Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
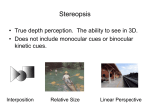
CHAPTER 15 Examination of the Patient—V DEPTH PERCEPTION tereopsis is an epiphenomenon of normal binocular vision (see Chapter 2). Its presence or absence is an important indicator of the state of binocularity in patients with ocular motility disorders. Barring a few notable exceptions (see Chapter 16), patients with essential infantile esotropia are stereoblind or, at best, have markedly reduced stereopsis, and the potential for regaining it is practically nil. In childhood strabismus with a later onset or in adults with acquired strabismus it is an important therapeutic goal to reestablish stereopsis. Whether this can be accomplished depends on many variables, among them the age of onset and the duration of the strabismus and the completeness of ocular realignment. S Development of Stereopsis Depth perception on the basis of binocular disparity is not fully developed at birth. Several studies using different paradigms such as line stereograms and a preferential looking procedure, random dots with a forced-choice preferential looking technique, and random dots with visually evoked responses have shown remarkably consistent findings: stereopsis is absent in almost all infants less than 3 months old, after which it rapidly develops 298 to normal levels which are reached by the sixth month of life. Interestingly, this rapid rate of maturation far exceeds that of visual acuity.11 The duration of the plasticity period of stereopsis in humans still needs to be established. For a review of the literature, see Teller31 and Birch.5 Stereopsis and Strabismus Patients with a large manifest deviation do not have useful stereopsis in casual seeing. Nevertheless, they can function quite well in space, making use of nonstereoscopic clues to depth perception, especially if the strabismus is of early origin. They may have trouble with fast-moving objects, such as flying balls, and this experience may be frustrating to young children. However, when the strabismus is acquired later in life the loss of stereopsis is felt acutely and may present a real handicap. It appears as if stereopsis is useful in the comprehension of complex visual presentations and those requiring good hand-eye coordination. Although the importance of stereopsis is often stressed, studies addressing the functional effects of stereoscopic deficits are sparse.8 It is always interesting and useful to determine whether a patient with strabismus has stereopsis Examination of the Patient—V or the potential for such. Some patients may respond to disparate stimulations with a degree of stereopsis if the targets are placed at the objective angle, as in a major amblyoscope. Some patients (e.g., intermittent exotropes) may respond with good stereoscopic acuity even when a stereoscope is used, although they seemingly may be unable to superimpose dissimilar targets. Such patients require strong fusional stimuli to keep their eyes aligned and to fuse. When they do, they gain motor and sensory fusion, often with a high degree of stereopsis. Some ophthalmologists use stereoscopic tests to determine whether patients with small or intermittent deviations have foveal suppression. If the stereoscopic threshold is low enough, they conclude that there is no foveal suppression.27 A positive result is certainly conclusive, but a negative result does not necessarily mean that foveal images are completely suppressed. There are patients who fuse all but disparate retinal stimuli, which are selectively suppressed. A positive stereoscopic response of a patient with a neuromuscular anomaly of the eyes at any fixation distance and in any part of the binocular field is of paramount importance prognostically and in directing treatment. This finding makes it mandatory that every effort be made, both nonsurgically and surgically, to restore to the patient full binocular cooperation with stereopsis at all fixation distances and in every part of the field. Testing for stereopsis should always be done after operations have properly aligned the eyes. The findings may give indications whether and how to follow up the operation by nonsurgical treatment. Testing for Stereopsis Equipment for testing stereopsis ranges from simple equipment to complex laboratory apparatus. Only tests that the ophthalmologist can