Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
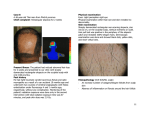
Clinical review Cicatricial (scarring) alopecia: an overview and a clinical approach to diagnosis Yi Zhen Chiang, Firas Al-Niaimi Scarring alopecia, also known as cicatricial alopecia, forms an important group of disorders whereby there is irreversible damage to hair follicles resulting in scarring and permanent hair loss. The hair follicles can be destroyed directly by a primary process (primary cicatricial alopecia) or secondary to an underlying disease or an external agent (secondary cicatricial alopecia). A diagnosis of scarring alopecia can be achieved on both clinical and histological grounds. Patients with cicatricial alopecia often have significant psychosocial impact and dermatology nurses can play an important role in the care for these patients. Introduction Scalp hair is an important component of identity, body image and self-esteem, and is often used to express personality and sexuality. It is therefore not surprising that alopecia (hair loss) can lead to significant psychosocial distress, psychiatric disorders, marital problems and career-related problems (Hunt, 2005). Alopecia can be cicatricial (scarring) or non-cicatricial (non-scarring).This review will focus on cicatricial alopecia with an aim to providing a systematic approach to the assessment of patients with suspected cicatricial alopecia and an overview of the different types of cicatricial alopecia. Cicatricial alopecia forms a rare, but important group of disorders characterised by permanent destruction of hair follicles, resulting in scarring and permanent hair loss. The hair follicle can be destroyed by a primary process aimed directly at the hair follicle (primary cicatricial alopecia (PCA)), or secondary to a generalised destructive process within the skin, which ultimately destroys the hair follicle’s capacity for regeneration (secondary cicatricial alopecia) (Harries, 2009). pathogenesis of primary cicatricial alopecias is not known, but is likely to result from an irreversible damage to the epithelial hair follicle stem cells that reside in the hair follicle ‘bulge’. This is suggested by the pattern of inflammation seen in cicatricial alopecia, which is around the ‘bulge’, as opposed to non-cicatricial alopecia, which is around the hair bulb (Harries, 2009). Secondary cicatricial alopecia develops as a result of an underlying process or an external agent. Potential causes are inflammatory/autoimmune diseases (eg, scleroderma, sarcoidosis), infections (eg, tinea capitis), neoplastic processes (eg, primary skin cancer, metastatic carcinoma), and physical agents (eg, ionising radiation, thermal burn) (Headington, 1996). Classification The North American Hair Research Society (NAHRS) has produced a working classification of primary cicatricial alopecia. The classification is based primarily on the predominant inflammatory infiltrate found on scalp biopsy, as shown in Table 1 (Olsen, 2003). Clinical assessment Patients with cicatricial alopecia often present fairly late due to the subtle, relentless progression of the disease. Diagnosis can be challenging due to the evolving clinical and histological features over time, and the overlapping clinical and histological features seen in one condition with the other (Harries, 2009). Nevertheless, a systematic approach to establish an accurate diagnosis is a vital first step in successful management. History Patients with cicatricial alopecia may present with an acute or gradual onset of hair loss and symptoms. Common symptoms include pain, irritation, itching and discharge. A full history should include the patient’s ethnic origin and age as some Table 1. The North American Hair Research Society classification of primary cicatricial alopecias (Olsen EA, 2001). The epidemiology of PCA has been reported to range from 3.2% to 7.3% (Whiting, 2001, Tan, 2004). The exact Inflammatory infiltrate Diagnosis Lymphocytic Lichen plano pilaris and variants; chronic cutaneous lupus erythematosus; pseudopelade