Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
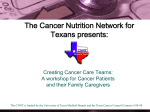
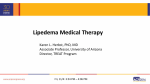
Management of Extremity Lymphedema Christopher A. Puleo, PA-C, and Marianne Luh, BS The Cutaneous Oncology Program at H. Lee Moffitt Cancer Center & Research Institute, Tampa, Fla. (C.A.P.) and Venus Medical, Inc., Palm Harbor, Fla. (M.L.) Chronic lymphedema is almost always a permanent and often progressive condition. In most cases, neither medical nor surgical means can completely relieve the effects of lymphedema. Surgical management of chronic lymphedema has high morbidity and a success rate of only 30%, and many patients return to their presurgical limb girth within three to four years. Nonsurgical treatment of chronic lymphedema can decrease overall lymphatic edema. Sequential gradient compression systems, which compensate for impaired lymphatic flow, return protein-rich lymphatic fluid from the extracellular regions of the tissues back into the circulatory system where the fluid can be excreted. Introduction Lymphedema occurs when an interruption in the lymphatic flow results in the accumulation of protein-rich fluid in soft tissues. While lymphedema occurs most frequently in the extremities, it also can be found in the head, neck, abdomen, lungs, and around the genitalia. When the lymphatic system is damaged or blocked, edema accumulates over a period of time and thickens the interstitial tissue with fibrosis. Primary lymphedema, which is associated with developmental abnormalities of the lymphatic system, may be manifested in neonates (congenital), in adolescents (praecox), or in patients over the age of 35 years (tarda). Secondary lymphedema, an acquired loss of lymphatic patency, is the more common form of lymphedema that occurs following infections or in patients with cancer. Secondary lymphedema occurs when the lymphatics are damaged by metastatic disease or when the lymphatic basins at risk are surgically removed and/or radiated in a prophylactic or therapeutic manner.[1] Following the onset of secondary lymphedema, the accumulation of lymphatic fluid in the subcutaneous tissue spaces and skin leads to a cosmetically displeasing enlargement of the extremity and overall limb heaviness and fullness that can limit activities of daily life. Recurrent infection in the extremity can lead to the deterioration of the lymphedematous limb over time. Recent reviews[2,3] of the intergroup study of elective lymph node dissections for melanoma show that surgical removal of the regional lymph node basins at risk induces postoperative leg lymphedema in 21.4% of patients. The incidence for arm lymphedema is 3%. ---------------------------------------------------------Table 1. Interventions to Avoid in Patients With Lymphedema Venipuncture Injections Intravenous contrast injections Acupuncture Liposuction Blood pressure tests ---------------------------------------------------------Pathophysiology The lymphatic system develops embryologically as part of the vascular system. Lymphatic fluid comprises endothelial cells, protein, water, tissue products, and foreign particles. The lymphatic system circulates interstitial proteins and lipids back into the vascular system through lymphatic capillaries. The capillaries are valveless intradermal vessels that drain into unidirectional-valved lymphatic vessels located at the junction between the dermis and the subcutaneous tissue. These unidirectional vessels then drain into afferent lymphatics. The lymph is propelled by muscular movement and contraction of the larger lymphatic vessels, and the flow is controlled by valves located at 1- to 2cm intervals. The lymphatic fluid is subsequently filtered by regional lymph nodes that eventually empty into larger vessels in the venous system, primarily at the thoracic duct. Unlike the blood circulatory system, the lymphatic system is a regional drainage system. However, lymph vessels communicate between various regions.[4] Diagnosis, Assessment Methods, and Symptoms Diagnosis of lymphedema of the arm or leg is established on the basis of an accurate history and a thorough physical examination. Assessment of the progression of edema in the postoperative care of the patient can be accomplished with photography, circumferential measurements, and water displacement measurements. Each method has inherent shortcomings, but a patient's progression or response to therapy is monitored well when these are used together. Photography[5] at preoperative and postoperative visits can be useful in determining the onset and progression of lymphedema. Photographs must be taken not only from the same focal distance, but also at the same time of day since the extent of lymphedema is dependent on time and activity. Photographs taken