conveniently apply in the office are discussed in this section. A test for stereopsis must incorporate two essential features. The two eyes must be dissociated; that is, each eye must be presented with a separate field of view, and each of the two fields or targets must contain elements imaged on corresponding retinal areas. Thus a frame of reference is provided, and disparately imaged elements can be fused and seen stereoscopically. In addition, 299 there should be fiducial marks that permit the examiner to check whether both eyes are used simultaneously. Major Amblyoscope or Stereoscope The targets may be opaque or transparent and may be used in a major amblyoscope or stereoscope. Both devices have mechanically separated fields of view, are set optically at infinity, and use exchangeable targets. The advantage of the major amblyoscope is that its arms can be set at the patient’s angle of deviation, thus allowing control of the retinal area being stimulated. Similarly the stereoscope may be used with prisms, but this procedure may not be accurate, and the distortions induced by prisms may become bothersome. The number and variety of targets are limited only by the ingenuity of the designer and user, but standard sets of targets and cards are commercially available for the different major amblyoscopes and stereoscopes. Targets of special interest in the present context are those that contain objects with differing amounts of disparity (e.g., the Keystone DB6 card), so that they appear at different relative depth distances. The object seen in depth, which has the least disparity, denotes the patient’s stereoscopic threshold. Stereogram A useful clinical application can be made of the simple stereogram consisting of eccentric circles, one set seen with each eye (see Fig. 2–15). If the patient reports that two fiducial marks and two circles are seen, but not in depth, one should inquire whether the two circles are concentric. They cannot be seen concentrically unless they are also seen stereoscopically. If they are seen eccentrically, one may now ask whether the inner circles are closer to the right or left of the outer circle. The patient’s answer determines whether the disparate elements are suppressed in the right or the left eye. Titmus Stereo Test Vectograph cards dissociate the eyes optically. A vectograph consists of Polaroid material on which the two targets are imprinted so that each target is polarized at 90⬚ with respect to the other. When the patient is provided with properly oriented Po- 300 Introduction to Neuromuscular Anomalies of the Eyes FIGURE 15–1. The Titmus Stereo Test. laroid spectacles, each target is seen separately with the two eyes. This principle is used in the Titmus Stereo Test (Fig. 15–1). In this test a gross stereoscopic pattern representing a housefly is provided to orient the patient and to establish whether there is gross stereopsis (threshold: 3000 seconds of arc). In testing young children, one must ask questions the child will understand. For example, one may ask the child to take hold of the wings of the fly. If the child sees them stereoscopically, the child will reach above the plate. It is amusing to watch the child’s startled look when he or she does so. It is indeed an eerie feeling not to have a tactile sensation of a seen object. Some children, though they have stereopsis, will touch the wings on the plate because they ‘‘know’’ they are there. The examiner must explain to these children that he or she does not inquire about what they know, but what they see. The Polaroid test also contains three rows of animals, one animal in each row imaged disparately (thresholds: 100, 200, and 400 seconds of arc, respectively). The child is asked which one of the animals stands out. The animal figures contain a misleading clue. In each row one of the animals, correspondingly imaged in two eyes, is printed heavily black. A child without stereopsis will name this animal as the one that stands out. Last, the Titmus test contains nine sets of four circles arranged in the form of a lozenge. In this sequence the upper, lower, left, or right circle is disparately imaged at random with thresholds ranging from 800 to 40 seconds of arc. If the child has passed the other tests, he or she is now asked to ‘‘push down’’ the circle that stands out, beginning with the first set. When the child makes mistakes