Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
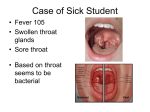
Clinical Policy Title: Molecular tests for group A streptococcus Clinical Policy Number: 18.01.04 Effective Date: Initial Review Date: Most Recent Review Date: Next Review Date: July 1, 2016 February 17, 2016 March 16, 2016 March, 2017 Policy contains: Group A streptococcus Molecular test Related policies: None. ABOUT THIS POLICY: AmeriHealth Caritas Pennsylvania has developed clinical policies to assist with making coverage determinations. AmeriHealth Caritas Pennsylvania’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by AmeriHealth Caritas Pennsylvania when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. AmeriHealth Caritas Pennsylvania’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. AmeriHealth Caritas Pennsylvania’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, AmeriHealth Caritas Pennsylvania will update its clinical policies as necessary. AmeriHealth Caritas Pennsylvania’s clinical policies are not guarantees of payment. Coverage policy AmeriHealth Caritas Pennsylvania considers the use of molecular testing for group A streptococcus (GAS) to be investigational and, therefore, not medically necessary. Limitations: All other uses of molecular testing for GAS are not medically necessary. Note: The following CPT/HCPCS code is not listed in the Pennsylvania Medicaid fee schedule: 87651 - Illumigene for Group A Streptococcus Alternative covered services: Rapid strep and throat culture 1 Background Approximately 9,000-11,500 cases of invasive disease (3.2 to 3.9/100,000 populations) occur each year in the United States; STSS and NF each accounted for approximately 6%-7% of cases. Over 10 million noninvasive GAS infections (primarily throat and superficial skin infections) occur annually. Acute pharyngitis, otherwise known as sore throat, results in 15 million primary care consultations each year in the US, with up to 30 percent of pediatric cases caused by Group A Streptococcus. GAS is the most common bacterial cause of acute pharyngitis, responsible for 5%–15% of sore throat visits in adults and 20%–30% in children. Group A Streptococcus (Group A Strep, or GAS) bacteria spread through contact with droplets from an infected person's cough or sneeze, and live in a person's nose and throat. Most GAS infections cause relatively mild (noninvasive) illnesses such as strep throat, scarlet fever, and impetigo (a skin infection). More than 10 million non-invasive GAS infections (primarily throat and superficial skin infections) occur annually in the U.S. Occasionally, these bacteria can cause severe and even life-threatening (invasive) diseases. Cases of invasive GAS infections, such as necrotizing fasciitis and streptococcal toxic shock syndrome, occur less frequently but are associated with higher rates of deaths. Acute GAS pharyngitis has certain characteristic epidemiological and clinical features .The disorder is primarily a disease of children 5–15 years of age, and, in temperate climates, it usually occurs in the winter and early spring. Patients with GAS pharyngitis commonly present with sore throat (generally of sudden onset), pain on swallowing, and fever. Headache, nausea, vomiting, and abdominal pain may also be present, especially in children. On examination, patients have tonsillopharyngeal erythema, with or without exudates, often with tender, enlarged anterior cervical lymph nodes (lymphadenitis). Other findings may include a beefy, red, swollen uvula; petechiae on the palate; excoriated nares (especially in infants); and a scarlatiniform rash. However, none of these findings are specific for GAS pharyngitis. Conversely, the absence of fever or the presence of clinical features such as conjunctivitis, cough, hoarseness, coryza, anterior stomatitis, discrete intra-oral ulcerative lesions, viral exanthema, and diarrhea strongly suggest a viral rather than a streptococcal etiology. In addition to high sensitivity and specificity, a significant advantage to molecular methods is their potential utility as rapid diagnostic tests. Results are available within 1 h of setup, enabling physicians to initiate appropriate treatment promptly. Alternatively, since tests can be batched easily, testing can be performed several times a day in laboratories with high throughput. Testing can potentially be coupled with a method of automated physician notification, as described by Uhl et al. This strategy would offer results with more rapidity than the standard 48-hr. culture. Rheumatic fever (RF) is an autoimmune disease which affects more than 20 million children in developing countries. It is triggered by Streptococcus pyogenes throat infection in untreated