Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
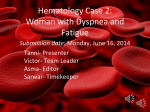
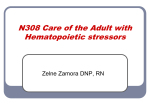
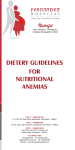
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:269 –277 Ferric Carboxymaltose Prevents Recurrence of Anemia in Patients With Inflammatory Bowel Disease RAYKO EVSTATIEV,* OLGA ALEXEEVA,‡ BERND BOKEMEYER,§ IVAN CHOPEY,储 MARCEL FELDER,¶ MAJA GUDEHUS,¶ TARIQ IQBAL,# IGOR KHALIF,** PHILIPPE MARTEAU,‡‡ JÜRGEN STEIN,§§ CHRISTOPH GASCHE,* and the FERGI Study Group *Department of Medicine 3, Division of Gastroenterology and Hepatology and Christian Doppler Laboratory for Molecular Cancer Chemoprevention, Medical University of Vienna, Vienna, Austria; ‡Regional Clinical Hospital, Nizhni Novgorod, Russian Federation; §Gastroenterology Practice, Minden, Germany; 储National University, Uzhgorod, Ukraine; ¶Vifor Pharma, Glattbrugg, Switzerland; #University Hospital, Birmingham, United Kingdom; **State Scientific Center of Coloproctology, Moscow, Russian Federation; ‡‡Hôpital Lariboisiere, Paris, France; and §§Department of Gastroenterology and Clinical Nutrition, Frankfurt/Main, Germany BACKGROUND & AIMS: Iron-deficiency anemia is the most common systemic complication of inflammatory bowel diseases (IBD). Iron-deficiency anemia recurs frequently and rapidly after iron-replacement therapy in patients with IBD. We performed a randomized, placebo-controlled trial to determine if administration of ferric carboxymaltose (FCM) prevents anemia in patients with IBD and low levels of serum ferritin. METHODS: We performed a single-blind, multicenter study of nonanemic patients who had completed the FERGIcor study. Serum levels of ferritin were assessed every second month, and patients were given FCM (total iron dose, 1181 ⴞ 662 mg; n ⴝ 105) or placebo (n ⴝ 99) when levels decreased to less than 100 g/L. The primary end point was time to recurrence of anemia within 8 months. Secondary end points included changes of quality of life, disease activity, results from laboratory tests, and adverse events. RESULTS: Anemia recurred in 26.7% of subjects given FCM and in 39.4% given placebo. The time to anemia recurrence was longer in the FCM group (hazard ratio, 0.62; 95% confidence interval, 0.38 –1.00; P ⴝ .049). Markers of body levels of iron increased or remained at normal levels in subjects given FCM (ferritin increased by 30.3 g/L, transferrin saturation increased by 0.6%) but decreased in the group given placebo (ferritin decreased by 36.1 g/L, transferrin saturation decreased by 4.0%). Changes in quality of life and disease activity were comparable between groups. Adverse events were reported in 59.0% of the FCM group and 50.5% of the placebo group, and serious adverse events were reported in 6.7% and 8.1%, respectively. CONCLUSIONS: FCM prevents recurrence of anemia in patients with IBD, compared with placebo. Nevertheless, the high rate of anemia recurrence warrants optimization of the frequency and requirements for FCM treatment. Clinical Trial number: NCT00810004. Keywords: Intravenous Iron; Crohn’s Disease; Ulcerative Colitis; Iron Maintenance Treatment. I ron deficiency is one of the world’s most common and potentially treatable health problems.1 Even in developed countries, patients suffering from conditions associated with chronic blood loss and/or chronic inflammation are at risk of developing irondeficiency anemia,2,3 a leading cause of hospitalization and morbidities such as fatigue in inflammatory bowel disease (IBD).2,4 –7 Iron deficiency can result from chronic blood loss, decreased dietary intake, reduced intestinal absorption, or impaired use of endogenous iron owing to chronic inflammation.8 Anemia and iron deficiency affect quality of life (QoL), physical performance, and cardiac function.9 –13 Improvement of hemoglobin (Hb) levels, serum ferritin, and transferrin saturation (TSAT) improved QoL independent of changes in disease activity in IBD.14 –16 Intravenous iron preparations such as iron sucrose and ferric carboxymaltose (FCM) have proven their efficacy in the correction of IBD-associated anemia.2,7 Intravenous iron is more ef- fective, better tolerated, and improves the QoL to a greater extent than oral iron.17 Therefore, international and national guidelines recommend intravenous iron replacement for the management of IBD-associated anemia.17,18 However, anemia recurs frequently and quickly after successful intravenous iron therapy.19 An analysis of 88 patients from 3 prospective clinical Abbreviations used in this paper: AE, adverse events; CI, confidence interval; FAS, full analysis set; FCM, ferric carboxymaltose; Hb, hemoglobin; IBD, inflammatory bowel disease; IBDQ, inflammatory bowel disease questionnaire; PPS, per-protocol set; QoL, quality of life; SF36, health survey short form; TEAE, treatment emergent adverse event; TSAT, transferrin saturation; UC, ulcerative colitis. © 2013 by the AGA Institute 1542-3565/$36.00 http://dx.doi.org/10.1016/j.cgh.2012.10.013 270 EVSTATIEV ET AL trials showed that anemia recurred in more than half of the patients within 12 months.19 The presented study, which was entitled Ferinject in gastrointestinal maintenance (FERGImain), evaluated whether FCM can prevent anemia in patients who had been treated previously for IBD-associated anemia. Methods