or finds no circle to push down, the limits of stereopsis are presumably reached. If there is doubt whether the patient actually does see stereoscopically, one may occlude one eye and inquire whether there is a difference in appearance, say, of the housefly, with one or both eyes open. And since only horizontal disparity produces stereopsis, one can also turn the plate 90⬚, which should block out the stereoscopic effect. Because of its simplicity, the Titmus Stereo Test is widely used. On the basis of this test alone, however, one is not always justified in stating simply that ‘‘the patient has no stereopsis,’’ that is, that there is no sensitivity for disparate stimuli. One must keep in mind that the vectograph test is used for testing near vision. Some patients suppress disparate stimuli at near but respond to them in distance fixation, or vice versa, usually when the deviation is intermittent at one fixation dis- Examination of the Patient—V tance and constant at the other. If such a pattern is suspected, it is always wise to supplement the vectograph test with a projected vectograph test at distance fixation (Polaroid Vectographic ProjectO-Chart, American Optical Reichert) or with the B-VAT (Mentor) projection device. In recent years much emphasis has been placed on the use of stereoacuity testing as a screening method to detect anomalies of binocular function.9, 29, 30 Normal stereoacuity is said to preclude suppression, amblyopia, or heterotropia, and a subnormal test result may indicate the presence of such anomalies. In applying the Titmus test as a screening device, Simons and Reinecke29 found that, with the exception of the fine stereoacuity circles 5 to 9, this test often is unreliable in differentiating patients with amblyopia and heterotropia from those with normal vision. Moreover, the Titmus test is capable of indicating an artifactual stereocapability when none actually exists (see also Köhler and Stigmar14). Some of the circles of the Titmus test may be selected even by stereoblind observers because they look ‘‘different’’ and not because they are seen stereoscopically. Some patients notice an image jump in the disparate portions of the test target (e.g., the wings of the fly) 301 when fixating alternately and utilize this clue to pass the Titmus test despite the fact that they may be stereoblind on any of the tests using random dots.29 Archer1 described a test based on dynamic circles designed to mimic the Titmus circles as closely as possible, while eliminating lateral displacement cues as well as the possibility of passing the test by alternation. Random-Dot Stereograms To avoid any such visual clues, two tests are available that use random-dot stereograms.2 The physiologic principle underlying these tests has been discussed in Chapter 2. Random-dot stereograms are devoid of any monocular clues, and the patient has no way of guessing what the stereofigure is and where it is located on the test plate.13 Reinecke and Simons28 introduced the random-dot E test (RDT) (Fig. 15–2), which contains three cards and Polaroid spectacles. One card is a bas-relief model of the stereotest figure and is used to show the child what to look for. One of the two other test cards contains the E stereo figure, and the other is stereoblank with an identical random-dot background. The test is performed FIGURE 15–2. Random-dot E test set. (From Simons K, Reinecke RD: Amblyopia screening and stereopsis. In Symposium on strabismus: Transactions of the New Orleans Academy of Ophthalmology. St. Louis, Mosby–Year Book, 1978, p 15.) 302 Introduction to Neuromuscular Anomalies of the Eyes FIGURE 15–3. A, The TNO test. B, The random-dot stereogram offers no monocular clues as to the presence of a large circle in the center of the upper right quadrant and a smaller circle in the center of the lower left quadrant. (From Noorden GK von: Present status of sensory testing in strabismus. In Symposium on Strabismus: Transactions of the New Orleans Academy of Ophthalmology. St. Louis, Mosby–Year Book, 1978, p 51.) by holding both test cards 50 cm in front of the patient, who is then requested to indicate which card contains the letter E. The test is simple to perform, and the patient will give a ‘‘pass’’ or ‘‘fail’’ response. It can be quantitated by increasing the testing distance from the patient. Many modifications of the RDT have become