Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
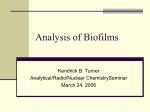
Volume 17 • Number 7 • July-August 2012 Indexed by the US National Library of Medicine and PubMed Biofilms in Dermatology Aron G. Nusbaum, BS1; Robert S. Kirsner, MD, PhD1,2; Carlos A. Charles, MD3 Department of Dermatology & Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, FL, USA 2 University of Miami Hospital, Miami, FL, USA 3 Department of Dermatology, Weill Cornell Medical College, New York, NY, USA 1 ABSTRACT Biofilms are diverse communities of microorganisms embedded within a self-produced matrix of extracellular polymeric substance which are firmly attached to biotic or abiotic surfaces. Approximately 80% of all human infections are associated with biofilms and evidence for their role in an ever-growing number of cutaneous disorders is constantly unfolding. Biofilms present a difficult challenge to clinicians due to their persistent nature, inability to be cultured with standard techniques, and resistance to conventional antimicrobial therapy. Although limited treatment options are presently available, better understanding of the molecular biology of biofilms and their pathogenicity will likely lead to the development of novel anti-biofilm agents for clinical use. Key words: bacterial colonization, biofilms, skin infection, wounds Introduction While bacteria have classically been viewed from the perspective of planktonic, free floating pathogens proliferating and exerting their virulence as individual organisms, it is now recognized that microbes also can exist as multicellular consortiums known as biofilms.1,2 (Figure 1) Several advantages exist for bacteria that live in a biofilm phenotype including structural stability, firm adherence to biotic or abiotic surfaces, increased virulence, and resistance to both antimicrobial therapy and the host immune response. Organisms within biofilms are embedded in a glycocalyx, a self-produced matrix of extracellular polymeric substance (EPS) composed of polysaccharides, proteins, lipids, and extracellular DNA (eDNA). The EPS is considered to be the hallmark of biofilm formation and in addition to facilitating attachment, it also serves a protective function by preventing neutrophilic penetration, 2 masking phagocytic detection of opsonins, 3 and sequestering host antibodies, as well as complement factors.4 The formation and behavior of the entire biofilm community is directed by signaling molecules that are produced when microorganisms reach a critical number. This phenomenon is termed quorum sensing (QS) and has also been shown to regulate the expression of virulence factors as well as modulate host immunity.5 Biofilms have been associated with approximately 80% of all human infections, yet their detection is extremely difficult with the use of routine culture techniques.6 New methods to detect biofilm-associated organisms are under development. For example, denaturating gradient gel electrophoresis and Figure 1. Scanning electron micrograph demonstrating the presence of mixed species biofilm in a chronic wound. Both cocci and bacilli are seen embedded in an amorphous matrix characteristic of biofilm formation. Figure from James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen. 2008 Jan-Feb;16(1):page 42, Figure 1D. Reprinted with permission from John Wiley and Sons. 16S rRNA sequencing are currently being used successfully in the research setting and may someday be available for use in clinical practice.7,8 Currently, biofilms cannot be visualized in skin biopsies submitted for routine light microscopy due to collapse of the glycocalyx during the dehydration process9 and require special techniques for visualization of the intact biofilm structure such as electron, epifluorescence, or confocal laser scanning microscopy ALSO IN THIS ISSUE: A Look at Epidermal Barrier Function in Atopic Dermatitis: Physiologic Lipid Replacement and the Role of Ceramides (page 6) & Update on Drugs (page 10) (CLSM). Conventional therapy is characteristically ineffective against biofilms, as the minimum inhibitory concentration (MIC) of antimicrobial agents has been shown to be 10 to 1000 fold greater than for planktonic organisms.10 Antimicrobial resistance can be attributed to the EPS serving as a physical barrier to antibiotic penetration, plasmid exchange facilitated by close proximity between organisms, and the low metabolic activity and growth rate observed within biofilms.4,6,11 In addition, decreased susceptibility to antimicrobial agents may also be related to an increased frequency of mutations, which result in upregulation of efflux pumps and antibiotic degrading enzymes such as betalactamase.12 Biofilms present a unique challenge to today’s clinician and evidence for their involvement throughout dermatology is constantly unfolding. Herein, we will present current knowledge regarding the role of biofilms in cutaneous disease along with potential therapeutic strategies for the management of biofilmassociated infections. Wounds In the United States, approximately 6.5 million patients are affected by chronic wounds13 and their treatment significantly impacts the health care system with an estimated $25 billion spent annually.14,15 Chronic wounds present an optimal environment for microbial proliferation and while the association between infection and delayed wound closure has long been established, little is known regarding the mechanisms by which bacteria inhibit healing. In a clinical study of 66 wounds of various etiologies, 60% of chronic wounds were shown to contain biofilms as compared to 6% of acute wounds, indicating the possible role of biofilms in wound chronicity.16 This study also demonstrated the presence of multiple species within the chronic wound environment existing in the form of highly organized biofilms. Traditional cultures identified Staphylococcus, Pseudomonas, and Enterococcus as the predominant organisms, while molecular analysis additionally revealed the presence of strictly anaerobic species.16 In fact, a recent profiling study utilizing 16S RNA sequencing in 15 chronic wounds demonstrated an average of 17 genera in each wound, with the majority being anaerobic bacteria.17 These polymicrobial communities have long been underappreciated due to the shortcomings of standard culture techniques, yet they have important clinical implications as interspecies interactions are likely operative in promoting biofilm pathogenicity.17 Biofilms have a negative effect on wound healing as evidenced by their ability to induce keratinocyte apoptosis in vitro18 and inhibit re-epithelialization in an in vivo animal wound model.19 In addition, biofilms may also augment the inflammatory response characteristic of chronic wounds, thus promoting tissue damage and further contributing to the nonhealing phenotype.20 It has been suggested that a biofilm-based wound care regimen would incorporate a multifaceted approach with debridement as its most essential component.6 In addition to removing devitalized tissue that serves as a fertile environment for bacteria, debridement physically disrupts the biofilm structure, resulting in a period of reassembly during which organisms are increasingly susceptible to antimicrobial therapies.21 Novel antibiofilm agents that have been proposed for use in chronic wounds 2 include lactoferrin, which inhibits bacterial adhesion and has been shown to decrease biofilm mass,4 as well as xylitol, which disrupts glycocalyx formation. 