in the morning generally show less edema. Afternoon photographs give a more accurate assessment of the patient's status and level of disability. Circumferential measurements using reference points to bony landmarks also are valuable in following a patient's response to therapy or the progression of lymphedema. Relatively small increases in the diameter of the leg can reflect a large increase in the overall volume and weight of the limb. In severe cases when most bony landmarks are obscured, the inferior border of medial malleolus and the superior border of the patella in the leg generally can be identified; in the arm, the ulnar styloid and the tip of the olecranon are the best landmarks. A third method of assessment, called water displacement[5] or volumetric study, measures the volume of displaced fluid after the affected limb is placed in a tank of water. Although this is the most accurate method of documenting changes in edema, it is time consuming, and its use is limited to facilities with the required equipment. Common complaints of chronic lymphedema include a sense of increase in size or fullness in the extremity, a corresponding heaviness, and a decrease in the functional ability of the limb. Patients with chronic disease may experience decreases in range of motion and function (usually in the arm) secondary to interstitial fibrosis. Pain and achiness also may occur. Lymphangiosarcoma, a rare sequela after mastectomy of long-term lymphedema, may be suspected if a local tumor or purple or bluish discolorations become apparent.[6] Management Prophylaxis Initial interventions for lymphedema are aimed at prevention. Some therapeutic interventions may aggravate lymphedema and may compromise a patient's response to treatment (Table 1). To avoid trauma and infection of the affected limb, any injections, blood pressure measurements, and administration of intravenous medications should be applied to an unaffected limb. Surgical Treatment During the last century, a number of surgical treatment plans have been used to attempt to reconstruct the lymphatic channels.[7] These treatments ranged from burying silk and other synthetic materials in the soft tissues to mimic lymphatic channels to the more recent practices of removing the subcutaneous fat and placing a dermal flap within the muscle to encourage superficial to deep lymphatic anastomoses.[8] A retrospective review[8,9] of the available surgical techniques shows that 30% of patients undergoing a surgical repair had good sustained results. The overall success rate was low, and many of the patients regressed to their pretreatment girth measurements within three to four years following the original reduction surgery. Two categories of patients might today be considered for surgical treatment. Patients who have massive lymphedema with overlying skin breakdown are candidates for the Charles procedure. Skin and subcutaneous tissue is removed to the level of the underlying fascia, and the extremity is covered with split thickness skin grafts. Although the cosmetic appearance of the limb is not favorable, this procedure can allow a patient who may have been immobile to return to a normal activity routine. Moderate length hospitalization is required and wound-healing problems can occur in the skin-grafted areas, but the risk-benefit evaluation is favorable since these patients are homebound and/or bedridden if untreated. The second category of patients for surgical treatment consists of those who have demonstrated no further progress from optimal conservative therapy, yet remain with significant extremity enlargement but with good skin cover. This group may benefit from excision of skin and subcutaneous tissue in a staged approach. The inner aspect of the extremity is addressed first. In a second stage, an excision is carried out on the lateral aspect This technique can be performed with a low morbidity and short hospitalization. To maintain the improvement that is obtained surgically, long-term compression garments are necessary, as well as all aspects of optimal care of the affected extremity. However, neither surgery nor conservative therapy will produce long-term results without lifelong diligent care. ---------------------------------------------------------Table 2. Care Guidelines for the Patient With Lymphedema Keep skin clean and moisturized Elevate limb while sleeping and traveling Wash with hypoallergenic soaps and cleaners Use electric razors (rather than straight razors) to remove hair Use mild detergents for clothes Maintain a constant temperature in the home Eat a balanced, nutritious diet Treat infections early and thoroughly with antibiotics Exercise (walking, swimming, prescribed isometrics) Wear prescribed garments and or bandages Avoid cuts, burns, and insect bites