Study Design and Patients FERGImain (ClinicalTrials.gov NCT00810004) was a randomized, placebo-controlled, multicenter, single-blinded trial testing the efficacy of iron treatment with intravenous FCM in preventing anemia recurrence in IBD patients who were nonanemic at the end of the FERGIcor study.14 The study was conducted from February 2009 to October 2010 at 69 hospitals and clinics in 13 countries in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines and after approval of the protocol and its amendments by the respective Ethics Committees and Competent Authorities. Eligible patients were older than age 18 years, nonanemic (Hb ⱖ12 g/dL in women or ⱖ13 g/dL in men), had completed the FERGIcor study,14 had normal levels of vitamin B12 and folic acid, and provided informed consent. Baseline serum ferritin levels or TSAT were not relevant for inclusion into the study. Women of child-bearing potential had to have a negative urine pregnancy test at screening and use an acceptable method of birth control during the study until 1 month after the last dose of the study drug. Patients with a history of erythropoietin treatment, oral iron, or blood transfusions within 12 weeks before screening were excluded. Further exclusion criteria comprised chronic alcohol abuse, chronic liver disease, increase of transaminase levels more than 3 times above the upper limit of normal, portal hypertension with esophageal varices, known hypersensitivity to the study drug, history of acquired iron overload, myelodysplastic syndrome, pregnancy, lactation, known active infection, clinically significant overt bleeding, active malignancy, chronic renal failure, surgery with relevant blood loss (Hb decrease ⬎2 g/dL) within 3 months before screening or planned surgery within the following 3 months, known infection with human immunodeficiency virus, hepatitis B or C, significant cardiovascular disease, and body weight less than 35 kg. Randomization and Treatment Subjects were randomized 1:1 to receive FCM (500 mg iron in a maximum of 250 mL 0.9% saline solution; Ferinject, Vifor Pharma, Glattbrugg, Switzerland) or the same volume of placebo (0.9% saline solution) over 15 minutes. Randomization was performed according to a predefined, computer-generated list as provided via sequentially numbered randomization envelopes (Data Management, Parexel International GmbH, Berlin, Germany). Subjects were stratified according to the treatment group of the preceding FERGIcor study (FCM or iron sucrose) and were blinded to the study drug by using dark nontransparent bags and infusion lines. Investigators and study nurses were aware of the treatment allocation. Treatment Schedule The last study visit of the preceding FERGIcor study served as the screening visit of this study and was followed by the baseline visit within 2 to 7 days. Follow-up visits were CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 3 performed bimonthly until recurrence of anemia or the end of the study at month 8 was reached. At each visit blood tests were performed and disease activity indexes were recorded, which were calculated without consideration of Hb or hematocrit levels. QoL was assessed using the health survey short form (SF-36) questionnaire version 2 and inflammatory bowel disease questionnaire (IBDQ) at baseline, month 2, and month 8. The subjects received the study drug (500 mg iron or placebo) at baseline, month 2, month 4, month 6, or month 8 if serum ferritin had decreased to less than 100 g/L at the respective study visit. Study drug administration was performed via an intravenous drip infusion. Outcome Measures The primary end point was the time to recurrence of anemia as defined by World Health Organization criteria (Hb level ⬍12 g/dL in women or ⬍13 g/dL in men). Because recurrence rates did not exceed 50%, the usual definition for median time to recurrence, probabilities of developing anemia (based on Greenwood’s formula for the standard error of the Kaplan– Meier estimate) were calculated. Secondary efficacy end points included the proportion of patients without anemia at months 2, 4, 6, and 8; changes in health-related QoL (SF-36 version 220 and IBDQ score21) from baseline to month 8; change in disease activity (Crohn’s Disease Activity Index, Colitis Activity Index, C-reactive protein); and days out of work as a result of IBD or anemia. Disease activity indexes were calculated without consideration of Hb or hematocrit. Follow-up and Safety Evaluation Subjects who presented with anemia at a specific study visit were considered to have reached the end point. Safety end points included the nature and frequency of adverse events (AEs) and changes in laboratory parameters. AEs and concomitant medication were recorded continuously. An AE was considered treatment-emergent (TEAE) if it occurred after the first study drug administration. The relationship to treatment was rated as certain, probable, possible, unlikely, or not related. The intensity was rated as mild, moderate, or severe. Safety stopping rules for premature discontinuation were Hb level less than 7 g/dL, Hb level greater than 18 g/dL (in men) or greater than 16 g/dL (in women), serum ferritin level greater than 800 g/L, TSAT greater than 50%, and liver transaminase levels 3 times more than the upper limit of normal. Statistical Analysis The