7 When used in combination, these agents exhibit a synergistic effect and, in vitro, have been shown to decrease the viability of a dual species Staphylococcus aureus (S. aureus) and Pseudomonas aeruginosa biofilm when added to a silver dressing.22 Future anti-biofilm therapies may also target quorum sensing, as promising results were shown in a murine wound model, where RNAIII inhibiting peptide, a specific staphylococcal quorum sensing inhibitor, resulted in deficient biofilm formation and improved the rate of healing.19 Atopic Dermatitis Atopic dermatitis (AD) affects 10-20% of children with 60% of cases occurring within a child’s first year and 85% before the age of 5.23 Although spontaneous resolution is seen in a majority of patients by 18 years of age, many cases persist into adulthood as evidenced by the 1-3% prevalence of AD among the adult population.24 It is well known that AD patients are colonized with S. aureus and this organism has been shown to exist in both dry skin as well as areas of severe dermatitis.25 Disease severity has been directly correlated to the degree of S. aureus colonization and therapy generally fails to improve symptoms in the presence of high S. aureus counts.26 CLSM has demonstrated the presence of biofilms on mouse skin inoculated with AD S. aureus isolates,27 as well as in skin stripping and biopsy specimens from 11 AD patients.9 The difficulty in eradicating S. aureus colonization with conventional antibiotic therapy may be due to the presence of biofilms. It is hypothesized that normal skin microflora, such as Staphylococcus epidermidis (S. epidermidis), has an important role in suppressing the growth of S. aureus by metabolizing sebum and, thus, creating a low pH environment that is inhibitory to pathogenic organisms.28 Since S. aureus and S. epidermidis exhibit similar antibiotic susceptibility, a logical rationale for therapy may be to specifically target S. aureus biofilm. A recent in vitro study29 examined the effects of farnesol and xylitol on S. aureus biofilms and showed that each agent alone inhibited a different stage of biofilm formation and, when used concomitantly, they inhibited biofilm formation and also disrupted mature biofilm. The MIC of farnesol was lower for S. aureus than S. epidermidis, indicating the potential of this agent to selectively target the pathogenic organism. In a clinical study of 17 patients with AD,28 a 0.02% farnesol and 5% xylitol (FX) combination emollient cream significantly decreased the number of S. aureus organisms, as well as the ratio of S. aureus to total aerobic skin microflora with an observed increase in coagulase-negative staphylococci. S. aureus biofilm, demonstrated in the intercellular spaces of the stratum corneum prior to therapy, was completely absent after 7 days of FX topical application. No adverse effects of FX were noted after 4 weeks of therapy. Ideal topical agents for the treatment of AD should selectively reduce pathogenic biofilm and restore the balance of skin microflora without the irritant effects typically seen with current topical germicides.29 Acne Acne affects approximately 45 million individuals in the United States with most patients aged 12-24 years old, where the • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 prevalence has been shown to be as high a s 85%.30 Evidence for the presence of biofilms in acne is predominantly derived from the ability of Propionibacterium acnes (P. acnes) to form biofilms both in vitro and on implanted medical devices. In addition, sequencing of the P. acnes genome reveals the presence of genes involved in the production of EPS and QS molecules.31 P. acnes strains isolated from acne patients form biofilms in vitro that are characterized by increased lipase activity as compared to planktonic organisms.32 This may explain a pathogenic role for P. acnes biofilms in acne, as lipase is not only a well known virulence factor, but it also produces irritant fatty acids that promote inflammation33 and enhance P. acnes adhesion to the sebaceous follicle.34 Keratin plugging has long been considered a key component of acne pathogenesis, and the adhesive properties of the EPS produced by P. acnes biofilms in sebum may be responsible for the tenacious binding of keratinocytes to the infundibular epithelium.35 The observed clinical trend towards decreased efficacy of topical antibiotics may be explained by their usage over time or by the presence of biofilms, as biofilm-associated P. acnes exhibits increased resistance to commonly used anti-acne agents.36 In addition, the extended length of treatment necessary for acne to respond to oral antibiotics further suggests that biofilms are a key pathogenic factor in this condition.37 An in vitro study32 evaluating multiple anti-acne agents alone or in combination found that only 0.1% triclosan, 5% benzoyl peroxide + 0.5% erythromycin, and 5% benzoyl peroxide + 1% clindamycin were effective in both reducing biofilm mass and killing >99% of biofilm-associated P. acnes. Interestingly, 5% benzoyl peroxide alone was ineffective unless combined with erythromycin or clindamycin, possibly as a result of antibiotics inhibiting protein synthesis and, therefore, making P. acnes cells vulnerable to benzoyl peroxide generated radicals. It should be noted that although 30mM azelaic acid was bactericidal, it did not reduce biofilm mass. Minocycline was the only agent in its class that removed biofilm and displayed the greatest bactericidal effect of all the tetracyclines tested. It has been postulated that the success of isotretinoin therapy may be related to reduction of sebaceous gland size with a subsequent decrease in sebum production, thus depleting the nutrient source for P. acnes biofilm.35 The effectiveness of photodynamic therapy may also be due to an indirect effect on biofilms mediated by decreased sebaceous gland activity.38 Future acne therapies may incorporate specific biofilm production antagonists or agents that alter the physical and biochemical properties of the pilosebaceous unit in order to create an unfavorable environment for P. acnes biofilm.39 Candidiasis Candida albicans (C. albicans) is a dimorphic yeast that typically exists in a commensal state on mucocutaneous surfaces.40 In the setting of predisposing factors such as immunosuppression, systemic antibiotic therapy, endocrinopathies, excessive moisture, or ill-fitting dentures, this organism becomes an opportunistic pathogen causing local infections of the skin, nails, and mucous membranes, and in some cases disseminated systemic disease.41 Recent in vivo animal models demonstrate the ability of C. albicans to form biofilms on mucosal surfaces suggesting that biofilm formation and its characteristic tissue adherence play a key role in promoting Candida infections in these sites.42 Although it has been suggested that C. albicans forms mucosal biofilms when there are changes in host immunity or alterations in the mucosal ecology or integrity, it is unknown if this organism always exists as a biofilm, even in its commensal state.43 Cutaneous Candida infections such as intertrigo and onychomycosis may also involve biofilm-associated organisms, although this has not been studied. Oropharyngeal candidiasis (OPC) is seen in 5% of newborns, 10% of the elderly, and is the most common opportunistic infection in AIDS, affecting 90% of these patients. 42 Acute pseudomembranous candidiasis, or thrush, is a common clinical presentation with its characteristic white plaques presumably due to biofilm formation.44 In a murine OPC model, BCR1, the master transcription factor for Candida biofilms, was shown to be involved in attachment to host cells, promoting epithelial invasion, and protecting C. albicans from neutrophilic attack.45 C. albicans biofilms have also been shown to overexpress the cell wall polysaccharide, β-glucan, which may be involved in regulating the host immune response and promoting antifungal resistance.44 Chronic atrophic candidiasis, also known as denture stomatitis, is seen in up to 70% of denture wearers and is caused by ill-fitting dentures compromising what is normally an effective mucosal barrier.46 Denture stomatitis can be directly linked to biofilm formation as dentures are abiotic surfaces that have been demonstrated to harbor C. albicans biofilms.47 Angular cheilitis is commonly seen in patients with denture stomatitis, suggesting that biofilms may also play a role in this type of infection. While routine and uncomplicated candidiasis typically responds to treatment with traditional antifungals such as the azoles, the ineffectiveness of these agents in recurrent and persistent Candida infections is thought to result from the presence of biofilms. Most of the information regarding Candida biofilm drug resistance stems from in vitro studies, yet these findings are likely applicable to the clinical setting, as in vitro and in vivo C. albicans biofilms have similar architectural structure, growth kinetics, and genetic determinants.42 Candida biofilms exhibit a 