of Brocq; central centrifugal cicatricial alopecia Yi Zhen Chiang is a Specialty Trainee in Dermatology at Birmingham City Hospital. Firas Al-Niaimi is a Fellow in Mohs Surgery and Laser, St John’s Institute of Dermatology, London Neutrophilic Folliculitis decalvans/Tufted folliculitis; dissecting cellulitis of the scalp Mixed Non-specific Folliculitis acne keloidalis End stage of scarring 32 Dermatological Nursing, 2012, Vol 11, No 4 32-34_Scarring alopecia.mjjpC2.indd 34 www.bdng.org.uk 04/12/2012 10:18 Figure 1. Lichen planopilaris (LPP). Figure 2. Pseudopelade of Brocq (PB). conditions appear more commonly in certain racial groups and age (Han, 2006). A complete and focused history should aim to elicit the following points: 8 Ethnic origin 8 Age 8 Onset 8 Progression 8 Local and systemic symptoms 8 Other medical problems (eg, presence of autoimmune diseases or associated inflammatory skin conditions such as lupus erythematosus (LE), lichen planus (LP), infections, malignancies) 8 Previous treatment (including any previous exposure to thermal burns, radiation treatment) 8 Previous hair care practice (eg, use of hot combs, excess traction) Examination A crucial first step in clinical examination is to confirm the presence of scarring on the areas of hair loss, which is characterised by the loss of follicular ostia (openings). Additional clues to scarring are epidermal atrophy, irregularly spaced hair shafts and hair tufting (multiple hairs emerging from a single follicular ostium) (Han, 2006). A good light, aided by a magnifying lens or dermatoscope, is essential in the examination of the scalp. Scalp inflammation often indicates active disease, and the signs of an active disease include erythema, scaling, crusting, pustules, scalp bogginess, and a positive pull test with anagen bulbs seen on the hair mount (Harries, 2009, Han, 2006). The following features should be recorded: 8 Pattern of hair loss and extent of scalp involvement 8 Presence or absence of scarring 8 Associated skin changes on the scalp (eg, erythema, scaling, atrophy, change www.bdng.org.uk 32-34_Scarring alopecia.mjjpC2.indd 35 GALDERMA/DermQuest.com GALDERMA/DermQuest.com GALDERMA/DermQuest.com GALDERMA/DermQuest.com Clinical review Figure 3. Dissecting cellulitis of the scalp (DCS). in pigmentation, scalp bogginess, pustules, crusting) 8 Other area(s) of hair loss 8 Signs of skin disease elsewhere (eg, lichen planus, lupus erythematosus). Investigations Samples for microscopy, culture and sensitivity (bacterial and fungal) are useful if there are signs of infection such as crusting, scaling, pustules or scalp bogginess. Pustules, however, are not always associated with infections, and can be seen in normal scalps (Harries, 2009). A scalp biopsy is often essential in the assessment of cicatricial alopecia. It will help to confirm scarring (if there is any clinical doubt), and to identify the secondary cause of cicatricial alopecia, or to confirm the diagnosis of a primary cicatricial alopecia based on the predominant inflammatory infiltrate involved (as shown in Table 1). Diagnosis The major forms of primary cicatricial alopecia are lichen planopilaris (LPP) (Figure 1) and variants — frontal fibrosing alopecia (FFA) and Graham-Little syndrome (GLS); chronic cutaneous lupus erythematosus (CCLE); pseudopelade of Brocq (PB) (Figure 2); central centrifugal cicatricial alopecia (CCCA); folliculitis decalvans (FD); dissecting cellulitis of the scalp (DCS) (Figure 3); tufted folliculitis (TF); and acne keloidalis nuchae (AKN) (Figure 4) (Ross, 2005). Lichen planopilaris and variants LPP is characterised by multiple patches of permanent alopecia distributed over the central scalp, mostly affecting middle-aged women. Mild to moderate itching has been reported. Scaling and erythema around the follicles in the expanding areas of alopecia are commonly seen (Ross, 2005). Figure 4. Acne keloidalis nuchae (AKN). FFP is a variant of LPP and presents typically with a band-like symmetrical recession of the frontal hairline.The