Avoid sunburns Wear loose-fitting clothing Avoid heavy, traumatic, or repetitive exercises Avoid lifting heavy objects ---------------------------------------------------------Nonsurgical Treatment Most patients with chronic secondary lymphedema are best managed by nonsurgical measures. Patient education on activity levels and infection prophylaxis are important factors in long-term control. Physical therapy[10] and compression garments or sequential gradient compression-type pumps are recent additions to the therapeutic armamentarium. Since the accumulation of protein-rich fluid creates a culture that encourages bacterial growth, infection prophylaxis is important for those patients with chronic lymphedema who are prone to repeated infections. Patient education relating to skin care (eg, avoidance of injury, care of open wounds, and proper nail care) is necessary. The risk of cellulitis and infection to the arm or leg correlates with the severity of the lymphedema, and each subsequent episode of infection increases the risk of bacteremia and systemic toxicity, thereby exacerbating the lymphedematous condition. Patients are instructed on early identification of infection. The use of antibiotics at the first sign of infection may prevent a serious cellulitis. Not all forms of exercise are beneficial to patients with extremity lymphedema, but those that increase circulation by incorporating use of the affected limb are recommended (eg, swimming, biking, walking, isometric exercises, and active range of motion exercises). Activities that involve heavy lifting or repetitive motion cause pooling of the fluids are avoided. Patients with leg lymphedema should avoid high-impact aerobics and jogging, while those with lymphedema of the dominant arm should avoid sports such as tennis and racquetball. Use of a compression garment during exercise will help to decrease pooling of fluids. The overall treatment plan, individualized based on the patient's specific needs and deficits, generally includes instruction by a physical therapist on exercises to regain or maintain normal range of motion and strength, as well as education regarding limb elevation, skin care precautions, massage techniques, pumping (isometric) exercises, and soft-tissue mobility. A physical therapist not only can provide education on the mechanism of lymphedema, signs and symptoms, physical therapy goals, and treatment options, but also can train the patient to use compression garments and to monitor sequential gradient compression-type pumps (Table 2).[4,11] Due to communications of the lymphatic vessels between various body regions, physical therapy can aid chronic lymphedema by shunting fluid out of the compromised limb. The physical therapy, which can be performed in a hospital or at home, is offered in two phases. The first phase, which spans a period of four weeks, is divided into four segments. The first focuses on improving and maintaining the normal skin integrity while decreasing the risks of infection. The second involves manual lymphatic drainage, a daily treatment that is designed to remove excess lymphatic fluid and to open collateral lymphatics, thereby allowing unaffected regions to aid the compromised regions in draining excess lymphatic fluid. The third consists of compression bandaging to maintain and increase compartment pressure and to prevent retrograde flow of lymphatic fluid, and the fourth entails specialized physical therapy exercises followed by lymphatic massage. The trunk is massaged first to empty the lymphatics, followed by the areas adjacent to the compromised extremity, the central portions of the limb, and finally the distal portion of the arm or leg. In theory, this massage therapy forces the excess lymphatic fluids into watershed regions of the body and provides access to the unaffected lymphatic collateral circulation. The second phase of physical therapy consists of fitting the patient with specially measured compression garments. Evaluation has shown that application of the techniques in these two phases can reduce the size of the affected limb by up to 65%.[10] In addition to the expertise of skilled personnel, a commitment by the patient to complete the time-consuming program is required in order to realize the benefits of therapy and to maintain the achieved improvements. Fig 1. Multicom 500 five-chamber peristaltic gradient sequensial pressures. Shown are maximum presures per chamber during peristaltic cycle with adjustment at 80 mmHg. Drug Therapy -Few drugs for the treatment of chronic lymphedema are currently being studied.