available in the meantime.6 Random-dot stereopsis can be measured also for distance with the Mentor BVAT II-SG computerized testing system (Mentor O & O, Norwell, MA). This is particularly useful in intermittent exotropia.32 TNO Test Another procedure, the TNO test, is based on a similar principle but has the advantage of eliciting quantitative responses without changing the testing distance. This test uses a pair of red-green spectacles and a test booklet (Fig. 15–3). Each test plate in the booklet consists of a stereogram in which the half-images have been superimposed and printed in complementary colors (anaglyphs). The test plates, when viewed binocularly with redgreen spectacles by a normal subject, will elicit Examination of the Patient—V perception of an image in depth. The TNO test is graded to provide retinal disparities ranging from 15 to 480 seconds of arc. Comparative studies have shown that this test compares favorably with the Titmus test when used as a screening device.26, 33 Together with the Lang test (see below) it is the preferred test in our clinic. It must be emphasized, however, that even random-dot testing of stereopsis is not a fail-safe method to assess visual acuity and binocular function in preschool and school-age children, since normal levels of stereoacuity have been observed in anisometropic and visual deprivation amblyopia.3, 7, 21 How should stereopsis, determined with any of the tests, be recorded? Cards and vectographs that attempt to qualify stereopsis are graded in different ways. Some use artificial scales (such as the Sheppard scale); many speak of percentage of stereopsis, assuming a certain threshold to mean 100%. All this is misleading and arbitrary. The only proper way to record stereopsis is by the amount of disparity incorporated into the target. It is unequivocal, and it should be generally understood when it is stated that a patient has stereopsis with a threshold of 400 or 100 or 40 seconds of arc or whatever the threshold may be. Lam and coworkers15 evaluated the response of normal subjects to various visual function tests, including stereopsis. They found a wide range of responses in completely normal subjects, thus raising the question which level of stereopsis reflects normalcy (see also Fisher9). It appears as a difficult task to identify a cutoff value separating 303 normals from abnormals. These authors further stated that because of the fact that more than 40% of normal children demonstrate stereoacuity of less than 40 seconds of arc, random-dot testing is not a real measure of a biological function. Awaya et al.4 studied the effects of aniseikonia on stereopsis measurements. With their aniseikonia test, they found that aniseikonia of 7% to 13% is still compatible with binocular fusion. However, aniseikonia of greater than 5% is incompatible with testing higher levels of stereoacuity with the Titmus and TNO tests. Lang Test Occasionally, young children will refuse to wear Polaroid or red-green spectacles, and observing the position of the eyes while the patient is being tested for stereopsis may be desirable. To overcome these difficulties, Lang17, 18 reported a new test (the Lang test) based on panographic presentation of a random-dot pattern. Glasses are not needed to recognize the stereoscopic images of a star, a car, and a cat (Fig. 15–4) embedded in random dots on the test card. A separate image is provided to each eye through cylindrical lenses imprinted on the surface lamination of the test card (Fig. 15–5) When held at a testing distance of 40 cm in the frontoparallel plane in front of the patient (Fig. 15–6), the disparity of the car and star is 600 seconds and of the cat 1200 seconds of arc.17 A revised version of this test (Lang II test)19 with smaller disparities and a less dense FIGURE 15–4. Stereoscopic images embedded in random dots of the Lang test. (From Lang J: A new stereotest. J Pediatr Ophthalmol Strabismus 20:72, 1983.) 