30 to 2000 fold increase in resistance to amphotericin B, fluconazole, itraconazole, and ketoconazole as compared to planktonic organisms.48 Subpopulations of cells that exhibit extremely high levels of antifungal resistance49 as well as the drug penetration barrier function of the EPS 50 have been demonstrated in C. albicans biofilms. Recently developed antifungal agents such as the echinocandins and liposomal formulations of amphotericin B have been shown to be effective against C. albicans biofilms,51 but are currently available only for intravenous administration. Gentian violet has shown efficacy on in vitro isolates from OPC lesions and may act by inhibiting germination and forming radicals, which enhance penetration through the biofilm matrix.52 Additional therapeutic strategies that may hold promise for the treatment of Candida biofilm infections include quorum sensing inhibitors, vaccines, anti-candidal antibodies, cytokine therapy, and specific inhibitors of BCR1 and its target genes.53 Fillers Adverse reactions to fillers were previously thought to be due to allergic or foreign body reactions, yet it is now recognized that painful inflammatory nodules in this setting should be • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 3 considered to be infectious in etiology and immediately treated with antibiotic therapy.54 Biofilms are possibly the causative factor as evidenced by the persistent nature of filler reactions, difficulty in culturing organisms with routine measures, and the reported high incidence of biofilm-infected medical implants. This has been corroborated by visualization of bacterial aggregates with surrounding eDNA within the filler gel and intervening dermis in biopsies of 8 patients with reactions to polyacrylamide gel.55 Seven of these patients had been treated with intralesional or systemic steroids, suggesting that reactions to polyacrylamide fillers be treated with antibiotics and that steroids should be avoided. The choice of antibiotic agents as well as the length and mode of administration should be selected based on the filler type and the onset, severity, and duration of infection. Incision and drainage for fluctuant lesions is recommended. Additionally, performing biopsy and cultures is essential for late onset reactions or when particulate fillers are used, keeping in mind that routine cultures are often negative in the case of biofilms.54 Finally, the performance of filler injections with aseptic precautions is crucial and antibiotic prophylaxis should be considered when injecting into highly colonized areas or acne affected skin. Other Dermatologic Diseases S. aureus biofilms have been demonstrated in specimens of bullous impetigo and pemphigus foliaceus 9 while biofilms containing both S. aureus and Streptococcus pyogenes have been identified in non-bullous impetigo.56 The effects of acetic acid (AA) and hydrochloric acid on S. aureus biofilm formation were evaluated in bullous impetigo and pemphigus foliaceus isolates and were both shown to decrease glycocalyx production. 9 AA had a superior effect in reducing biofilm-associated S. aureus counts, indicating a specific effect of AA unrelated to low pH. In the clinical setting, AA 2.5% ointment was reported to reduce S. aureus counts in pemphigus foliaceus lesions, although no supporting data was presented.9 Biofilm formation has also been demonstrated in a murine model inoculated with S. aureus isolated from a furuncle.57 Treatment with a combination of imipenem and roxithromycin showed significantly reduced S. aureus counts in lesional skin, while treatment with either agent alone showed no effect. Biofilms have been implicated in miliaria by a clinical study in which only EPS producing S. epidermidis was capable of inducing lesions after inoculation and occlusion.58 Biopsy specimens revealed sweat glands blocked with EPS material, further supporting a pathogenic role for biofilms in this condition. Evidence is lacking to support the presence of biofilms in onychomycosis. Nevertheless, several factors including firm adherence of dermatophytes to the nail plate, presence of dormant fungal elements, ability of yeast to form biofilms, and difficulty of eradication all suggest that biofilms may be operative in this condition.59 Conclusion Biofilms are known to be ubiquitous in nature and modern medical technology continues to unveil their role in an evergrowing number of disease processes. In the field of dermatology, biofilms appear to be taking center stage, and their presence likely explains the chronic nature of many cutaneous disorders. 4 It is expected that further knowledge regarding the molecular mechanisms that govern biofilm formation, their virulence, and drug resistance will vastly improve the limited therapeutic options currently available to today’s clinician. References 1. Charles CA, Ricotti CA, Davis SC, et al. Use of tissue-engineered skin to study in vitro biofilm development. Dermatol Surg. 2009 Sep;35(9):1334-41. 2. Davis SC, Ricotti C, Cazzaniga A, et al. Microscopic and physiologic evidence for biofilm-associated wound colonization in vivo. Wound Repair Regen. 2008 Jan-Feb;16(1):23-9. 3. Thomson CH. Biofilms: do they affect wound healing? Int Wound J. 2011 Feb;8(1):63-7. 4. Davis SC, Martinez L, Kirsner R. The diabetic foot: the importance of biofilms and wound bed preparation. Curr Diab Rep. 2006 Dec;6(6):439-45. 5. Nakagami G, Morohoshi T, Ikeda T, et al. Contribution of quorum sensing to the virulence of Pseudomonas aeruginosa in pressure ulcer infection in rats. Wound Repair Regen. 2011 Mar-Apr;19(2):214-22. 6. Wolcott R, Dowd S. The role of biofilms: are we hitting the right target? Plast Reconstr Surg. 2011 Jan;127(Suppl 1):28S-35S. 7. Black CE, Costerton JW. Current concepts regarding the effect of wound microbial ecology and biofilms on wound healing. Surg Clin North Am. 2010 Dec;90(6):1147-60. 8. Martin JM, Zenilman JM, Lazarus GS. Molecular microbiology: new dimensions for cutaneous biology and wound healing. J Invest Dermatol. 2010 Jan;130(1):38-48. 9. Akiyama H, Hamada T, Huh WK, et al. Confocal laser scanning microscopic observation of glycocalyx production by Staphylococcus aureus in skin lesions of bullous impetigo, atopic dermatitis and pemphigus foliaceus. Br J Dermatol. 2003 Mar;148(3):526-32. 10. Donlan RM, Costerton JW. Biofilms: survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev. 2002 Apr;15(2):167-93. 11. Percival SL, Hill KE, Malic S, et al. Antimicrobial tolerance and the significance of persister cells in recalcitrant chronic wound biofilms. Wound Repair Regen. 2011 Jan-Feb;19(1):1-9. 12. Hoiby N, Bjarnsholt T, Givskov M, et al. Antibiotic resistance of bacterial biofilms. Int J Antimicrob Agents. 2010 Apr;35(4):322-32. 13. Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009 Nov-Dec;17(6):763-71. 14. Brem H, Stojadinovic O, Diegelmann RF, et al. Molecular markers in patients with chronic wounds to guide surgical debridement. Mol Med. 2007 Jan-Feb;13(1-2):30-9. 15. Tomic-Canic M, Ayello EA, Stojadinovic O, et al. Using gene transcription patterns (bar coding scans) to guide wound debridement and healing. Adv Skin Wound Care. 2008 Oct;21(10):487-92. 16. James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen. 2008 Jan-Feb;16(1):37-44. 17. Han A, Zenilman JM, Melendez JH, et al. The importance of a multifaceted approach to characterizing the microbial flora of chronic wounds. Wound Repair Regen. 2011 Sep-Oct;19(5):532-41. 18. Kirker KR, Secor PR, James GA, et al. Loss of viability and induction of apoptosis in human keratinocytes exposed to Staphylococcus aureus biofilms in vitro. Wound Repair Regen. 2009 Sep-Oct;17(5):690-9. 19. Schierle CF, De la Garza M, Mustoe TA, et al. Staphylococcal biofilms impair wound healing by delaying reepithelialization in a murine cutaneous wound model. Wound Repair Regen. 2009 May-Jun;17(3):354-9. 20. Fazli M, Bjarnsholt T, Kirketerp-Moller K, et al. Quantitative analysis of the cellular inflammatory response against biofilm bacteria in chronic wounds. Wound Repair Regen. 2011 May-Jun;19(3):387-91. 21. Wolcott RD, Rumbaugh KP, James G, et al. Biofilm maturity studies indicate sharp debridement opens a time- dependent therapeutic window. J Wound Care. 2010 Aug;19(8):320-8. 