sample size was a consequence of the preceding FERGIcor study, assuming that approximately 50% of patients from this study would enroll into FERGImain. Kaplan–Meier survival curves for time to recurrence of anemia (primary end point) were compared between groups by log-rank test, providing an estimate of the treatment hazard ratio and the corresponding 95% confidence interval (CI). Continuous secondary efficacy end points were analyzed by descriptive statistics comprising mean and standard deviation and with analysis of covariance models. Categoric end points were analyzed by logistic regression. Missing data were treated as missing and only observed cases were used for analysis. Data were analyzed from the safety set, full analysis set (FAS), and per-protocol set (PPS). The safety set comprises all randomized patients with a baseline and at least one postbaseline visit. Patients of the safety set who March 2013 INTRAVENOUS IRON FOR PREVENTION OF ANEMIA 271 Figure 1. Patient flow and disposition. received at least one dose of study drug comprised the FAS. Patients who did not receive any treatment (serum ferritin level remaining ⬎100 g/L throughout the study period) were analyzed separately. The PPS comprised patients without major protocol deviations. Data are presented as percentages of the analyzed population, mean (standard deviation), or median (interquartile range Q1, Q3) unless otherwise indicated. The authors had full access to the study data, statistical analysis, and reviewed and approved the final manuscript. Results Patient and Treatment Characteristics Of 262 screened patients, 256 were randomized to FCM or placebo (Figure 1). A total of 245 patients had at least one postbaseline visit, 105 received FCM, and 99 received placebo (FAS). A total of 41 patients (22 randomized to FCM, 19 randomized to placebo) received no treatment during the study because the serum ferritin trigger of less than 100 g/L had not Table 1. Patient Demographics and Disease Characteristics (Safety Set) Demographics Median age, y (range) Female, n (%) Disease history and status CD, n (%) Median duration of CD, mo (range) Mean CDAI (SD) in CD patients UC, n (%) Median duration of UC, mo (range) Mean CAI (SD) in UC patients Mean Hb, g/dL (SD) Mean ferritin, g/L (SD) Mean TSAT, % (SD) Mean CRP, mg/L (SD) Prior and concomitant medication (in ⱖ5% patients) Aminosalicylates, n (%) Systemic corticosteroids, n (%) Thiopurines, n (%) Anti-TNFs, n (%) FCM (n ⫽ 105) Placebo (n ⫽ 99) 39.0 (18–73) 62 (59.0) 37.0 (20–78) 58 (58.6) 35 (33.3) 74.1 (5.4–413.8) 77.1 (73.3) 70 (66.7) 41.5 (3.7–301.6) 2.5 (2.2) 13.7 (1.0) 76.1 (65.0) 21.8 (11.4) 7.6 (10.0) 25 (25.3) 58.8 (9.4–280.6) 65.4 (45.9) 74 (74.7) 45.3 (3.4–411.1) 2.1 (2.2) 13.6 (0.9) 74.0 (57.9) 23.4 (9.6) 6.3 (8.6) 45 (42.9) 6 (5.7) 12 (11.4) 9 (8.6) 38 (38.4) 3 (3.0) 12 (12.1) 8 (8.1) No treatment (n ⫽ 41) 44.0 (18–74) 27 (65.9) 16 (39.0) 61.5 (3.4–278.7) 84.3 (68.3) 25 (61.0) 64.8 (3.6–324.8) 1.9 (1.6) 13.3 (1.0) 221.0 (106.8) 32.1 (13.7) 7.8 (11.0) 15 (36.6) 2 (4.9) 13 (31.7) 4 (9.8) Total (n ⫽ 245) 39.0 (18–78) 147 (60.0) 76 (31.0) 67.4 (3.4–413.8) 74.9 (64.3) 169 (69.0) 46.5 (3.4–411.1) 2.2 (2.2) 13.6 (1.0) 99.5 (89.4) 24.1 (11.6) 7.1 (9.6) 98 (40.0) 11 (4.5) 37 (15.1) 21 (8.6) P valuea .155c .719d .218d .996c .655e .218d .771c .423e .174e ⬍.001b,e ⬍.001b,e .575e .753d .651d .003b,d .910d CAI, Colitis Activity Index; CDAI, Crohn’s Disease Activity Index; CRP, C-reactive protein; SD, standard deviation; TNF, tumor necrosis factor. aP values for statistical tests over all groups (FCM, placebo, no treatment). bStatistical difference only between the treatment (FCM and placebo) and no treatment groups. cKruskal–Wallis test. dFisher exact test. eStudent t test. 272 EVSTATIEV ET AL been met. The PPS comprised 170 patients: 85 FCM-treated and 85 placebo-treated patients. Patient demographics, medical and surgical history, as well as prior and concomitant medication were not significantly different between FCM- and placebotreated patients (Table 1). Differences for serum ferritin, TSAT, and concomitant treatment with thiopurines were owing to higher counts in the no-treatment group. In the preceding FERGIcor study, 138 (53.9%) patients had received FCM and 118 (46.1%) patients had received iron sucrose. In FERGImain, a smaller proportion of FCM- than placebotreated patients required iron infusions at all visits after baseline. FCM-treated patients received a median of 2 infusions (range, 1–5 infusions), corresponding to 1000 mg iron (range, 500 –2500 mg iron); placebo-treated patients received 3 saline infusions (range, 1–5 infusions). The median time to first infusion was 5 days (range, 0 –246 days) for FCM and 4 days (range, 4 –246 days) for placebo, respectively. Recurrence of Anemia (Primary End Point) Kaplan–Meier analysis of the probability of becoming anemic showed significantly lower rates in FCM-treated patients compared with the placebo-treated patients of the FAS (27.2% vs 40.4%; hazard ratio, 0.62; 95% CI, 0.38 –1.00; Kaplan– Meier analysis; P ⫽ .049, log-rank test) (Figure 2). The calculated time to development of anemia in 25% of patients was 7.6 months (FCM) vs 4.7 months (placebo). The cumulative Kaplan–Meier probabilities of developing anemia at months 2, 4, 6, and 8 were 10.5%, 16.2%, 21.0%, and 27.2% in the FCM group, and 