susceptible individuals. Carditis, the most serious manifestation of the disease, leads to severe and permanent valvular lesions, causing chronic rheumatic heart disease (RHD). We have been studying the mechanisms leading to pathological autoimmunity in RF/RHD for the last 15 years. Studies allowed a better understanding of the cellular and molecular pathogenesis of RHD, paving the way for the development of a safe vaccine for a post-infection autoimmune disease. We have focused on the search for protective T and B cell epitopes by testing 620 human blood samples against 2 overlapping peptides spanning 99 residues of the C-terminal portion of the M protein, differing by one amino acid residue. We identified T and B cell epitopes with 22 and 25 amino acid residues, respectively. Although these epitopes were from different regions of the C-terminal portion of the M protein, they showed an identical core of 16 amino acid residues. Antibodies against the B cell epitope inhibited bacterial invasion/adhesion in vitro. Our results strongly indicated that the selected T and B cell epitopes could potentially be protective against S. pyogenes. PMCID: PMC2270766 PMID: 17162355 [PubMed indexed for MEDLINE]. US Food and Drug Administration clearance Roche Diagnostics for its cobas Strep A test for detecting group A streptococcus bacterial DNA in throat swab specimens. According to Roche, The test runs on Roche's cobas Liat System, a molecular point-of-care diagnostic system scheduled for launch later this year. The PCR-based test can detect Strep A DNA in 15 minutes when run on the Liat system. Alere Inc. (NYSE: ALR), a global leader in rapid diagnostic tests, today announced that its Alere™ i Strep A test has received marketing clearance from the U.S. Food and Drug Administration (FDA). Alere i Strep A is the first molecular test that detects Group A Streptococcus (GAS) bacteria in throat swab specimens in 8 minutes or less. Other companies offering nucleic acid amplification tests for strep include Focus Diagnostics, Meridian Bioscience, and Quidel, while firms like Hibergene and Tetracore have assays in development. Cultures of a throat swab on a sheep blood agar plate has been the standard for the documentation of the presence of GAS pharyngitis in the upper respiratory tract and for the confirmation of the clinical diagnosis of acute streptococcal pharyngitis If performed correctly, culture of a single throat swab on a blood agar plate is 90%– 95% sensitive for detection of GAS pharyngitis. The clinical significance of the number of GAS colonies on the throat culture plate is problematic. Although patients with true acute GAS pharyngitis are likely to have more strongly positive cultures than patients who are streptococcal carriers (i.e., individuals with chronic GAS colonization of the pharynx), there is too much overlap in this regard to permit accurate differentiation on this basis alone rapid antigen detection test (RADTs). A major disadvantage of throat cultures is the delay (overnight or longer) in obtaining results. RADTs have been developed for the identification of GAS pharyngitis directly from throat swabs, with shorter turnaround time. Rapid identification and treatment of patients with GAS pharyngitis can reduce the risk of spread, allowing the patient to return to school or work sooner, and can reduce the acute associated morbidity. Diagnosis of GAS Pharyngitis should be established by: 1. Swabbing the throat and testing for GAS pharyngitis by rapid antigen detection test (RADT) and/or culture should be performed because the clinical features alone do not reliably discriminate between GAS and viral pharyngitis except when overt viral features like rhinorrhea, cough, oral ulcers, and/or hoarseness are present. In children and adolescents, negative RADT tests should be backed up by a throat culture (strong, high). Positive RADTs do not necessitate a back-up culture because they are highly specific. 2. 2. Routine use of back-up throat cultures for those with a negative RADT is not necessary for adults in usual circumstances, because of the low incidence of GAS pharyngitis in adults and because the risk of subsequent acute rheumatic fever is generally exceptionally low in adults with acute pharyngitis . Physicians who wish to ensure they are achieving maximal sensitivity in 3 diagnosis may continue to use conventional throat culture or to back up negative RADTs with a culture. 3. 