22. Ammons MC, Ward LS, James GA. Anti-biofilm efficacy of a lactoferrin/xylitol wound hydrogel used in combination with silver wound dressings. Int Wound J. 2011 Jun;8(3):268-73. 23. Krakowski AC, Eichenfield LF, Dohil MA. Management of atopic dermatitis in the pediatric population. Pediatrics. 2008 Oct;122(4):812-24. 24. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003 Jan 11;361(9352):151-60. 25. Ikezawa Z, Komori J, Ikezawa Y, et al. A role of Staphylococcus aureus, interleukin-18, nerve growth factor and semaphorin 3A, an axon guidance • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. molecule, in pathogenesis and treatment of atopic dermatitis. Allergy Asthma Immunol Res. 2010 Oct;2(4):235-46. Akiyama H, Yamasaki O, Tada J, et al. Adherence characteristics and susceptibility to antimicrobial agents of Staphylococcus aureus strains isolated from skin infections and atopic dermatitis. J Dermatol Sci. 2000 Aug;23(3):155-60. Akiyama H, Huh WK, Yamasaki O, et al. Confocal laser scanning microscopic observation of glycocalyx production by Staphylococcus aureus in mouse skin: does S. aureus generally produce a biofilm on damaged skin? Br J Dermatol. 2002 Nov;147(5):879-85. Katsuyama M, Kobayashi Y, Ichikawa H, et al. A novel method to control the balance of skin microflora Part 2. A study to assess the effect of a cream containing farnesol and xylitol on atopic dry skin. J Dermatol Sci. 2005 Jun; 38(3):207-13. Katsuyama M, Ichikawa H, Ogawa S, et al. A novel method to control the balance of skin microflora. Part 1. Attack on biofilm of Staphylococcus aureus without antibiotics. J Dermatol Sci. 2005 Jun;38(3):197-205. White GM. Recent findings in the epidemiologic evidence, classification, and subtypes of acne vulgaris. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S34-7. Coenye T, Honraet K, Rossel B, et al. Biofilms in skin infections: Propionibacterium acnes and acne vulgaris. Infect Disord Drug Targets. 2008 Sep;8(3):156-9. Coenye T, Peeters E, Nelis HJ. Biofilm formation by Propionibacterium acnes is associated with increased resistance to antimicrobial agents and increased production of putative virulence factors. Res Microbiol. 2007 May;158(4): 386-92. Jappe U. Pathological mechanisms of acne with special emphasis on Propionibacterium acnes and related therapy. Acta Derm Venereol. 2003; 83(4):241-8. Gribbon EM, Cunliffe WJ, Holland KT. Interaction of Propionibacterium acnes with skin lipids in vitro. J Gen Microbiol. 1993 Aug;139(8):1745-51. Burkhart CG, Burkhart CN. Expanding the microcomedone theory and acne therapeutics: Propionibacterium acnes biofilm produces biological glue that holds corneocytes together to form plug. J Am Acad Dermatol. 2007 Oct;57(4):722-4. Simonart T, Dramaix M. Treatment of acne with topical antibiotics: lessons from clinical studies. Br J Dermatol. 2005 Aug;153(2):395-403. James KA, Burkhart CN, Morrell DS. Emerging drugs for acne. Expert Opin Emerg Drugs. 2009 Dec;14(4):649-59. Hongcharu W, Taylor CR, Chang Y, et al. Topical ALA-photodynamic therapy for the treatment of acne vulgaris. J Invest Dermatol. 2000 Aug;115(2):183-92. Burkhart CN, Burkhart CG. Microbiology’s principle of biofilms as a major factor in the pathogenesis of acne vulgaris. Int J Dermatol. 2003 Dec;42(12):925-7. Seneviratne CJ, Jin L, Samaranayake LP. Biofilm lifestyle of Candida: a mini review. Oral Dis. 2008 Oct;14(7):582-90. Wolff K, Goldsmith LA, Katz SI, et al. (eds). Fitzpatrick’s dermatology in general medicine. 7th ed. New York: McGraw Hill; 2008. 42. Ganguly S, Mitchell AP. Mucosal biofilms of Candida albicans. Curr Opin Microbiol. 2011 Aug;14(4):380-5. 43. Harriott MM, Lilly EA, Rodriguez TE, et al. Candida albicans forms biofilms on the vaginal mucosa. Microbiology. 2010 Dec;156(Pt 12):3635-44. 44. Dongari-Bagtzoglou A, Kashleva H, Dwivedi P, et al. Characterization of mucosal Candida albicans biofilms. PLoS One. 2009;4(11):e7967. 45. Dwivedi P, Thompson A, Xie Z, et al. Role of Bcr1-activated genes Hwp1 and Hyr1 in Candida albicans oral mucosal biofilms and neutrophil evasion. PLoS One. 2011;6(1):e16218. 46. Nett JE, Marchillo K, Spiegel CA, et al. Development and validation of an in vivo Candida albicans biofilm denture model. Infect Immun. 2010 Sep; 78(9):3650-9. 47. Williams DW, Kuriyama T, Silva S, et al. Candida biofilms and oral candidosis: treatment and prevention. Periodontol 2000. 2011 Feb;55(1):250-65. 48. Hawser SP, Douglas LJ. Resistance of Candida albicans biofilms to antifungal agents in vitro. Antimicrob Agents Chemother. 1995 Sep;39(9):2128-31. 49. LaFleur MD, Kumamoto CA, Lewis K. Candida albicans biofilms produce antifungal-tolerant persister cells. Antimicrob Agents Chemother. 2006 Nov; 50(11):3839-46. 50. Vediyappan G, Rossignol T, d’Enfert C. Interaction of Candida albicans biofilms with antifungals: transcriptional response and binding of antifungals to beta-glucans. Antimicrob Agents Chemother. 2010 May;54(5):2096-111. 51. Kuhn DM, George T, Chandra J, et al. Antifungal susceptibility of Candida biofilms: unique efficacy of amphotericin B lipid formulations and echinocandins. Antimicrob Agents Chemother. 2002 Jun;46(6):1773-80. 52. Traboulsi RS, Mukherjee PK, Chandra J, et al. Gentian violet exhibits activity against biofilms formed by oral Candida isolates obtained from HIV-infected patients. Antimicrob Agents Chemother. 2011 Jun;55(6):3043-5. 53. Tournu H, Van Dijck P. Candida biofilms and the host: models and new concepts for eradication. Int J Microbiol. 2012;2012:845352. 54. Narins RS, Coleman WP, 3rd, Glogau RG. Recommendations and treatment options for nodules and other filler complications. Dermatol Surg. 2009 Oct; 35(Suppl 2):1667-71. 55. Bjarnsholt T, Tolker-Nielsen T, Givskov M, et al. Detection of bacteria by fluorescence in situ hybridization in culture-negative soft tissue filler lesions. Dermatol Surg. 2009 Oct;35(Suppl 2):1620-4. 56. Akiyama H, Morizane S, Yamasaki O, et al. Assessment of Streptococcus pyogenes microcolony formation in infected skin by confocal laser scanning microscopy. J Dermatol Sci. 2003 Sep;32(3):193-9. 57. Yamasaki O, Akiyama H, Toi Y, et al. A combination of roxithromycin and imipenem as an antimicrobial strategy against biofilms formed by Staphylococcus aureus. J Antimicrob Chemother. 2001 Oct;48(4):573-7. 58. Mowad CM, McGinley KJ, Foglia A, et al. The role of extracellular polysaccharide substance produced by Staphylococcus epidermidis in miliaria. J Am Acad Dermatol. 1995 Nov;33(5 Pt 1):729-33. 59. Burkhart CN, Burkhart CG, Gupta AK. Dermatophytoma: recalcitrance to treatment because of existence of fungal biofilm. J Am Acad Dermatol. 2002 Oct;47(4):629-31. Free app available for iPad, iPhone and iPod touch Content & instructions can be found at: http://www.skintherapyletter.com/ipad/about.html http://www.skintherapyletter.com/ipad/support.html • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 5 A Look at Epidermal Barrier Function in Atopic Dermatitis: Physiologic Lipid Replacement and the Role of Ceramides Dušan Sajić, MD, PhD; Rachel Asiniwasis, MD; Sandy Skotnicki-Grant, MD, FRCPC Division of Dermatology, University of Toronto Dermatology, Toronto, ON Bay Dermatology Centre, Toronto, ON ABSTRACT This review summarizes and discusses the role and efficacy of moisturizers, particularly the more recently introduced ceramide-based formulations, in the skin care regimen of patients with both active and quiescent atopic dermatitis (AD). It is now well established that a complex interplay of environmental and genetic factors are responsible for disease onset and chronicity. Indeed, several novel genetic mechanisms have been recently discovered to be associated with AD pathogenesis. Moreover, it is increasingly recognized that the epidermal barrier plays a critical role in the initiation, perpetuation, and exacerbation of AD. The skin of patients with AD harbors several defects in epidermal barrier function, including filaggrin and ceramides. An improved understanding of these etiopathogenic factors has led to the development of topical ceramide-dominant moisturizers to replace the deficient molecules and re-establish the integrity of barrier defenses. Some of these products have demonstrated efficacy in the treatment of adult and childhood AD that are similar