15.2%, 23.3%, 32.8%, and 40.4% in the placebo group. The actual number of patients who developed anemia during the study period was 28 (27.5%) and 39 (41.5%) among FCM- and CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 3 placebo-treated patients who completed the 8-month period or became anemic during this period (2 test: P ⫽ .038). Patients who did not receive treatment during the study (because their serum ferritin level was always greater than 100 g/L) were not included in the FAS. In this no-treatment group, anemia had recurred in 14 (35%) patients by month 8 (1 patient withdrew without postbaseline Hb assessments). In the PPS, the estimated hazard ratio for anemia recurrence was similar to the one calculated for the FAS (hazard ratio, 0.65; 95% CI, 0.38 – 1.09). Secondary End Points Serum ferritin level improved and TSAT remained within the normal range in FCM-treated (⫹30.3 g/L and ⫹0.58%) but not in placebo-treated patients (⫺36.1 g/L and ⫺4.00%) over the 8-month study period (P ⬍ .001 and P ⫽ .022; Figure 3A and B). In this nonanemic patient population, QoL scores (SF-36 physical component and IBDQ) showed a positive mean change from baseline to month 8 in the FCM group (SF-36, 0.3 ⫾ 0.7; IBDQ, 1.7 ⫾ 3.1), but a decrease in the placebo group (SF-36, ⫺0.6 ⫾ 0.8; IBDQ, ⫺1.1 ⫾ 3.7); however, differences between the study groups were not significant (P ⫽ .4 and P ⫽ .5, respectively). In addition, changes in clinical disease activity and C-reactive protein levels from baseline to the end of the study period were not different between FCM and placebo (Crohn’s Disease Activity Index, ⫺3.8 ⫾ 46.6 and 13.3 ⫾ 60.4; P ⫽ .171; Colitis Activity Index, ⫺0.1 ⫾ 2.2 and 0.1 ⫾ 2.1; P ⫽ .319; C-reactive protein, ⫺1.0 ⫾ 9.5 mg/L and 1.2 ⫾ 7.0 mg/L, P ⫽ .456). In addition, a trend was observed toward fewer FCM- than placebo-treated patients who had lost 1 or more working days because of IBD (6.7% vs 11.1%; P ⫽ .25). The median percentage of days out of work because of IBD was comparable between FCM and placebo (7.95 [Q1, Q3; 5.06, 19.18] vs 6.41 [Q1, Q3; 1.26, 15.06]). Tolerability TEAEs were reported for 59.0% (FCM) and 50.5% (placebo) of patients and serious AEs for 6.7% and 8.1% (FCM vs placebo; Table 2). The most common TEAEs were ulcerative colitis (UC)–specific symptoms and nasopharyngitis (7.8% and 7.3%, respectively). Interestingly, gastrointestinal symptoms and flares of UC were somewhat less frequent with FCM compared with placebo (20.0% vs 28.3% [P ⫽ .17] and 6.7% vs 12.1% [P ⫽ .18], respectively). No infusion site reaction was reported and no death occurred. Three FCM-treated patients had TEAEs leading to permanent discontinuation of the study drug. All events were of moderate intensity, 2 events (increased alanine aminotransferase level and increased aspartate aminotransferase level) were considered possibly related, and 1 event (pancreatitis) was considered not related to the study drug. There was no treatment-related anaphylactic reaction. Discussion Figure 2. Kaplan–Meier plots of anemia-free survival from baseline to month 8 (FAS patient population) (hazard ratio, 0.62; 95% CI, 0.38 – 1.00; P ⫽ .049). Time to recurrence of anemia in 25% of patients: 7.6 months (FCM), 4.7 months (placebo). Recurrence rate at month 8: 26.7% (FCM), 39.4% (placebo). Iron deficiency is the main cause of anemia in IBD, which responds well to iron-replacement therapy. However, anemia recurs in more than half of iron-treated patients within a year, indicating a need for iron maintenance therapy.2 FERGImain tested intravenous iron maintenance therapy for the prevention of anemia recurrence in this setting. In this study, the serum ferritin concentration was measured every 2 months March 2013 INTRAVENOUS IRON FOR PREVENTION OF ANEMIA 273 Figure 3. Adjusted mean changes and standard error of iron status parameters (A) serum ferritin and (B) TSAT at months 2, 4, 6, and 8. *P ⬍ .05 vs placebo. ⫹Month 8 or early termination. and FCM (or placebo) was administered when serum ferritin level had decreased to less than 100 g/L.17 The results show that FCM infusions (500 mg iron each) can reduce the rate of anemia recurrence in IBD. Because separation of the Kaplan– Meier curves continued to increase until the end of the study period we may anticipate a further benefit from FCM beyond 8 months. Iron status (serum ferritin and TSAT) improved or remained normal over the study period in FCM-treated patients, but worsened in those on placebo. Thus, ferritin-triggered FCM treatment effectively prevented iron deficiency and IBD-associated anemia. FCM was well tolerated without new safety findings. AE and serious AE rates were comparable between FCM and placebo. Importantly, no drug-related anaphylaxis or infusion site reaction occurred in this study. Of note, gastrointestinal symptoms and flares of UC were less frequent in the FCM group. Among patients randomized to placebo, the recurrence of anemia, 39.4% at 8 months, was considerably high. This is in line with a previous retrospective analysis that indicated a 40% recurrence of anemia after 8 months, 50% after 10 months, and 56% after a year.19 Notably, the patient population in FERGImain displayed a rather low clinical disease activity, reflecting the inclusion criteria of the preceding FERGIcor study.14 Accordingly, the results of this study