[5,12] Venalot is a benzopyrene that breaks down the larger protein molecules and may facilitate absorption of proteins into the vascular system at the level of the capillaries. This drug currently is not available in the United States. Diuretics give minimal benefit in the treatment of chronic lymphedema secondary to oncologic surgery or metastatic spread of the disease, and their beneficial effects are temporary. The use of these drugs should be reserved for early treatment of primary lymphedema. Compression Devices - Compression pumps are being used more often in the medical management of chronic lymphedema.[13-17] While clinical massage can be effective, constraints created by the need for experienced personnel and the time needed to perform the technique limit the availability of this treatment on a regular basis. Researchers have focused on duplicating the beneficial effects of massage by developing mechanical and/or air compression devices.[14,17-19] The older intermittent, single-chamber, nonsegmental compression pumps provide even pressure throughout the treated extremity. These do not provide a direction for the transfer of fluid, thereby allowing some backflow of the lymphatic fluid. This retrograde flow, therefore, may cause increase lymphatic fluid in the proximal tissues of the limb. Newer devices provide sequential compression. Such machines force compressed air into a sleeve that fits over the affected limb. There are standard and gradient sequential systems. The standard sequential compression system without calibrated gradient pressure is a multichamber pump that delivers the compression at the same pressure in each garment section from distal to proximal tissues.[17] The peristaltic sequential gradient compression system more closely mimics normal extremity pressure changes. The pressures delivered by the sequential gradient system differ by approximately 10 mmHg between each chamber. The higher pressures are delivered to the distal chamber, with each chamber having approximately 10 mmHg less pressure than the preceding chamber (Fig 1). For increased efficiency, the delivery of lymphedema therapy must be not only physiologically compatible with the lymph system, but also powerful enough to imitate the rhythmic motion of the skeletal muscles in order to transfer the excess lymphatic fluid in a distal-to-proximal fashion. This system provides the best results when the patient is recumbent (for treatment of a leg) or when the limb is elevated (for treatment of an arm), since these positions minimize the effects of gravity on venous flow. Initial studies[13] with compression pumps employed a series of overlapping cell compartments that applied a sequential pattern of compression to the affected limb. This recreated the physiologic "milking" action of the lymphatics within the extremity. The pressures used in this pump ranged to 110 mmHg in the arms and to 150 mmHg in the legs. A controlled site trial[18] of this type of pump followed 24 patients for six months following treatment and demonstrated that even after one treatment with the device, approximately half of the patients maintained most of their reduction over several months. The best results were seen in a patient who had access to a pump and used it on an intermittent basis (three times per week) over the follow-up period of six months. An overall reduction in girth and heaviness was seen in each limb without cutaneous, neurologic, or muscular complications. Success requires treatment for a minimum of one hour each session, and lower pressures for longer periods of time are more effective than higher pressures for shorter periods of time. Patients are instructed to wear their fitted compression garments and to elevate the limb whenever possible. Fig 2. Sequential compression systems consist of an air compression pump, sequential pneumatic garments, and air hoses that connect the pump to the individual compartments of the garment. This therapy can be self- administered at home. The most advanced sequential compression systems consist of air compression pumps, sequential pneumatic garments, and air hoses that connect the pump to individual compartments of the garment. The system provides continuous pneumatic compression to gently massage the arm or leg. Once connected, the garment will inflate peristaltically up the limb: the first chamber inflates and holds, followed by the second chamber, and when the third chamber inflates, the first one deflates. This sequential compression continues up the limb to provide maximum therapeutic pressures while relieving unnecessary pressure on tissues behind the wave of compression. This therapy can be self-administered at home (Fig 2). Contraindications to the use of gradient sequential compression devices include massive edema of the extremity secondary to congestive heart failure, concurrent neurologic symptoms, ischemic vessel disease or severe arteriosclerosis, deformity of the limb, metastatic disease in the involved extremity, and skin changes (eg, dermatitis, gangrene, recent skin grafts, and especially cellulitis and deep-vein thrombosis).