304 Introduction to Neuromuscular Anomalies of the Eyes and the object is seen in depth does recognition take place. Two-Pencil Test FIGURE 15–5. Cylinder gratings provide separate images for each eye. (From Lang J: A near stereotest. J Pediatr Ophthalmol Strabismus 20:72, 1983.) arrangement of random dots has become available. One of the stimuli in the Lang II test is perceived binocularly and serves as a control mark. The subject can see it also in the absence of stereopsis. Test results obtained with the older and newer version of the Lang test have been reported to be comparable.25 The advantage of the Lang I test is that it can be performed in children as young as 6 months of age. If the baby stares for a few seconds at the card one can infer the presence of stereopsis, following the same reasoning underlying the preferential looking testing technique. Stereo tests that use random dots are an accurate and established method to measure stereoacuity; however, the results obtained with different tests will vary widely.21 As stated in Chapter 2, testing based on random dots exposes the child to visual demands that are different from and more difficult than those prevailing under more casual conditions of seeing. For instance, random-dot tests contain no information about the shape or nature of the object hidden in the visual noise of random dots. Only when the images from the right and left eye are combined at the neural level The two-pencil test, though somewhat crude, indicates how well a child is able to cope with a simple visual-motor task that is at least partially based on intact stereopsis. The two-pencil test was popularized by Lang but must have been known at least 388 years ago (1613) as shown by a sketch by Peter Paul Rubens to illustrate Aguilonius’ textbook on optics12 (Fig. 15–7). In this illustration, perhaps the oldest one available that shows the superiority of binocular over monocular vision, the cherub teasingly holds a vertical rod in front of the scholar who tries to touch the rod with his index finger from the side while keeping his left eye closed. He will not accomplish this task easily, of course, because his stereopsis cannot function with one eye closed, and the three cherubs anticipate the scholar’s apparent lack of skill with great merriment. We agree with Lang16 that the test is better performed by approaching the rod from above, since this makes better use of horizontal disparity detectors and approximates daily manual tasks that require good stereopsis, such as pouring milk into a glass or hitting a nail with a hammer. There is no question that monocular clues to depth perception (see p. 25) also are involved in completing this test. However, the drastic change of performance when one eye is covered or, for instance, when a child is fusing through bifocals but has a manifest deviation when looking through the upper segments suggests that stereopsis must be involved to a large extent in this visual task. The test is performed as shown in Figure 15–8. Its threshold values have been estimated to be between 3000 and 5000 seconds of arc, depending on the subject’s interpupillary distance and arm length.20 Finally, we must mention recent developments aimed at testing stereopsis objectively in infants. With the current emphasis on early diagnosis and treatment of strabismus, such efforts are of more than theoretical interest. The principle of such tests is based on the ability to elicit optokinetic nystagmus2, 10 or saccadic eye movements22 by electronically generated stereograms moving back and forth on a television screen. Although such methods are still largely confined to the laboratory, Examination of the Patient—V FIGURE 15–6. The Lang test. The child points to the stereoscopic image. (From Lang. J: A new stereotest. J Pediatr Ophthalmol Strabismus 20-72, 1983.) FIGURE 15–7. Illustration by Peter Paul Rubens in Aguilonius’ textbook on optics. (From Jaeger W: Die Illustrationen von Peter Paul Rubens zum Lehrbuch der Optik des Franciscus Aguilonius/1613. Heidelberg, Verlag Brausdruck, 1976, p 36.) 305 306 Introduction to Neuromuscular Anomalies of the Eyes one would hope that simplified equipment will eventually become available for use in a clinical environment. FIGURE 15–8. The two-pencil test. A, Examiner holds pencil vertically in front of the patient. The patient’s task is to touch the upper tip of the examiner’s pencil with one swift movement from above. B, Patient passes the test with both eyes open. C, Patient fails the test with one eye closed (or when both eyes are open but stereopsis is absent). (From Noorden GK von: Atlas of Strabismus, ed 4. St Louis, Mosby–Year Book, 1983.) REFERENCES 1. Archer SM: Stereotest artifacts and the strabismus patient. Graefes Arch Clin Exp Ophthalmol 226:313, 1988. 