suggest that even IBD patients with apparently quiescent disease and replenished iron stores cannot maintain a positive iron balance and are therefore at a considerable risk of developing anemia. This observation not only should warrant close monitoring of iron and anemia markers, but also is suggestive of subclinical mucosal disease that may need re-evaluation and treatment escalation.17 The great risk of anemia recurrence, however, supports the implementation of preventive measures as successfully shown in this study. In contrast to the traditional watch-and-wait strategy, FERGImain introduces the novel concept of proactive anemia prevention. Considering that anemia in IBD substantially reduces QoL, contributes to fatigue,13 and is a common trigger for hospitalization,5,7 effective anemia prevention may provide a meaningful alleviation of the overall disease burden. Further support for preventive ferritin-triggered iron replacement comes from reports showing that treatment of iron deficiency even without anemia can improve fatigue, exercise performance, and muscle function.10,11,22,23 Although the study was not designed and powered to detect a treatment effect on QoL, a positive trend in terms of improved physical characteristics in favor of FCM treatment was observed. Cost comparisons also favor a proactive approach to anemia management. Waiting for anemia recurrence may be expensive because the average annual health care payments are more than twice as high for anemic compared with nonanemic IBD patients (US$19,113 vs US$7678).24 Therefore, FCM maintenance therapy may be a cost-effective option for anemic IBD patients. Notably, colitis symptoms were reported less frequently in FCM-treated patients and there was a trend toward a lower percentage of patients who lost at least 1 working day as a result of IBD. This confirms the good tolerability profile of FCM and is in line with clinical experience and in vitro experiments that have shown a reduced responsiveness of iron-loaded macrophages to the TH-1 cytokine interferon-␥, leading to lower production of tumor necrosis factor-␣ and other proinflammatory stim- 274 EVSTATIEV ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 3 Table 2. Safety Results n (%) Any TEAE Any severe TEAE Any SAE TEAE leading to discontinuation Death Any related TEAE Any related severe TEAE Any related SAE Related TEAE leading to discontinuation Most common TEAEs (⬎2% of patients in the FCM or placebo group) Worsening of UC Nasopharyngitis Abdominal pain Transaminase increase Worsening of Crohn’s disease CRP increase Headache Viral respiratory tract infection Hematochezia Back pain Nausea FCM (n ⫽ 105) Placebo (n ⫽ 99) No treatment (n ⫽ 41) Total (n ⫽ 245) 62 (56.0) 10 (9.5) 7 (6.7) 3 (2.9) 0 8 (7.6) 0 0 2 (1.9)c 50 (50.5) 4 (4.0) 8 (8.1) 0 0 1 (1.0) 0 0 0 16 (39.0) 0 3 (7.3) 0 0 1 (2.4) 0 0 0 128 (52.2) 14 (5.7) 18 (7.3) 3 (1.2) 0 10 (4.1) 0 0 2 (0.8) .036b — — .652 7 (6.7) 10 (9.5) 7 (6.7) 9 (8.6) 1 (1.0) 5 (4.8) 4 (3.8) 5 (4.8) 1 (1.0) 4 (3.8) 3 (2.9) 12 (12.1) 7 (7.1) 5 (5.1) 3 (3.0) 3 (3.0) 3 (3.0) 2 (2.0) 1 (1.0) 3 (3.0) 0 0 0 1 (2.4) 0 0 4 (9.8) 0 2 (4.9) 0 0 0 0 19 (7.8) 18 (7.3) 12 (4.9) 12 (4.9) 8 (3.3) 8 (3.3) 8 (3.3) 6 (2.4) 4 (1.6) 4 (1.6) 3 (1.2) .050d .375 .277 .061 .029d .397 .641 .180 .399 .132 .216 P valuea .086 .059 .946 .297 CRP, C-reactive protein. aP values for statistical tests over all groups (FCM, placebo, no treatment). bStatistical difference between the FCM and placebo groups (Fisher exact test). cPossibly related increase in liver enzymes. dStatistical difference between the treatment group (FCM and placebo) and the no treatment group. uli.4,8,25,26 These considerations may translate into an individual as well as a communal benefit of FCM in prevention of IBDassociated anemia. Because all patients had been part of a preceding anemia correction trial (FERGIcor14), the study population was well defined and reflects the clinical situation of anemic IBD patients who are treated until resolution of anemia. Although the single-blinded design may be considered a potential shortcoming, the primary end point, a laboratory value, was unlikely to be affected by the study personnel’s awareness of the treatment. A bias on the physician’s judgment of disease activity or of drug-related AEs cannot be excluded; however, a single-blinded design tends to cause an overestimation of drug-related AEs, and disease activity was persistently in remission in both treatment arms. Identification of an appropriate trigger and monitoring frequency for iron replacement in a nonanemic IBD patient population was a challenge when designing this study. The conventional definition of iron deficiency in patients without inflammation is a serum ferritin level less than 30 g/L.27,28 However, because ferritin is an acute-phase protein, serum levels can increase to greater than 30 g/L in patients with chronic inflammation despite empty iron stores, and a ferritin level less than 100 g/L may be more appropriate to define iron deficiency in active IBD.14,16,17,29 Accordingly, anemia recurrence in IBD patients can occur way before a decrease of ferritin level to less than 30 g/L.19 Therefore, a higher ferritin cut-off value was chosen to ensure early recognition of patients at risk of anemia recurrence. Shortcomings of the selected treatment trigger