to mid-potency topical steroids. More importantly, they have been shown to be safe with very few associated side-effects. We recommend the addition of such new agents as both the first step of treatment and in the maintenance of clinically quiescent skin of patients with AD. Key words: atopic dermatitis, ceramides, eczema, emollients, epidermal barrier, lipids, transepidermal water loss Introduction Atopic dermatitis (AD) is a chronic, inflammatory, pruritic skin disease of increasing prevalence (affecting 15-30% of children and 2-10% of adults).1 AD is considered by many to be the first step in the “atopic march” that can progress to include asthma and allergic rhinitis, as well as be a precursor to, rather than a consequence of, food allergies.1 The precise sequence of biochemical events leading to the development of AD has still not been fully elucidated, but most experts agree that it involves a complex interplay of environmental and genetic factors that induce derangements in the structure and function of the epidermal barrier and immune system. Diagnosis can be challenging, as the variability of clinical presentation can be confounding. Morphology alone cannot reliably confirm the diagnosis and the spectrum of features associated with AD must be considered. While several sets of diagnostic criteria for AD have been proposed and validated, the traditionally used being that of Hanifin and Rajka, full agreement amongst clinicians and uniformity of criteria are still lacking.2 Epidermal Barrier Dysfunction Traditionally, it was thought that the primary pathogenic mechanism of atopic dermatitis was initiated by immune dysfunction leading to a Th2 cytokine imbalance, increased inflammation, and secondary disruption of the epidermal barrier.1,3 However, accumulating evidence suggests that rather than merely having a bystander effect, a primary defect in the stratum corneum plays a major role in driving the pathogenesis of atopic dermatitis that leads to sustained cytokine release, 6 recruitment of pro-inflammatory molecules, and stimulation of a Th2 response.3,4 Moreover, further barrier disruption in the chronic stages of AD, through mechanical scratching, not only perpetuates but alters the response to a mostly Th1 type.5 In addition, while several other cytokines and T cell subsets like IL-31 and Th2,6 respectively, have recently been identified within the skin of patients with AD, the role of the skin barrier influencing their expression remains unclear.7 AD has been separated into two different subtypes, i.e., intrinsic and extrinsic, which were derived on the basis of the extrinsic subtype stemming from allergic sensitization to an external antigen with subsequent allergen specific IgE production, and the intrinsic variant describes patients with all clinical features of AD, but no detectable allergen specific IgE. However, these subtypes may actually represent different stages of evolution based on the relative degree of sensitization. Under this view, AD in infancy is thought to begin as “intrinsic” or non-atopic dermatitis, and over time it progresses to “true” atopy in the majority of cases via allergen exposure through what is now being more widely recognized as a primarily defective epidermal barrier function.1,2 It is well established that the first line of defense within the epidermal barrier is the stratum corneum, which serves several fundamental roles in maintaining protection from the environment as well as preventing water loss. This “outside-in” theory views a primary defect in the stratum corneum as a key condition that drives the inflammatory cascade of AD, predisposing to increased transepidermal water loss (TEWL), penetration of irritants, allergens, secondary infection, and • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 6 increased inflammation.8 Several lines of evidence demonstrate the capacity of the cutaneous barrier to initiate and perpetuate AD including observations that: 1. the defects in the barrier result in elevated pH that activates proteases capable of directly inducing a Th2 inflammatory response,9 2. the severity of the barrier defect parallels AD severity,10,11 3. the barrier defect persists longer than both the clinical lesions and the underlying inflammation,11 4. several genetic disorders with skin lesions similar to AD implicate abnormal gene coding that affect the epidermal barrier, and lastly,12 5. therapeutic strategies aimed at repairing the epidermal barrier, as further discussed below, also ameliorates both the inflammation and the clinically involved skin.13 Morphological Changes in Epidermal Lipids in AD The stratum corneum represents a multicellular vertically stacked layer of cells embedded within a hydrophobic extracellular matrix. This matrix is derived from the secretion of lipid precursors and lipid hydrolases, both of which are secreted from lamellar bodies in the stratum granulosum. These hydrolases cleave the precursors to form essential and non-essential fatty acids, cholesterol, and at least 10 different ceramides, which self-organize into multilayered lamellar bilayers between the corneocytes (“bricks”), resulting in the formation of watertight “mortar”, thus, maintaining skin hydration.12 In physiological balance, the approximate proportions of the lipid component are predominantly composed of 50% ceramides, 25% cholesterol, and 10-20% free fatty acids.8 In atopic dermatitis, there is a decrease in all three key lipids, especially ceramides, which are found in both lesional and non-lesional skin.1 A lipid imbalance and inadequate amounts of ceramides contribute to defective formation of the corneocyte lipid envelope and lipid mortar, which correlates with increased TEWL and enhanced barrier permeability. Filaggrin Mutations and Exogenous Factors in AD Contribute to Epidermal Barrier Dysfunction There has been a large focus on the role of genetic abnormalities leading to defects in key structural components of the epidermal barrier. Perhaps the best example of this is a loss of function mutation in the filaggrin gene, which encodes for the filament aggregating protein (FLG), found in up to 60% of AD patients.12 While there are various other candidate genes that lead to increased susceptibility, including KLK7, SPINK5, and CSTA, FLG remains by far the most prominent.14 Although filaggrin is certainly one of the most important single genes involved in AD susceptibility, inherent redundancy in the epidermal differentiation complex with several other similar genes may mitigate the negative effect of filaggrin mutations and explain the incomplete penetrance in AD. As such, patients carrying a mutation in the FLG gene display a wide spectrum of disease, ranging from mildly dry skin to more severe manifestations of ichthyosis vulgaris.15 Moreover, since only 44% of AD patients carry the heterozygous mutation and 76% of homozygous or compound heterozygous FLG mutation carrying patients suffer from AD,16 this further implicates the role of other genes and the environment in disease pathogenesis. Nevertheless, complete absence of FLG, either as a homozygous mutation or a compound heterozygote mutation, clearly disrupts the epidermal barrier, as all of these patients to date have been shown to present with a clinical picture of ichthyosis vulgaris.17,18 Filaggrin normally assists in cytoskeletal aggregation and formation of the cornified cell envelope (CCE), providing additional strength and structure. It is required for normal lamellar body formation and content secretion. Furthermore, as corneocytes mature and start losing water, FLG dissociates from the CCE and is processed into acidic metabolites acting as osmolytes that help to retain hydration and keep the pH below the threshold required for the activation of Th2-inducing endogenous serine proteases. 