condition is common in post-menopausal women. GLS is another variant of LPP and is characterised by the triad of patchy, progressive scarring alopecia, non-scarring alopecia of axillary and pubic hair, and widespread horny follicular papules (keratosis pilaris) on trunk and limbs (Ghislain, 2006). Chronic cutaneous lupus erythematosus A third of the cases of CCLE have scarring alopecia.This condition is more common in adult women. It commonly affects the central scalp with associated skin changes such as erythema, scaling, follicular plugging, change in pigmentation, and skin atrophy (Annessi, 1999, Harries 2009). In contrast, diffuse and non-scarring hair loss is frequently observed in systemic lupus erythematosus (Cardinali, 2000). Pseudopelade of Brocq It is still not clear whether PB is a disease in its own right or just the end stage of a different scarring process. However, it has a characteristic clinical picture.Typically, there are multiple, variably sized, white to skincoloured plaques on the vertex (known as ‘footprints in the snow’), and they are largely asymptomatic (Braun-Falco, 1986, Dawber, 1992). Central centrifugal cicatricial alopecia CCCA is often seen in women of African descent and has been referred to as ‘follicular degeneration syndrome’ or ‘hot comb alopecia’ (Sperling, 1992).The disorder commonly starts over the vertex and spreads symmetrically and centrifugally. The hair loss is often incomplete with groups of hairs remaining in the area of scarring. Symptoms are usually absent and there is no clinical evidence of inflammation (Harries, 2009). Dermatological Nursing, 2012, Vol 11, No 4 33 04/12/2012 10:18 Clinical review Folliculitis decalvans, tufted folliculitis, dissecting cellulitis of the scalp and acne keloidalis nuchae These conditions form a group of scarring alopecia that present with discharging material.They affect men and women from young adulthood to middle-age.The vertex is most commonly affected.The scarred areas are often hypertrophic with features of pustules, crusting and tufts.TF is often thought to be a variant of FD. DCS is seen almost exclusively in males of African descent.There are typically multiple painful interconnecting scalp nodules, fluctuant nodules which may discharge purulent material, and the presence of sinus tracts (Brooke, 2001). AKN commonly involves the occipital scalp. Like DCS, AKN tends to affect young men of African descent. Keloid plaques are seen, with secondary infection suggested by the presence of pustule formation, pain and discharge (Sperling, 2000, Dinehart, 1989). Management Management of cicatricial alopecia is challenging as hair regrowth in scarred areas hardly ever occurs.The principle aim of treatment is to reduce symptoms and to stop or slow progression of the scarring process. It is important to ensure that patients understand the aims of their treatment and are provided with a realistic expectation. As a general rule, immunosuppressants such as potent topical corticosteroids, intralesional triamcinolone acetate, oral corticosteroids, and antimalarials (eg, hydroxychloroquine) are useful for the lymphocyte-predominant sub-group of primary cicatricial alopecia; while antimicrobials (eg, tetracyclines) and dapsone are useful for the neutrophilpredominant sub-group. Patients with completely stable or ‘burned-out’ cicatricial alopecia may benefit from scalp reduction surgery and, possibly, hair transplantation (Harries, 2008). Damaging hair care practice such as tight hair braiding, use of chemical relaxers, glued-in or sewnin hair weaves should be stopped.The underlying cause of a secondary cicatricial alopecia should be identified and treated accordingly. As hair loss is associated with significant psychosocial morbidity, 34 management of these patients should also include addressing their psychosocial aspects. Patients can be referred to a psychologist for counselling and ways to deal with the psychological impact of hair loss if needed. Regular monitoring of disease progression and adequate provision of information can