[5] Conclusions The oncologist often is faced with the problematic management of chronic lymphedema of the arm or leg. Until recent years, this condition had been neglected due to poor understanding of the causative and abnormal physiology behind the condition. Consequently, most patients were either undertreated or completely untreated. This resulted in a lifelong struggle for many patients that eventually led to crippling and disabling consequences. In the past, patients were told that this condition was something they had to live with. Knowledge of the physiology and pathophysiology of lymphedema is helpful to understand the rationale of available prophylactic and therapeutic approaches. The degree of edema is established prior to initiating short- or long-term care. Surgical intervention is useful for some patients, but the current standard of care is conservative medical management aimed at minimizing existing edema while controlling the formation of new edema. Patient education includes instruction in exercises, elevation of the arm or leg, and infection prophylaxis, as well as activities to avoid.[20] Physicians, nurses, physical therapists, and occupational therapists all have active roles in the care of chronic lymphedema. External compression therapy using peristaltic sequential gradient compression devices assist control. This treatment can be given intermittently at home. A realistic approach to long-term care, coupled with therapeutic and emotional support, can maximize the quality of life of patients with chronic lymphedema. References 1. Fitts WT, Keunelian, JG, Ravdin IS, et al. Swelling of the arm after radical mastectomy. Surgery. 1954;35:460. 2. Smith TJ, Balch C, Bartolucci A. et al. H. Lee Moffitt Cancer Center, Tampa, Fla. Risks and complications of elective inguinal node dissection. Abstract: SSO, 1995. 3. Smith T, Balch C, Bartolucci A, et al. Current results of the Intergroup Surgical Trial in intermediate thickness melanoma. In: Program and abstracts of the 38th Annual Clinical Congress: Advances in the Biology and Clinical Management of Melanoma; February 21-24, 1995; Houston, Tex. Abstract: 9-10. 4. Vasudevan SV, Melvin JL. Upper extremity edema control. Am J Occup Ther. 1979;33:520-523. 5. Miller TA, Das SK. Classification and treatment of lymphedema. In: Rutherford R, ed. Vascular Surgery. 4th ed. Philadelphia, Pa: WB Saunders Co; 1995:232-240. 6. Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema. Cancer. 1948;1:64-81. 7. Handley WS. Lymphangioplasty: a new method for the relief of the brawny arm of breast cancer and for similar conditions of lymphatic edema: preliminary note. Lancet. 1:1783, 1908. 8. Chilvers AS, Kinmonth JB. Operations for lymphedema for the lower limbs: a study of the results in 108 operations utilizing vascularized dermal flaps. J Cardiovasc Surg (Torino). 1975;16;115-119. 9. Kinmonth JB, Patrick JH, Chilvers AS. Comments on operations for lower limb lymphoedema. Lymphology. 1975:8:56-61. 10. Zeissler RH, Rose GB, Nelson PA. Postmastectomy lymphedema: late results of treatment in 385 patients. Arch Phys Med Rehabil. 1972;53:159-166. 11. Stillwell GK. Psychiatric management of postmastectomy lymphedema. Med Clin North Am. 1962;46:1051-1063. 12. Piller NB. Conservative treatment of acute and chronic lymphoedema with benzo-pyrones. Lymphology. 1976;9:132-137. 13. Zelikovski A, Manoach M, Giler S, et al. Lympha-Press, a new pneumatic device for the treatment of lymphedema of the limbs. Lymphology. 1980;13:68-73. 14. Zelikovski A, Melamed I, Kott M, et al. The "Lympha-Press": a new pneumatic device for the treatment of lymphedema: clinical trials and results. Folia Angiologia. 1980;28:165-169. 15. McLeod A, Brooks D, Hale J, et al. A clinical report on the use of three external pneumatic compression devices in the management of lymphedema in a pediatric population. Physiother Cancer. 1991;43:28-31. 16. Bastien MR, Goldstein BG, Lesher JL Jr, et al. Treatment of lymphedema with a multicompartmental pneumatic compression device. J Am Acad Dermatol. 1989;20:853854. 17. Raines JK, O'Donnell TF Jr, Kalisher L, et al. Selection of patients with lymphedema for compression therapy. Am J Surg. 1977;133:430-437. 18. Richmond DM, O'Donnell TF Jr, Zelikovski A. Sequential pneumatic compression for lymphedema: a controlled trial. Arch Surg. 1985;120:1116-1119. 19. Pappas CJ, O'Donnell TF Jr. Long-term results of compression treatment for lymphedema. J Vasc Surg. 1992;16:555-562. 20. O'Donnell TF Jr. The management of primary lymphedema. In: Ernst CB, Stanley CJ, eds. Current Therapy in Vascular Surgery. 2nd ed. Philadelphia, Pa: BC Decker; 1991:1022-1029.