Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
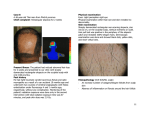
950 Clinical Dermatology Scarring Alopecia BOX 24-13 Primary Scarring Alopecia (Classification based on clinical presentation and histology) Initially lymphocytic • Chronic cutaneous lupus erythematosus • Lichen planopilaris (LPP) • Classic lichen planopilaris • Frontal fibrosing alopecia • Lassueur-Graham-Little syndrome (LPP and lichen planus and spinous lesions) • Pseudopelade (Brocq) • Central centrifugal cicatricial alopecia (follicular degeneration syndrome, hot comb alopecia) Neutrophilic • Folliculitis decalvans • Dissecting cellulitis/folliculitis Mixed • Acne keloid • Tufted folliculitis • Acne necrotica • Erosive pustular dermatosis Adapted from Whiting DA: Clin Dermatol 19(2):211-225, 2001. PMID: 11397600 BOX 24-14 Secondary Scarring Alopecia Inherited and congenital disorders Aplasia cutis, chondrodysplasia punctata, cutis verticis gyrata, Darier’s disease, eccrine hamartoma, epidermal nevi, epidermolysis bullosa, hair-follicle hamartoma, hypotrichosis congenita, ichthyosis (sex-linked recessive), incontinentia pigmenti, keratosis pilaris spinulosa decalvans, neurofibromatosis, polyostotic fibrous dysplasia, porokeratosis of Mibelli, scarring follicular keratosis Physical/chemical agents Chemical burns, insect bites, mechanical trauma or laceration, radiation dermatitis, thermal burns Sclerosing disorders Lichen sclerosus et atrophicus, morphea, scleroderma, scleroderma en coup de sabre and facial hemiatrophy, sclerodermoid porphyria cutanea tarda Dermal granulomatous infiltrations Actinic granuloma; amyloidosis; infections caused by fungi, protozoa, syphilis, tuberculosis, viruses, etc.; Miescher’s granuloma; necrobiosis lipoidica; sarcoidosis Dermal neoplastic infiltrations Adnexal tumors, basal cell carcinoma, dematofibrosarcoma protuberans, lymphoma, melanoma, metastatic carcinoma, squamous cell carcinoma, etc. Adapted from Whiting DA: Clin Dermatol 19(2):211-225, 2001. PMID: 11397600 The classification of scarring alopecia is confusing. The cicatricial or scarring alopecias cause destruction of follicles and result in irreversible hair loss. They occur with either destruction of the follicle or scarring of the reticular dermis. Scarring alopecias are classified as primary or secondary. In primary scarring alopecias (Box 24-13), the follicle is the target of inflammation. In secondary scarring alopecias (Box 24-14), the follicle is destroyed by a nonfollicular process. In primary scarring alopecias, the inflammation is either primarily lymphocytic or neutrophilic. All parts of the follicle can be involved, but the bulge area of the follicle, where the arrector pili muscles insert, is the primary target of the inflammatory process. This bulge contains the stem cells for regeneration of the lower follicle during normal follicular cycling. The end stage is smooth skin with no follicular orifices. The primary cause may be related to sebaceous glands. Central Centrifugal Scarring Alopecia (Follicular Degeneration Syndrome). Central centrifugal cicatricial alopecia (CCCA) (previously known as hot comb alopecia, follicular degeneration syndrome) can result in the permanent destruction of hair follicles. It is the most common form of cicatricial hair loss among black women. The ideology is unknown. Hair styles causing traction and inflammation from bacterial infection may be contributing factors. The increase in diabetes mellitus type 2 among those with CCCA supports the theory that cicatricial alopecia may be a manifestation of metabolic dysregulation. CCCA presents on the vertex of the scalp and can be divided into early (inflammatory) and late (scarring) stages (Box 24-15). Erythema and scaling indicate the presence of inflammation around hair follicles. Pruritus and scalp tenderness are common. Early in the disease process, there is decreased hair density in an area measuring a few centimeters. The disease progresses slowly. Histologically there are varying levels of inflammation, BOX 24-15 Central Centrifugal Scarring Alopecia (Follicular Degeneration Syndrome, Hot Comb Alopecia) • Middle-aged black females, some black males • Some have history of hot comb usage • Scarring alopecia starts on the vertex, spreads forwards and outwards and gradually assumes the central, elongated configuration of female pattern alopecia; most active disease at the periphery; eventual burnout • Lymphocytic inflammation • Premature disintegration of the inner root sheath • Release of hair fragments into the dermis, causing granulomatous inflammation • Differential diagnosis—discoid lupus erythematosus, lichen planopilaris, folliculitis decalvans, pseudopelade, tufted folliculitis • Treatment—minimal hair grooming; no oily scalp preparations, traction, heat, chemicals, straighteners, perming, or dyeing; treat with topical or intralesional steroids, topical minoxidil www.PTools.ir