may be the reason that a smaller than expected prolonga- tion of anemia-free survival was seen, indicating a potential to improve the maintenance treatment regimen. In fact, despite the high ferritin cut-off value, a substantial proportion of FCM-treated patients (26.7%) experienced recurrence within 8 months. Also, 14 of 40 patients (35%) with postbaseline Hb assessments who did not receive any treatment became anemic before their serum ferritin levels decreased to less than 100 g/L. This no-treatment group had higher serum ferritin and TSAT levels at baseline (Table 1) and more patients on concomitant thiopurine treatment. It is likely that the observed mild Hb decrease in this no-treatment population is rather a consequence of thiopurines than of iron deficiency itself. In a prior analysis,19 a decrease in TSAT (⬍16%) occurred before anemia recurrence, indicating that TSAT might have been a better treatment trigger. However, concerns about the reliability of TSAT as a diagnostic marker (particularly when blood is drawn in a nonfasting state or hemolysis occurs within the test tube) prompted the recommendation of a serum ferritin level of less than 100 g/L as the treatment trigger instead. Reasons for recurrence in iron-treated patients may be the low FCM dose (500 mg iron compared with the maximum recommended single dose of 1000 mg or 20 mg/kg body weight) and the monitoring interval between ferritin assessments. Considering this 2-month monitoring interval and prior findings on early anemia recurrence,19 triggering treatment at a higher ferritin level might be appropriate. Further subanalyses of the patient populations that benefit most from FCM maintenance treatment may allow for optimization of the treatment schedule and the triggers for treatment. In conclusion, serum ferritin–triggered iron therapy with FCM is an effective and safe March 2013 treatment to prevent recurrence of anemia in patients who have responded to prior intravenous iron-replacement therapy. Optimizations regarding the treatment trigger, FCM dose, and dosing interval, as well as the identification of high-risk groups are warranted. INTRAVENOUS IRON FOR PREVENTION OF ANEMIA 20. 21. References 1. WHO. Worldwide prevalence of anaemia 1993–2005. Geneva, Switzerland: World Health Organization, 2008. 2. Kulnigg S, Gasche C. Systematic review: managing anaemia in Crohn’s disease. Aliment Pharmacol Ther 2006;24:1507–1523. 3. Qunibi WY. The efficacy and safety of current intravenous iron preparations for the management of iron-deficiency anaemia: a review. Arzneimittelforschung 2010;60:399 – 412. 4. Gasche C, Lomer MC, Cavill I, et al. Iron, anaemia, and inflammatory bowel diseases. Gut 2004;53:1190 –1197. 5. Gisbert JP, Gomollón F. Common misconceptions in the diagnosis and management of anemia in inflammatory bowel disease. Am J Gastroenterol 2008;103:1299 –1307. 6. Graff LA, Vincent N, Walker JR, et al. A population-based study of fatigue and sleep difficulties in inflammatory bowel disease. Inflamm Bowel Dis 2011;17:1882–1889. 7. Stein J, Hartmann F, Dignass AU. Diagnosis and management of iron deficiency anemia in patients with IBD. Nat Rev Gastroenterol Hepatol 2010;7:599 – 610. 8. Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med 2005;352:1011–1023. 9. Anker SD, Comin Colet J, Filippatos G, et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med 2009;361:2436 –2448. 10. Brownlie T, Utermohlen V, Hinton PS, et al. Tissue iron deficiency without anemia impairs adaptation in endurance capacity after aerobic training in previously untrained women. Am J Clin Nutr 2004;79:437– 443. 11. Krayenbuehl PA, Battegay E, Breymann C, et al. Intravenous iron for the treatment of fatigue in nonanemic, premenopausal women with low serum ferritin concentration. Blood 2011;118: 3222–3227. 12. Verdon F, Burnand B, Stubi CL, et al. Iron supplementation for unexplained fatigue in non-anaemic women: double blind randomised placebo controlled trial. BMJ 2003;326:1124. 13. Wells CW, Lewis S, Barton JR, et al. Effects of changes in hemoglobin level on quality of life and cognitive function in inflammatory bowel disease patients. Inflamm Bowel Dis 2006;12: 123–130. 14. Evstatiev R, Marteau P, Iqbal T, et al. FERGIcor, a randomized controlled trial on ferric carboxymaltose for iron deficiency anemia in inflammatory bowel disease. Gastroenterology 2011;141: 846 – 853. 15. Gasché C, Dejaco C, Waldhoer T, et al. Intravenous iron and erythropoietin for anemia associated with Crohn disease. A randomized, controlled trial. Ann Intern Med 1997;126:782–787. 16. Kulnigg S, Stoinov S, Simanenkov V, et al. A novel intravenous iron formulation for treatment of anemia in inflammatory bowel disease: the ferric carboxymaltose (FERINJECT) randomized controlled trial. Am J Gastroenterol 2008;103:1182–1192. 17. Gasche C, Berstad A, Befrits R, et al. Guidelines on the diagnosis and management of iron deficiency and anemia in inflammatory bowel diseases. Inflamm Bowel Dis 2007;13:1545–1553. 18. Gasche C, Evstatiev R, Haas T, et al. [Diagnosis and treatment of iron deficiency and anaemia in inflammatory bowel diseases. Consensus of the Austrian IBD Working Party]. Z Gastroenterol 2011;49:627– 632. 19. Kulnigg S, Teischinger L, Dejaco C, et al. Rapid recurrence of IBD-associated anemia and iron deficiency after intravenous iron 22. 