9 Therefore, a FLG mutation contributes to a disrupted epidermal barrier, increased water loss, and inflammation. There are also many exogenous factors that can exacerbate barrier dysfunction, specifically soaps and surfactants in detergents that accelerate corneocyte and lipid degradation. Several antigens, including those from cockroaches, Staphylococcus aureus, dust mites, and scabies induce endogenous proteolytic activity, cleaving corneodesmosomal proteins and filaggrin, thus contributing further to the cycle of inflammation and pruritus.1 Lipid Replacement Therapy in AD Traditionally viewed as an immunological disorder, therapies for AD have included topical steroids and immunomodulators, and sometimes more aggressive immunosuppressives that do not target the underlying structural barrier abnormalities.4,19 As well, most conventional moisturizers do not address this underlying lipid deficiency. With an improved understanding of AD etiopathogenesis, a new nonpharmacologic approach has emerged aimed at barrier repair involving the delivery of balanced proportions of stratum corneum specific lipids to assist in correcting this epidermal barrier dysfunction. With accumulating evidence supporting barrier defect-initiated disease pathogenesis and its effects on both triggering and perpetuating AD, it is not surprising that emollients, ointments and oils thought to prevent epidermal water loss and inhibit sensitizing exogenous peptides from traversing the compromised barrier, have become the first-line/adjunctive therapy in patients with AD. While the use of sophisticated moisturizers has been shown to confer protective effects on the skin barrier by delaying onset and decreasing AD severity and flares,1 it is not appropriate to generalize this benefit to all moisturizers, as they not only differ widely in their compositions, but are classified into subcategories based on the therapeutic properties of their key ingredients, e.g., occlusives, humectants, emollients (e.g., intercellular lipids), or some combination of the three. Within the intercellular lipids category, moisturizers contain a variable mix of ceramides, cholesterol, and free fatty acids. One of the most promising barrier repair methods have been ceramide-dominant physiological lipid-based barrier repair topical emulsions. In contrast to traditional moisturizers, these formulations focus on physiologic lipid replacement therapy, particularly ceramides, to restore normal balance of the epidermal barrier. In comparison with other emollients (e.g., petrolatum) that form a more superficial occlusive barrier, ceramide-dominant moisturizers are thought to permeate the stratum corneum and are synthesized in the keratinocytes, processed in lamellar bodies, • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 7 and secreted back into the stratum corneum to become a part of the dermal matrix.8,20 Interestingly, while cholesterol, ceramides, and fatty acids are all required for repair, individually they encumber rather than facilitate barrier recovery.21 Moreover, incomplete mixtures can also result in suboptimal recovery,22 underlining the importance of proper physiological ratios of individual components to achieve maximal efficacy. Ceramide-based emulsions, such as EpiCeram® and TriCeram®, contain the physiological 3:1:1 molar ratio of ceramides, cholesterols, and free fatty acids, which emulates the endogenous composition of the stratum corneum and has been shown to repair its integrity and function.21 While several reports have shown that the 3:1:1 ratio seems to be important in barrier repair,21-24 it appears that the “3” does not necessarily need to be a ceramide, as both three-fold higher ratios of a fatty acid or cholesterol rather than a ceramide can significantly improve barrier function when compared to vehicle alone. 23 Moreover, while both TriCeram® and EpiCeram® contain 2.1% of ceramides, one study showed that a dilution of 1:9 also has significant effects on barrier repair.21 In addition to assisting in restoration of the lipid defect in AD, these products also help to normalize the pH of the skin, which itself is separately associated with a decrease in epidermal barrier integrity, increased inflammation, and reduced antimicrobial defenses.25,26 Although most of the early studies compared the efficacy of the three component mixtures to vehicle alone, several recent reports have shown that some ceramide-dominant formulations can, on their own, induce improvements comparable to topical steroids in the treatment of mild to moderate disease.19,27 Therefore, avoiding associated adverse effects from corticosteroid treatment and certain dosing restrictions, as therapy is suitable for patients of all ages and may be used on sensitive skin sites (e.g., face and intertriginous areas), which are prone to steroid-induced atrophy. Another ceramide-based barrier repair cream is CeraVe™, the first over-the-counter (OTC) product featuring multilamellar vesicular emulsions (MVEs), which are similar to liposomes, but facilitate a slow 24-hour controlled, time-released delivery of the contents. This delivery advance offers once-daily application, thereby encouraging adherence to a simplified regimen of moisturizer use. While no standalone trials have been conducted with MVEs, the combination of MVEs with topical fluocinonide 0.05% has recently been shown to reduce disease duration and time to clearance when compared with the same corticosteroid alone, resulting in accelerated skin barrier recovery.28 Natural vs. Synthetic Ceramides As previously discussed, ceramides are the main components of the multilayered lamellar bilayers between the corneocytes and, thus, a key factor in water retention and overall integrity of the barrier. Chemically, they are amide-linked free fatty acids with long-chain amino alcohol sphingoid bases, which are amidelinked to hydroxylated, x-hydroxylated or nonhydroxylated fatty acids, and shown to also have functions in apoptosis, cell growth, senescence, and cell cycle control.29 Clinically, while many other moisturizers are important in providing short-term relief from dryness in AD, long-term benefits can only be derived through restoring adequate ceramide levels. While replacement with natural ceramides seems to represent the most logical step in the 8 correction of the barrier, there are three important considerations connected with the use of “natural” ceramides. Firstly, there is a high cost associated with nature-identical, synthetic ceramides (e.g., $2,000-$10,000/kg).30 Secondly, inexpensive naturally occurring ceramides are typically extracted from bovine central nervous system, which raises concerns about bovine spongiform encephalopathy (‘mad cow disease’). Thirdly, excess intracellular ceramides can be linked with significant toxicity and lead to cell growth retardation and apoptosis.20,30 Synthetic ceramides are capable of overcoming most of these obstacles and are currently being explored as potential alternatives to natural ceramides. Kang et al. showed that application of 1% K6PC-9p (a synthetic ceramide derivative of PC-9S) resulted in similar improvement of tetradecanoylphorbol acetate (TPA)-induced skin inflammation, when compared to 0.1% hydrocortisone.31 Moreover, application of a ceramide complex (pseudoceramides and eucalyptus leaf extract) resulted in not only improved TEWL and erythema gradings of treated AD patients when compared to vehicle control, but also increased levels of endogenous stratum corneum ceramides.32 Another study investigated a synthetic pseudoceramide and eucalyptus leaf extract formulation in patients with mild to severe AD. 33 This double-blind, within subject vehicle-controlled study of patients with AD lesions on the arms and legs assessed TEWL, global assessment, and erythema. A significant differential benefit for the ceramide complex over vehicle was shown. Additionally, the findings demonstrated that this ceramide complex of pseudoceramides appears to work similar to the endogenous ceramindes found in the skin. Other Non-steroidal Barrier Repair Products While ceramide-based moisturizers clearly appear to be superior to most non-ceramide OTC moisturizers, it should be noted that a recent trial showed the use of a glycyrrhetinic acid-containing barrier repair cream (Atopiclair®) resulted in improvement of mild to moderate AD in children that was equivalent to EpiCeram®.34 Similar findings were seen in another recent study that demonstrated non-superiority of topical pimecrolimus when compared to a number of different OTC creams (collectively regarded as one group),25 suggesting that correction of numerous epidermal barrier derangements may be an effective way of controlling AD. As well, a multicenter, observational, uncontrolled study of 2456 AD patients aged 2-70 years showed that regular use of a barrier cream containing lipids and N-palmitoylethanolamine (MimyX®) significantly reduced AD skin symptoms (e.g., erythema, pruritus, excoriation, scaling, lichenification, and dryness), sleep disturbance, and topical steroid use.35 Eletone® is another FDA-cleared 510(k) prescription medical device moisturizer that helps to improve stratum corneum impairment and restore barrier integrity. The product contains 70% oil dispersed in 30% water, but it uses a proprietary reverse emulsion technology that produces a formulary consistency of a cream with occlusive properties of an ointment, resulting in enhanced cosmetic acceptability. In a study assessing the use of twice-daily Eletone® in 133 pediatric patients with mild to moderate AD, at 4 weeks 54% of patients experienced improvement in pruritus and average body surface area involvement decreased by 43.6%. 