2. Archer SM, Miller KK, Helveston EM: Stereoscopic contours and optokinetic nystagmus in normal and stereoblind subjects. Vision Res 27:841, 1987. 3. Avilla C, Noorden GK von: Limitation of the TNO random dot stereo test for visual screening. Am Orthopt J 31:87, 1981. 4. Awaya S, Sugawara M, Horibe F, et al: Studies on aniseikonia and stereopsis with the ‘‘new aniseikonia test.’’ In Reinecke RD, ed: Proceedings of the Fourth Meeting of the International Strabismological Association. New York, Grune & Stratton, 1984, p 549. 5. Birch EE: Stereopsis in infants and its developmental relation to visual acuity. In Simons K, ed: Early Visual Development, Normal and Abnormal. New York, Oxford University Press, 1993, p 224. 6. Birch EE, Salamao S: Infant random dot stereoacuity cards. J Pediatr Ophthalmol Strabismus 35:86, 1998. 7. Campos E, Enoch JM: Amount of aniseikonia compatible with fine binocular vision: Some old and new concepts. J Pediatr Ophthalmol Strabismus 17:44, 1980. 8. Fiedler AR, Moseley MJ: Does stereopsis matter in humans? Eye 10:233, 1996. 9. Fisher NF: Stereopsis revisited. J Pediatr Ophthalmol Strabismus 34:76, 1997. 10. Fox R, Lehmkuhle S, Leguire LE: Stereoscopic contours induce optokinetic nystagmus. Vision Res 18:1189, 1978. 11. Held R: What can rates of development tell us about underlying mechanisms? In Granud C, ed: Visual Perception and Cognition in Infancy. Hillsdale, NJ, Erlbaum, 1993, p 75. 12. Jaeger W: Die Illustrationen von Peter Paul Rubens zum Lehrbuch der Optik des Franciscus Aguilonius/1613. Heidelberg, Verlag Brausdruck, 1976, p 36. 13. Julesz B: Foundations of Cyclopean Perception. Chicago, University of Chicago Press, 1971. 14. Köhler L, Stigmar G: Vision screening in four year old children. Acta Paediatr Scand 62:17, 1973. 15. Lam S, LaRoche GR, De Backer I, Macpherson H: The range and variability of ophthalmological parameters in normal children aged 41⁄2 to 51⁄2 years. J Pediatr Ophthalmol Strabismus 33:251, 1996. 16. Lang J: Der Treffversuch zur Prüfung des stereoskopischen Sehens. Klin Monatsbl Augenheilkd 165:895, 1974. 17. Lang J: New stereotests. In Boschi MC, Frosini R, eds: Proceedings of the International Symposium on Strabismus, Florence, Italy, June 21–23, 1982, p 177. 18. Lang J: A new stereotest. J Pediatr Ophthalmol Strabismus 20:72, 1983. 19. Lang J: Nine years’ experience with the Lang stereotest. In Tillson G, ed: Transactions of the Seventh International Orthoptic Congress. Nuremberg, June 2–6, 1991, p 163. 20. LaRoche R, Noorden GK von: Theoretical and practical evaluation of a simple stereotest (abstract). Invest Ophthalmol Vis Sci 22 (suppl):266, 1982. 21. Marsh WR, Rawlings SC, Mumma JV: Evaluation of clinical stereoacuity tests. Ophthalmology 87:1265, 1980. 22. Mizukami Y, Awaya S, Koizumi E, Kamiya A: The investigation of stereoacuity in infants by the new TV random dot stereotest. Folia Ophthalmol Jpn 38:1182, 1987. Examination of the Patient—V 23. Noorden GK von: Present status of sensory testing in strabismus. In Symposium on Strabismus: Transactions of the New Orleans Academy of Ophthalmology. St Louis, Mosby–Year Book, 1978, p 51. 24. Noorden GK von: Atlas of Strabismus, ed 4. St Louis, Mosby–Year Book, 1983. 25. Nüssgens Z, Czerwonka B, Roggenkämper P: Examination of the new Lang test. Strabismus 1:69, 1993. 26. Okuda F, Apt L, Wanter B: Evaluation of the TNO random-dot stereogram test. Am Orthopt J 27:124, 1977. 27. Parks MM: Stereoacuity as an indicator of bifixation. In Arruga A, ed: International Strabismus Symposium, University of Giessen, Germany 1966. Basel, S Karger, 1968, p 258. 307 28. Reinecke R, Simons K: A new stereoscopic test for amblyopia screening. Am J Ophthalmol 78:714, 1974. 29. Simons K, Reinecke RD: A reconsideration of amblyopia screening and stereopsis. Am J Ophthalmol 78:707, 1974. 30. Simons K, Reinecke RD: Amblyopia screening and stereopsis. In Symposium on Strabismus: Transactions of the New Orleans Academy of Ophthalmology. St Louis, Mosby–Year Book, 1978, p 15. 31. Teller DY: First glances: The vision of infants (Friedenwald lecture). Invest Ophthalmol Vis Sci 38:2183, 1997. 32. Yildrim C, Altinsoy I, Yakut E: Distance stereoacuity norms for the mentor B-VAT II-SG video acuity tester in young children and young adults. J AAPOS 2:26, 1998. 33. Walraven J: Amblyopia screening with random-dot stereogram. Am J Ophthalmol 80:893, 1975.