23. 24. 25. 26. 27. 28. 29. 275 sucrose and erythropoietin treatment. Am J Gastroenterol 2009;104:1460 –1467. Ware JE, Kosinski M, Dewey JE. How to score version 2 of the SF-36 Health Survey. 3rd ed. Lincoln, RI: QualityMetric, Inc, 2001. Irvine EJ, Feagan B, Rochon J, et al. Quality of life: a valid and reliable measure of therapeutic efficacy in the treatment of inflammatory bowel disease. Canadian Crohn’s Relapse Prevention Trial Study Group. Gastroenterology 1994;106:287–296. Brutsaert TD, Hernandez-Cordero S, Rivera J, et al. Iron supplementation improves progressive fatigue resistance during dynamic knee extensor exercise in iron-depleted, nonanemic women. Am J Clin Nutr 2003;77:441– 448. Hinton PS, Sinclair LM. Iron supplementation maintains ventilatory threshold and improves energetic efficiency in iron-deficient nonanemic athletes. Eur J Clin Nutr 2007;61:30 –39. Nissenson AR, Wade S, Goodnough T, et al. Economic burden of anemia in an insured population. J Manag Care Pharm 2005;11: 565–574. Weiss G, Fuchs D, Hausen A, et al. Iron modulates interferongamma effects in the human myelomonocytic cell line THP-1. Exp Hematol 1992;20:605– 610. Weiss G, Werner-Felmayer G, Werner ER, et al. Iron regulates nitric oxide synthase activity by controlling nuclear transcription. J Exp Med 1994;180:969 –976. Bartels U, Pedersen NS, Jarnum S. Iron absorption and serum ferritin in chronic inflammatory bowel disease. Scand J Gastroenterol 1978;13:649 – 656. Hansen TM, Hansen NE, Birgens HS, et al. Serum ferritin and the assessment of iron deficiency in rheumatoid arthritis. Scand J Rheumatol 1983;12:353–359. Lindgren S, Wikman O, Befrits R, et al. Intravenous iron sucrose is superior to oral iron sulphate for correcting anaemia and restoring iron stores in IBD patients: a randomized, controlled, evaluator-blind, multicentre study. Scand J Gastroenterol 2009; 44:838 – 845. Reprint requests Address requests for reprints to: Christoph Gasche, MD, Department of Medicine 3, Division of Gastroenterology and Hepatology, Medical University of Vienna, Währinger Gürtel 18-20, 1090 Wien, Austria. e-mail: [email protected]; fax: (43) (1) 404004735. Acknowledgments The authors acknowledge the contribution of all investigators at all study sites (listed in the Appendix). Conflicts of interest These authors disclose the following: Bernd Bokemeyer received consultancy honoraria from Vifor Germany and Pharmacosmos. Marcel Felder and Maja Gudehus are employees of Vifor Pharma (Switzerland). Tariq Iqbal and Philippe Marteau have received speakers honoraria from Vifor International. Jürgen Stein is a consultant for and has received speakers honoraria from Vifor International. Christoph Gasche has received grant and consultancy honoraria from Vifor Pharmacosmos A/S, Fresenius Medical Care, and Renapharma Sweden. The remaining authors disclose no conflicts. No conflicts of interests were disclosed to study participants in the informed consent form. Funding Vifor Pharma (Switzerland) sponsored this study and supported the development of the study design and preparation of the manuscript; an independent clinical research organization (Parexel International, Germany) conducted the trial and performed the statistical analysis; 276 EVSTATIEV ET AL and medical writing support was provided by Walter Fürst, SFL Regulatory Affairs & Scientific Communication, Switzerland, and was funded by Vifor Pharma, Switzerland. The study sponsors had no role in interpreting the results or in the decision for submission. Appendix The following institutions and local principal investigators participated in this study. Austria: Christoph Gasche, Department of Medicine III, Division of Gastroenterology and Hepatology, Medical University of Vienna; Friedrich Wewalka, Konventhospital der Barmherzigen Brüder Linz; Thomas Feichtenschlager, Krankenanstalt Rudolfstiftung, 4. Medizinische Abteilung mit Gastroenterologie und Hepatologie, Wien. Denmark: Jørn Brynskov, Med. Gastroenterology, Herlev Hospital, Herlev; Ole Bonderup, Medicinsk Gastroenterologsik Afdeling, Regions Hospitalet Randers, Randers; Vibeke Andersen, Medicinsk Afd., Regions Hospitalet Viborg, Viborg. France: Philippe Marteau, Gastro-Enterologie et Hepatologie, Hopital Lariboisiere, Paris Cedex 10; Jean-Louis Dupas, HepatoGastro-Enterologie, Hopital Nord, Amiens Cedex 1. Germany: Jürgen Stein, Department of Gastroenterology and Clinical Nutrition and Crohn Colitis Centre Rhein Main, Klinik für Viszeral und Ernährungsmedizin Katharina Kasper Kliniken, Frankfurt/Main; Ulrich Boecker, Gastroenterologie, Hepatologie, Infektiologie, Universitätsklinikum Mannheim, Mannheim; Thomas Ochsenkuehn, Medizinische Klinik und Poliklinik II, Klinikum der Universität München–Campus Grosshadern; Bernd Bokemeyer, Gastroenterologische Gemeinschaftspraxis Minden, Minden; Giuliano Ramadori, Universitätsklinikum, Göttingen; Ursula Seidler, Medizinische Hochschule für Hannover, Abteilung für Gastroenterologie; Ulrike Strauch, Klinik und Poliklinik für Innere Medizin I, Universitätsklinikum Regensburg; Andreas Sturm, Medizinische Klinik mit Schwerpunkt Hepatologie und Gastroenterologie, Charité-Campus Virchow Klinikum, Berlin; Stefan Zeuzem, Universitätsklinikum, Frankfurt/Main; Dietrich Hueppe, Gastroenterologische Gemeinschaftspraxis Herne; Carsten Büning, Charite Campus