibular impairment—accumulation of utricle debris Excessive translation of atlas Brachial plexus injury Thoracic outlet compression Nerve root irritability Brachial plexus injury Sacroiliac lesion, hip pathology, or L4 nerve root lesion Problem at the sacroiliac joint 24 Chapter 1 Normal Values and Assessments 4/23/12 12:28:52 P 15_CH01_FINAL.indd 25 Positive test may indicate rotator cuff tear. Positive Test Abduct the shoulder against gravity. Instruct patient to slowly lower arm to side. The patient will not be able to lower arm smoothly and slowly; the arm will drop. Hawkins-Kennedy Positive test may indicate impingement Flex the shoulder and elbow to 90° then internally rotate the Test syndrome involving the supraspinatus. shoulder. The patient will complain of pain. I mpingement Positive test may indicate impingement When sitting, passively horizontally adduct the shoulder with arm in Sign of the supraspinatus and/or long head 90° of shoulder flexion. of the biceps. Patient will have pain at the end range. Passively and forcibly flex the shoulder. Neer Test Positive test may indicate shoulder impingement involving the biceps Patient will complain of pain. tendon. continues SHOULDER Drop Arm Test Table 1.13 Selected Special Test Descriptions Name Assessment Table 1.13 Selected Special Test Descriptions 25 4/23/12 12:28:52 P 15_CH01_FINAL.indd 26 Mill’s Test Positive test may indicate lateral epicondylitis. Positive test may indicate medial epicondylitis. Positive test may indicate bicipital tendonitis. Yergason’s Test ELBOW Golfer’s Elbow Test Positive test may indicate bicipital tendonitis. Speed’s Test Stabilize the elbow. Supinate the patient’s forearm while extending the elbow and wrist. Patient will complain of pain at the medial epicondyle. Stabilize the elbow. Ask the patient to pronate the forearm and extend and radially deviate the wrist against manual resistance. Patient will complain of pain at the lateral epicondyle. Flex the shoulder against gravity about 60° with the elbow extended and forearm supinated. Isometrically resist shoulder flexion at the forearm. Patient will complain of pain at the bicipital groove. Position the shoulder at the side and flex the elbow to 90° and pronate the forearm. Resist supination and external rotation. Patient will complain of pain at the bicipital groove. Table 1.13 Selected Special Test Descriptions, continued Name Assessment Positive Test 26 Chapter 1 Normal Values and Assessments 4/23/12 12:28:53 P 15_CH01_FINAL.indd 27 Tinel’s Sign Phalen’s Test WRIST Bunnel-Littler Test Tinel’s Test Positive test may indicate lateral epicondylitis. Positive test may indicate tightness of the intrinsic muscles of the hand or a capsular problem of the joints. Positive test may indicate carpal tunnel syndrome. Positive test may indicate a problem with the ulnar nerve. Table 1.13 Selected Special Test Descriptions continues The patient flexes both wrists and presses the dorsal surfaces against each other to maintain flexion for 1 minute. The patient will experience paresthesias along the median nerve sensory distribution. Supinate the forearm. Tap over the median nerve. The patient will experience paresthesias along the median nerve sensory distribution. Hold the MCP in extension and move the PIP into flexion. The PIP will not be able to be flexed. Flex the elbow to 90°. Tap over the ulnar nerve. Patient will complain of paresthesias along the ulnar nerve sensory distribution. 