help relieve unnecessary anxiety. Dermatology nurses who care for these patients can play a role in providing continuous support, information on scalp and hair care practice, techniques of scalp coverage and camouflage, and to ensure that these patients have a good understanding about the nature and treatment of their condition. Useful information on cicatricial alopecia can be obtained from the British Association of Dermatologists (BAD) website and various patient support groups (Table 2) (Hunt, 2005). Conclusion Cicatricial alopecia forms an important group of disorders that result in scarring and permanent hair loss. An early diagnosis can be achieved by a systematic approach to the clinical assessment. Patients with cicatricial alopecia often have significant psychosocial impact and management of these patients should address both their physical and psychological aspects. DN References Annessi G, Lombardo G, Gobello T, Puddu P (1999) A clinicopathologic study of scarring alopecia due to lichen planus: comparison with scarring alopecia in discoid lupus erythematosus and pseudopelade. Am J Dermatopathol 21: 324-31 Braun-Falco O, Imai S, Schmoeckel C, Steger O, Bergner T (1986) Pseudopelade of Brocq. Dermatologica 172(1): 18-23 Brooke RC, Griffiths CE (2001) Folliculitis decalvans. Clin Exp Dermatol 26(1): 120-12 Cardinali C, Caproni M, Bernacchi E, Amato L, Fabbri P (2000) The spectrum of cutaneous manifestations in lupus erythematosus—the Italian experience. Lupus 9(6): 417-423 Alopecia UK Online www.alopeciaonline.org.uk Alopecia Help and Advice (Scotland) www.alopeciascotland.co.uk Bebold Alopecia Awareness www.bebold.org.uk Changing Faces www.changingfaces.org.uk Cicaticial Alopecia Research Foundation www.carfintl.org Hair Foundation www.hairfoundation.org Hairline International www.hairlineinternational.com Hunt N, McHale S (2004) Coping with alopecia. London: Sheldon Press, Top 50 Blogs for Understanding and Coping with Alopecia http://msndegree.com/top-50-blogs-forunderstanding-coping-with-alopecia Ghislain PD, van Eeckhout P, Ghislain E (2006) Graham-Little-Piccardi-Lasseur syndrome: a 20year follow-up. Dermatology 206: 391-2 Han A, Mirmirani P (2006) Clinical approach to the patient with alopecia. Semin Cutan Med Surg 25(1): 11-23 Harries MJ, Sinclair RD, MacDonald-Hull S, et al (2008) Management of primary cicatricial alopecias: options for treatment. Br J Dermatol 159(1): 1-22 Harries MJ, Trueb RM, Tosti A, et al (2009) How not to get scar(r)ed: pointers to the correct diagnosis in patients with suspected primary cicatricial alopecia. Br J Dermatol 160(3): 482-501 Headington JT (1996) Cicatricial alopecia. Dermatol Clin 14(4): 773-82 Hunt N, McHale S (2005) The psychological impact of alopecia. BMJ 331: 951-3 Ross EK, Tan E, Shapiro J (2005) Update on primary cicatricial alopecias. J Am Acad Dermatol 53(1): 1-37 Sperling LC, Sau P (1992) The follicular degeneration syndrome in black patients. ‘Hot comb alopecia’ revisited and revised. Arch Dermatol 128(1): 68-74 Sperling LC, Homoky C, Pratt L, Sau P (2000) Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol 136(4): 479-84 Dawber R (1992) What is pseudopelade? Clin Exp Dermatol 17(5): 305-6 Olsen EA, Bergfeld WF, Cotsarelis G, et al (2003) Summary of North American Hair Research Society (NAHRS)-sponsored workshop on cicatricial alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol 48(1): 103-10 Dinehart SM, Tanner L, Mallory SB, Herzberg AJ (1989) Acne keloidalis in women. Cutis 44(3): 250-2 Tan E, Martinka M, Ball N, et al (2004) Primary cicatricial alopecias: clinicopathology of 112 cases. J Am Acad Dermatol 50(1): 25-32 de Berker D, Dissaneyeka M, Burge S (1992) The sequelae of chronic cutaneous lupus erythematosus. Lupus 1(3): 181-6 Whiting DA (2001) Cicatricial alopecia: clinicopathological findings and treatment. Clin Dermatol 19(2): 211-25 Dermatological Nursing, 2012, Vol 11, No 4 32-34_Scarring alopecia.mjjpC2.indd 36 Table 2. Useful resources for patients and healthcare professionals. www.bdng.org.uk 04/12/2012 10:18