Mitte, Berlin; Martin Zeitz, Charite Campus Benjamin Franklin, Berlin. Norway: Jorgen Jahnsen, Medisinsk Dagpost, Aker Universitetssykehus HF, Oslo; Roald Torp, Sykehuset Innlandet, Medisinsk Avdeling, Hamar. Romania: Ioan Sporea, Spitalul Clinic Judetean de Urgenta, Timişoara; Adrian Goldis, Cabinet Particular Policlinic Algomed SRL, Timişoara; Mihail-Radu Voiosu, Spitalul Clinic Colentina, Bucharest; Mircea Manuc, Institutul Clinic Fundeni, Bucharest. Spain: Xavier Calvet Calvo, Corporación Sanitaria Parc Tauli, Sabadell; Sam Khorrami, Hospital Universitario Son Dureta, Palma de Mallorca. Sweden: Henrik Hjortswang, Endokrin-Och Mag/Tarmmedicinska Mottagningen, Universitetssjukhuset, Linköping; Per-Ove Stotzer, Medicinal Gastroenterology, Gastrosektionen, Göteborg; Anders Eriksson, Medicine Clinic, Medicinkliniken Plan 2, Sahlgrenska Universitetssjukhus/Östra Sjukhuset, Göteborg; Ragnar Befrits, Karolinska Universitetssjukhuset, Stockholm. Switzerland: Rémy Meier, Medizinische Universitätsklinik Kantonspital Liestal; Janek Binek, Kantonspital St Gallen. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 3 United Kingdom: Tariq Iqbal, University Hospital, Birmingham, Queen Elizabeth Hospital, Edgbaston; Anthony Barnabus Hawthorne, University Hospital, Wales, Cardiff; Peter Isaacs, Blackpool Victoria Hospital, Blackpool; Chris Probert, Bristol Royal Infirmary, Bristol Russia: Igor Lvovich Khalif, Federal State Institution “State scientific centre of coloproctology of Rosmedtechnology,” Moscow; Elena Alexandrovna Belousova, State Institution “Moscow Regional Scientific Research Clinical Institute named M.F. Vladimirsky,” Moscow; Oleg Nikolaevich Minushkin, State Health Institution of Moscow “City Clinical Hospital # 51,” Moscow; Andrey Yrievich Baranovskiy, St. Petersburg State Health Institution “City Clinical Hospital # 31,” St. Petersburg; Vladimir Ilich Simanenkov, St. Petersburg State Health Institution “City Hospital # 26,” St. Petersburg; Vladimir Borisovich Grinevich, Federal State Institution “442 District Military Clinical Hospital of Leningradsky Military District” of the Ministry of Defense of the Russian Federation, St. Petersburg; Elena Sergeevna Pasechnik, State Health Institution “Kaluga Regional Hospital,” Kaluga; Oleg Yrievich Dolgikh, Road Clinical Hospital on Samara Station “RGD,” Samara; Asfold Ivanovich Parfenov, State Health Institution of Moscow “Central Scientific Educational Institute Of Gastroenterology,” Moscow; Vladimir Vitalievich Rafalskiy, Municipal Treatment and Prophylactic Institution “Clinical Hospital No 1,” Smolensk; Alexey Alexandrovich Nizov, State Health Institution “Ryazan Regional Clinical Hospital,” Ryazan; Elena Alexandrovna Sishkova, Federal Health State Institution “Clinical Hospital # 122 named L.G. Socolov FMBA of Russia,” St. Petersburg; Olga Polikarpovna Alexeeva, State Health Institution “Nizhni Regional Clinical Hospital named N.A. Semashko,” Nizhni Novgorod; Oleg Lenianovich Solovyev, ZAO “Medical Scientific Production Association Clinic Dvizhenie,” Volgograd; Andrey Vladislavovich Kulyapin, MU City Clinical Hospital # 21, Ufa; Emiliya Prokhorovna Yakovenko, State Educational Institution of Higher Professional Education “Russian State Medical University Roszdrava” based on Federal State Institution “National Medical-Surgical Centre named by N.I. Pirogov Roszdrava,” Moscow; Vladimir Vasilievich Pavlenko, Stavropol State Medical Academy, Stavropol; Ildar Gazimdzhanovich Salikhov, Department of Gastroenterology, Kazan State Medical University, Republic Clinical Hospital, Kazan; Igor Borisovich Khlynov, Municipal Institution “City Clinical Hospital # 40,” Ekaterinburg; Irina Yurievna Pirogova, Municipal Healthcare Institution “City Clinical Hospital # 8,” Chelyabinsk; Olga Vladimirovna Krivtsova, Open JointStock Company (OAO) “Medical Unit Neftyanik,” Tyumen. Estonia: Lidia Randvee, MEDICUM, Ltd, Tallinn; Kyllikke Suurmaa, West Tallinn Central Hospital. Ukraine: Ivan Chopey, Departmental Clinical Hospital, Department of General Therapy, Uzhgorod National University, Faculty of Post-Graduate Education, Uzhgorod; Borys Palamar, Kyiv City Clinical Hospital # 3, Department of Gastroenterology, Kiev; Galyna Popik, Odessa Railway Clinical Hospital, Department of Therapy # 2, Odessa; Mykola Yabluchanskiy, State Treatment and Preventive Establishment “Central Clinical Hospital of Railways of Ukraine,” Department of Gastroenterology, Kharkiv National University named after V.N. Karazin, March 2013 Kharkiv; Iryna Klyaryts’ka, Department of Gastroenterology, Simferopol, Crimean State Medical University named after S.I. Georgievsky, Simferopol; Tetyana D. Zvyagintseva, Kharkiv City Clinical Hospital # 2, Department of Gastroenterology, Kharkiv; Natalia V. Kharchenko, Department of Gastroenterology, Kyiv City Clinical Hospital # 8, Kyiv; Galina D. Fadieienko, State Establishment “Institute of Therapy named after L.T. INTRAVENOUS IRON FOR PREVENTION OF ANEMIA 277 Mala of Academy of Medical Science of Ukraine,” Kharkiv; Valeriy ⌱. Vdovichenko, Department of Therapy # 1, Lviv City Municipal Clinical Emergency Hospital, Lviv National Medical University named after Danylo Halytskyi, Lviv; Yuriy M. Stepanov, Dnepropetrovsk State Medical Academy, Dnepropetrovsk; Lyubomyr V. Glushko, Ivano-Frankivsk National Medical University, Ivano-Frankovsk.