27 4/23/12 12:28:53 P 15_CH01_FINAL.indd 28 T rendelenburg Sign Thomas Test Piriformis Test HIP Ober Test Positive test may indicate tightness of Position the patient in side lying on the uninvolved limb. Abduct and the iliotibial band or tensor fascia latae. extend the uphill hip, and then release the limb. The limb will not lower to the uninvolved limb. Positive test may indicate tightness of Position the patient in side lying on the uninvolved limb. Flex the the piriformis muscle. hip to 60°–90° and the knee to 90°. Stabilize the pelvis and adduct the hip to the table. The patient will complain of pain in the buttocks. Positive test may indicate hip flexion Place patient in supine. Have patient flex both hips and knees to the contracture. chest. Instruct patient to extend one limb to the table. The patient will be unable to fully extend the limb. Positive test may indicate weakness of Have patient stand on one leg. the gluteus medius. The pelvis will drop to the noninvolved side. Table 1.13 Selected Special Test Descriptions, continued Name Assessment Positive Test 28 Chapter 1 Normal Values and Assessments 4/23/12 12:28:53 P 15_CH01_FINAL.indd 29 Positive test may indicate meniscus damage. Positive test may indicate collateral ligament damage. A pley’s Distraction Test Positive test may indicate tightness of the hamstrings. A pley’s (Compression) Test KNEE 90–90 Straight Leg Raise Test Have the patient assume the prone position and flex the knee to 90°. With the clinician’s hands on the plantar surface of the foot, internally and externally rotate the leg while pressing down. Patient will complain of pain at the knee. Have the patient assume the prone position and flex the knee to 90°. Use one hand to grasp the leg just proximal to the malleoli and distract the leg while the other hand stabilizes at the posterior thigh. Patient will complain of pain at the knee. In supine, have the patient flex the hip and knee to 90°. Using the patient’s or clinician’s hands to maintain hip flexion, extend knee as much as possible. Patient is unable to extend knee beyond –20° extension. Table 1.13 Selected Special Test Descriptions 29 4/23/12 12:28:53 P 15_CH01_FINAL.indd 30 Table 1.14 Vital Signs 36 mo–adult 2–36 mo Newborns 1y 2–6 y 8–12 y 13–16 y Adults Birth–1 mo Heart Rate (Pulse) Blood Pressure Age Group Vital Sign 70–190 beats/min 80–160 beats/min 70–125 beats/min 70–110 beats/min 60–100 beats/min 55–100 beats/min Systolic: 60–90 mm Hg Diastolic: 30–60 mm Hg Systolic: 75–130 mm Hg Diastolic: 45–90 mm Hg Systolic: 90–140 mm Hg Diastolic: 50–80 mm Hg Normal Range Note: Normal values may vary from one laboratory to another. The values presented in these charts should not be considered absolute. 30 Chapter 1 Normal Values and Assessments 4/23/12 12:28:53 P 15_CH01_FINAL.indd 31 Oxygen Saturation (as measured with a pulse oximeter) Respiratory Rate Birth–1 mo 3 mo–6 y 6–10 y 10–16 y Adults 35–55 breaths/min 20–30 breaths/min 15–25 breaths/min 12–30 breaths/min 12–20 breaths/min Normal oxygen saturation at rest or during exercise is 98%. Exercise may be contraindicated in values of ≤90%. Table 1.14 Vital Signs 31 4/23/12 12:28:53 P 15_CH01_FINAL.indd 32 32 Chapter 1 Normal Values and Assessments References American Spinal Injury Association. (2005). International standard for neurological classification of spinal cord injury. Chicago: ASIA. Dutton, M. (2008). Orthopedic examination, evaluation and intervention. Second Edition. Philadelphia: McGraw Hill. Goodman, C., Boissonault,W., & Fuller, K. (2009). Pathology: Implications for the physical therapist. Third edition. Philadelphia: Saunders. Hislop, H., & Montgomery, J. (2007). Daniels and Worthingham’s muscle testing: Techniques of manual examination. Eighth edition. Philadelphia: W.B. Saunders Company. Hoppenfeld, S. (1976). Physical examination of the spine and extremities. Norwalk, CT: Prentice Hall. Norkin, C., & White, J. (2009). Measurement of joint motion: A guide to goniometry. Fourth edition. Philadelphia: F.A. Davis. Palmer, L., & Epler, M. (1998). Fundamentals of musculoskeletal assessment techniques. Philadelphia: Lippincott. 4/23/12 12:28:53 P