3. Anti-streptococcal antibody titers are not recommended in the routine diagnosis of acute pharyngitis as they reflect past but not current events. (IDSA 2012) Searches AmeriHealth Caritas Pennsylvania searched PubMed and the databases of: UK National Health Services Centre for Reviews and Dissemination. Agency for Healthcare Research and Quality’s National Guideline Clearinghouse and other evidence-based practice centers. The Centers for Medicare & Medicaid Services (CMS). We conducted searches on January 28, 2016. Search terms were: “molecular test, pharyngitis, streptococci, throat culture, rapid streptococcal test, pharyngeal carriers, tonsillectomy, and streptococcal antibody tests” We included: Systematic reviews, which pool results from multiple studies to achieve larger sample sizes and greater precision of effect estimation than in smaller primary studies. Systematic reviews use predetermined transparent methods to minimize bias, effectively treating the review as a scientific endeavor, and are thus rated highest in evidence-grading hierarchies. Guidelines based on systematic reviews. Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple cost studies), reporting both costs and outcomes — sometimes referred to as efficiency studies — which also rank near the top of evidence hierarchies. Findings The current gold standard for laboratory diagnosis of GAS pharyngitis is culture of pharyngeal swab specimens. Cultures are screened for the presence of beta-hemolytic colonies, which are positively identified as GAS using standard biochemical tests (e.g., catalase, pyrrolidonyl arylamidase, and latex agglutination for type-specific antigen tests). While sensitive, culture requires up to 48 h of incubation, which is problematic for physicians considering antibiotic therapy as an option for treating acute pharyngitis. ( Mitchell MS, 2011). Although commercial rapid antigen detection tests (RADTs) are more expensive than blood agar plate (BAP) cultures, the advantage they offer is the speed with which they provide results. Rapid identification and consequent prompt treatment of patients with pharyngitis due to group A betahemolytic streptococci (GABHS) can reduce the risk of spread of GABHS, can allow patients to return to school or work sooner, and may reduce the acute morbidity of this illness. In most studies, RADTs have been compared with BAP cultures as the criterion standard. However, these comparisons are complicated by the fact that there is no universally accepted procedure for performing a BAP culture. The great majority of the RADTs that are currently available have a high specificity (i.e., 95% or greater) and a sensitivity of between 70 and 90% compared with BAP cultures. Few published studies have compared the performance of various RADTs to each other or examined the performance of various RADTs in the office setting. There is also relatively little published information about how physicians in 4 practice actually use RADTs, but the available information suggests that many physicians do not follow recommended guidelines. While the development of easy-to-perform RADTs for the diagnosis of GABHS pharyngitis has altered clinical practice substantially, only limited data about cost-effectiveness are currently available. Point-of-care (POC) tests offer potentially substantial benefits for the management of infectious diseases, mainly by shortening the time to result and by making the test available at the bedside or at remote care centers. Commercial POC tests are already widely available for the diagnosis of bacterial and viral infections and for parasitic diseases, including malaria. Infectious diseases specialists and clinical microbiologists should be aware of the indications and limitations of each rapid test, so that they can use them appropriately and correctly interpret their results. The clinical applications and performance of the most relevant and commonly used POC tests are reviewed. Some of these tests exhibit insufficient sensitivity, and should therefore be coupled to confirmatory tests when the results are negative (e.g. Streptococcus pyogenes rapid antigen detection test), whereas the results of others need to be confirmed when positive (e.g. malaria). New molecular-based tests exhibit better sensitivity and specificity than former immunochromatographic assays (e.g. Streptococcus agalactiae detection). In the coming years, further evolution of POC tests may lead to new diagnostic approaches, such as panel testing, targeting not just a single pathogen, but all possible agents suspected in a specific clinical setting. To reach this goal, the development of serology-based and/or molecular-based microarrays/multiplexed tests will be needed. The availability of modern technology and new microfluidic devices will provide clinical microbiologists with the opportunity to be back at the bedside, proposing a large variety of POC tests that will allow quicker diagnosis and improved patient care. PMID: 20670287 [PubMed - indexed for