36 Whether such treatments lead to an indirect restoration of ceramide levels remains unknown and warrants further investigation. • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 Conclusion AD follows a chronic relapsing course, as such, in addition to pharmacologic intervention, it is essential to maintain hydration and barrier function of the skin with daily regimented moisturizer use. Ceramide-based moisturizers have been shown to be beneficial in reducing TEWL, improving barrier function, and maintaining hydration of the stratum corneum, and thus, can be a useful component in AD management. Adequate moisturization reduces the need for drug treatments, as well as limits the severity and frequency of eczematous flares. Indeed, more studies are showing that correction of the skin barrier defects through emollient therapy inhibits downstream drivers of the inflammatory response, thereby providing the rationale for prophylactic and continuous use. Furthermore, the ceramidebased barrier repair emulsions have an excellent safety profile, without significant adverse events other than occasional transient tingling upon application, and thus, can be safely used in patients of all ages and on sensitive skin regions, including the face and intertriginous areas. Additional research is warranted and will lead to a better understanding of the optimal formulary compositions as well as development of a better treatment ladder for varying severities of AD. Also, long-term studies would be helpful in establishing whether lipid barrier replacement therapy reduces bacterial colonization or prevents progression of the atopic march. References 1. Danby S, Cork MJ. A new understanding of atopic dermatitis: the role of epidermal barrier dysfunction and subclinical inflammation. J Clin Dermatol. 2010;1:33-46. 2. Bos JD, Brenninkmeijer EE, Schram ME, et al. Atopic eczema or atopiform dermatitis. Exp Dermatol. 2010 Apr;19(4):325-31. 3. Elias PM, Schmuth M. Abnormal skin barrier in the etiopathogenesis of atopic dermatitis. Curr Allergy Asthma Rep. 2009 Jul;9(4):265-72. 4. Elias PM. An Appropriate response to the black-box warning: corrective, barrier repair therapy in atopic dermatitis. Clin Med Dermatol. 2009 Feb 9;2:1-3. 5. Matsushima H, Hayashi S, Shimada S. Skin scratching switches immune responses from Th2 to Th1 type in epicutaneously immunized mice. J Dermatol Sci. 2003 Sep;32(3):223-30. 6. Jin H, He R, Oyoshi M, et al. Animal models of atopic dermatitis. J Invest Dermatol. 2009 Jan;129(1):31-40. 7. Szegedi K, Kremer AE, Kezic S, et al. Increased frequencies of IL-31 producing T cells are found in chronic atopic dermatitis skin. Exper Dermatol. 2012 Jun; 21(6):431-6. 8. Sugarman JL. The epidermal barrier in atopic dermatitis. Semin Cutan Med Surg. 2008 Jun;27(2):108-14. 9. Briot A, Deraison C, Lacroix M, et al. Kallikrein 5 induces atopic dermatitis-like lesions through PAR2-mediated thymic stromal lymphopoietin expression in Netherton syndrome. J Exp Med. 2009 May 11;206(5):1135-47. 10. Sugarman JL, Fluhr JW, Fowler AJ, et al. The objective severity assessment of atopic dermatitis score: an objective measure using permeability barrier function and stratum corneum hydration with computer-assisted estimates for extent of disease. Arch Dermatol. 2003 Nov;139(11):1417-22. 11. Seidenari S, Giusti G. Objective assessment of the skin of children affected by atopic dermatitis: a study of pH, capacitance and TEWL in eczematous and clinically uninvolved skin. Acta Derm Venereol. 1995 Nov;75(6):429-33. 12. Elias PM, Wakefield JS. Therapeutic implications of a barrier-based pathogenesis of atopic dermatitis. Clin Rev Allergy Immunol. 2011 Dec; 41(3):282-95. 13. Elias PM, Wood LC, Feingold KR. Epidermal pathogenesis of inflammatory dermatoses. Am J Contact Dermat. 1999 Sep;10(3):119-26. 14. Cork MJ, Danby SG, Vasilopoulos Y, et al. Epidermal barrier dysfunction in atopic dermatitis. J Invest Dermatol. 2009 Aug;129(8):1892-908. 15. Heimall J, Spergel JM. Filaggrin mutations and atopy: consequences for future therapeutics. Expert Rev Clin Immunol. 2012 Feb;8(2):189-97. 16. Palmer CN, Irvine AD, Terron-Kwiatkowski A, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006 Apr;38(4):441-6. 17. Smith FJ, Irvine AD, Terron-Kwiatkowski A, et al. Loss-of-function mutations in the gene encoding filaggrin cause ichthyosis vulgaris. Nat Genet. 2006 Mar;38(3):337-42. 18. Hu Z, Xiong Z, Xu X, et al. Loss-of-function mutations in filaggrin gene associate with psoriasis vulgaris in Chinese population. Hum Genet. 2012 Jul; 131(7):1269-74. 19. Kircik LH, Del Rosso JQ, Aversa D. Evaluating clinical use of a ceramidedominant, physiologic lipid-based topical emulsion for atopic dermatitis. J Clin Aesthet Dermatol. 2011 Mar;4(3):34-40. 20. Anderson PC, Dinulos JG. Are the new moisturizers more effective? Curr Opin Pediatr. 2009 Aug;21(4):486-90. 21. Man MQ, Feingold KR, Elias PM. Exogenous lipids influence permeability barrier recovery in acetone-treated murine skin. Arch Dermatol. 1993 Jun; 129(6):728-38. 22. Man MQ, Brown BE, Wu-Pong S, et al. Exogenous nonphysiologic vs physiologic lipids. Divergent mechanisms for correction of permeability barrier dysfunction. Arch Dermatol. 1995 Jul;131(7):809-16. 23. Man MM, Feingold KR, Thornfeldt CR, et al. Optimization of physiological lipid mixtures for barrier repair. J Invest Dermatol. 1996 May;106(5):1096-101. 24. Yang L, Mao-Qiang M, Taljebini M, et al. Topical stratum corneum lipids accelerate barrier repair after tape stripping, solvent treatment and some but not all types of detergent treatment. Br J Dermatol. 1995 Nov;133(5):679-85. 25. Emer JJ, Frankel A, Sohn A, et al. A bilateral comparison study of pimecrolimus cream 1% and a topical medical device cream in the treatment of patients with atopic dermatitis. J Drugs Dermatol. 2011 Jul;10(7):735-43. 26. Elias PM, Choi EH. Interactions among stratum corneum defensive functions. Exp Dermatol. 2005 Oct;14(10):719-26. 27. Sugarman JL, Parish LC. Efficacy of a lipid-based barrier repair formulation in moderate-to-severe pediatric atopic dermatitis. J Drugs Dermatol. 2009 Dec;8(12):1106-11. 28. Draelos ZD. The effect of ceramide-containing skin care products on eczema resolution duration. Cutis. 2008 Jan;81(1):87-91. 29. Sawai H, Domae N, Okazaki T. Current status and perspectives in ceramidetargeting molecular medicine. Curr Pharm Des. 2005;11(19):2479-87. 30. Uchida Y, Holleran WM, Elias PM. On the effects of topical synthetic pseudoceramides: comparison of possible keratinocyte toxicities provoked by the pseudoceramides, PC104 and BIO391, and natural ceramides. J Dermatol Sci. 2008 Jul;51(1):37-43. 31. Kang JS, Yoon WK, Youm JK, et al. Inhibition of atopic dermatitis-like skin lesions by topical application of a novel ceramide derivative, K6PC-9p, in NC/ Nga mice. Exp Dermatol. 2008 Nov;17(11):958-64. 32. Ishikawa J, Shimotoyodome Y, Chen S, et al. Eucalyptus increases ceramide levels in keratinocytes and improves stratum corneum function. Int J Cosmet Sci. 2012 Feb;34(1):17-22. 33. Ishida K, Takahashi A, Koutatsu B, et al. The ability of ceramide complex to reduce erythema and enhance barrier function of atopic skin. Poster #5433 presented at: American Academy of Dermatology 70th Annual Meeting. San Diego, CA. March 16-20, 2012. 34. Miller DW, Koch SB, Yentzer BA, et al. An over-the-counter moisturizer is as clinically effective as, and more cost-effective than, prescription barrier creams in the treatment of children with mild-to-moderate atopic dermatitis: a randomized, controlled trial. J Drugs Dermatol. 2011 May;10(5):531-7. 35. Eberlein B, Eicke C, Reinhardt HW, et al. Adjuvant treatment of atopic eczema: assessment of an emollient containing N-palmitoylethanolamine (ATOPA study). J Eur Acad Dermatol Venereol. 2008 Jan;22(1):73-82. 36. Abramovits W, Alvarez-Connelly E, Breneman D, et al. A double-blind, randomized, vehicle-controlled trial to determine the efficacy and safety of hydrocortisone butyrate 0.1% lipocream in the treatment of mild to moderate atopic dermatitis in pediatric subjects. Poster presented at: 25th Anniversary Fall Clinical Dermatology Conference. Las Vegas, NV. October 6-9, 2006. • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012 9 Update on Drugs EDITOR-IN-CHIEF Stuart Maddin, MD University of British Columbia, Vancouver, Canada ASSOCIATE EDITORS Hugo Degreef, MD, PhD Catholic University, Leuven, Belgium Jason Rivers, MD University of British Columbia, Vancouver, Canada EDITORIAL ADVISORY BOARD Murad Alam, MD Northwestern University Medical School, Chicago, USA Kenneth A. Arndt, MD Beth Israel Hospital Harvard Medical School, Boston, USA Wilma Fowler Bergfeld, MD Cleveland Clinic, Cleveland, USA Jan D. Bos, MD University of Amsterdam, Amsterdam, Holland Alastair Carruthers, MD University of British Columbia, Vancouver, Canada Bryce Cowan, MD, PhD University of British Columbia, Vancouver, Canada Jeffrey S. Dover, MD Yale University School of Medicine, New Haven, USA Dartmouth Medical School, Hanover, USA Boni E. Elewski, MD University of Alabama, Birmingham, USA Barbara A. Gilchrest, MD Boston University School of Medicine, Boston, USA Christopher E.M. Griffiths, MD University of Manchester, Manchester, UK Aditya K. Gupta, MD, PhD University of Toronto, Toronto, Canada Mark Lebwohl, MD Mt. Sinai Medical Center, New York, USA James J. Leydon, MD University of Pennsylvania, Philadelphia, USA Name/Company CIP-Isotretinoin The US FDA has approved this novel formulation of isotretinoin Absorica™ in May 2012 for the treatment of severe recalcitrant nodular Cipher Pharmaceuticals acne. According to the manufacturer, CIP-isotretinoin is based on the patented oral Lidose® drug delivery system, which offers precise, consistent, and uniform dosage delivery with an absorption characteristic that is stable with or without food when compared with traditional generic isotretinoin. A major challenge for existing isotretinoin products is patient adherence, as the active ingredient should be taken with a high-fat meal to ensure consistent absorption. Currently available generic isotretinoin products have an estimated 65% variability in absorption depending on dietary intake, resulting in inconsistent dosing and pharmacokinetic implications, which is of particular concern in teenaged patients. Hence, CIP-istotretinoin was designed to maintain steady drug absorption throughout the typical 3- to 5-month course of treatment. Product launch in the US is expected in Q4 2012 and it is currently under Health Canada review. Tazarotene 0.1% foam Fabior™ Stiefel Laboratories FDA approval was granted to a novel retinoid formulation in May 2012 for the topical treatment of acne vulgaris. Therapy is indicated for acne patients ≥12 years of age. The approval of tazarotene foam was based on two multicenter, randomized, double-blind, vehicle-controlled pivotal Phase 3 studies. The most common side-effects were application site reactions, such as irritation, dryness, erythema, and exfoliation. Butoconazole nitrate 2% vaginal cream Perrigo Company The FDA approved an abbreviated new drug application for this antifungal agent in May 2012, which is indicated for the local treatment of vulvovaginal candidiasis (infections cause by Candida). It is the generic equivalent of innovator brand Gynazole-1® (KV Pharmaceuticals). Andrew N. Lin, MD University of Alberta, Edmonton, Canada Harvey Lui, MD University of British Columbia, Vancouver, Canada Howard I. Maibach, MD University of California Hospital, San Francisco, USA Jose Mascaro, MD, MS University of Barcelona, Barcelona, Spain Larry E. Millikan, MD Tulane University Medical Center, New Orleans, USA Jean Paul Ortonne, MD Centre Hospitalier Universitaire de Nice, Nice, France Jaggi Rao, MD University of Alberta, Edmonton, Canada Ted Rosen, MD Device News Baylor College of Medicine, Houston, USA Alan R. Shalita, MD SUNY Health Sciences Center, Brooklyn, USA Wolfram Sterry, MD Humboldt University, Berlin, Germany Richard Thomas, MD University of British Columbia, Vancouver, Canada Stephen K. Tyring, MD, PhD University of Texas Health Science Center, Houston, USA John Voorhees, MD University of Michigan, Ann Arbor, USA Multisource radiofrequency aesthetic device Glow by EndyMed™ EndyMed Medical Ltd Eclipse Aesthetics The FDA cleared this aesthetic device in May 2012 for the reduction of mild to moderate facial wrinkles and fractional radiofrequency (RF) skin resurfacing. Two versions are available: one with a non-ablative multisource RF dermal heating handpiece and the other with a multisource fractional RF skin resurfacing (FSR) handpiece. This system utilizes 3DEEP™ technology, a multisource, phase-controlled RF energy source and advanced software to control the phase of the energy flowing between the handpiece electrodes. Low-level laser for circumferential upper arm reduction Zerona® Erchonia Medical The FDA granted 510(k) clearance to market this bodycontouring laser treatment in June 2012 for the non-invasive reduction of arm circumference by emitting low-level (or cold) output energy that does not generate a thermal effect on body tissues. The device is a monochromactic semiconductor diode laser that emits 5 independent 635 nm divergent beams. A blinded and controlled clinical study showed that Zerona® laser demonstrated a statistically significant difference in circumference reduction, which was sustained 7.6 months post-treatment, as compared with a placebo laser. Subjects who received Zerona® laser therapy experienced approximately 4 cm reduction in the circumference of their arms without dieting, exercising or nutritional supplementation. Guy Webster, MD Jefferson Medical College, Philadelphia, USA Klaus Wolff, MD University of Vienna, Vienna, Austria Skin Therapy Letter © (ISSN 1201–5989) Copyright 2012 by SkinCareGuide.com Ltd. Skin Therapy Letter © is published 10 times annually by SkinCareGuide.com Ltd, 1004 – 750 West Pender, Vancouver, British Columbia, Canada, V6C 2T8. All rights reserved. Reproduction in whole or in part by any process is strictly forbidden without prior consent of the publisher in writing. While every effort is made to see that no inaccurate or misleading data, opinion, or statement appears in the Skin Therapy Letter ©, the Publishers and Editorial Board wish to make it clear that the data and opinions appearing in the articles herein are the responsibility of the contributor. Accordingly, the Publishers, the Editorial Committee and their respective employees, officers, and agents accept no liability whatsoever for the consequences of any such inaccurate or misleading data, opinion, or statement. While every effort is made to ensure that drug doses and other quantities are presented accurately, readers are advised that new methods and techniques involving drug usage, and described herein, should only be followed in conjunction with the drug manufacturer’s own published literature. Printed on acid-free paper effective with Volume 1, Issue 1, 1995. Subscription Information. Annual subscription: Canadian $94 individual; $171 institutional (plus GST); US $66 individual; $121 institutional. Outside North America: US$88 individual; $143 institutional. We sell reprints in bulk (100 copies or more of the same article). For individual reprints, we sell photocopies of the articles. The cost is $20 to fax and $15 to mail. Prepayment is required. Student rates available upon request. For inquiries: [email protected] 10 Approval Dates/Comments • Editor: Dr. Stuart Maddin • Volume 17, Number 7 • July-August 2012