MEDLINE]. Policy updates: Summary of clinical evidence: Citation Rogo T et al. (2010) Comparison of the Inverness Medical Acceava Strep A test with the Genzyme OSOM and Quidel QuickVue Strep A tests. Content, Methods, Recommendations Key points: Schmuziger N et al. (2003) Reliability and general practice value of 2 rapid Streptococcus A tests. Previous studies of the accuracy of rapid in-office tests for group A Streptococcus had disparate results, ranging from a sensitivity of 70% to more than 90%. The sensitivity and specificity of 3 commercially available Strep A tests were determined in 2 private pediatric office settings. Acceava Strep A, Genzyme OSOM Strep A, and the Quidel QuickVue Strep A tests were the representative rapid tests for detection of Streptococcus pyogenes. Overnight culture on standard 5% sheep blood agar was the reference standard for this study. All 3 Clinical Laboratory Improvement Amendments-waived tests had sensitivities and specificities that exceeded 95%. Key points: Results of the optical immunoassay and the conventional immune assay Strep A Plus were compared in 65 patients with acute pharyngitis. A standard culture was used as reference and confirmed by enhanced broth culturing and nucleic acid hybridization assay (Gen-Probe) when the two detection assays produced contradictory results. While both assays were equally sensitive (78.3%), Strep A OIA MAX and Strep A Plus had a similar specificity of 95.2% and 100%, respectively. Four and nine steps were required for Strep A Plus and for Strep A OIA MAX test procedures, respectively with results being available in 4-5 min and in 9-10 min, respectively. 5 Citation Content, Methods, Recommendations Concluded that both rapid immunoassays have a similar reliability while the handling of the Strep A Plus is much simpler than the handling of the Strep A OIA MAX. Neither rapid immunoassays are sensitive enough to eliminate the need for backup cultures. Neuner JM et al. (2003) Diagnosis and management of adults with pharyngitis. A cost-effectiveness analysis. Key points: Five strategies for the management of adult patients with pharyngitis: 1) observation without testing or treatment, 2) empirical treatment with penicillin, 3) throat culture using a two-plate selective culture technique, 4) optical immunoassay (OIA) followed by culture to confirm negative OIA test results, or 5) OIA alone. Observation, culture, and two rapid antigen test strategies for diagnostic testing and treatment of suspected GAS pharyngitis in adults have very similar effectiveness and costs, although culture is the least expensive and most effective strategy when the GAS pharyngitis prevalence is 10%. Empirical treatment was not the most effective or least expensive strategy at any prevalence of GAS pharyngitis in adults, although it may be reasonable for individual patients at very high risk for GAS pharyngitis as assessed by a clinical decision rule. Le Marechal F et al ( 2012) Streptococcal pharyngitis in children: a meta-analysis of clinical decision rules and their clinical variables Key points: To identify the best clinical decision rules (CDRs) for diagnosing group A streptococcal (GAS) pharyngitis in children. A combination of symptoms could help clinicians exclude GAS infection in children with pharyngitis. The rule of Joachim et al could be useful for clinicians who do not use rapid diagnostic tests and should allow avoiding antibiotic treatment for the 35% of children identified by the rule as not having GAS pharyngitis. Owing to its poor specificity, such CDR should be used to focus rapid diagnostic tests to children with high risk of GAS pharyngitis to reduce the antibiotic consumption. Mayo Clin Proc.( 2012) Current concepts in laboratory testing to guide antimicrobial therapy. Key points: Antimicrobial susceptibility testing (AST) is indicated for pathogens contributing to an infectious process that warrants antimicrobial therapy if susceptibility to antimicrobials cannot be predicted reliably based on knowledge of their identity. Such tests are most frequently used when the etiologic agents are members of species capable of demonstrating resistance to commonly prescribed antibiotics. Some organisms have predictable susceptibility to antimicrobial agents (i.e., Streptococcus pyogenes to penicillin), and empirical therapy for these organisms is typically used. Therefore, AST for such pathogens is seldom required or performed. In addition, AST is valuable in evaluating the activity of new and experimental compounds and investigating the epidemiology of antimicrobial resistant pathogens. Several laboratory methods are available to characterize the in vitro susceptibility of bacteria to antimicrobial agents. When the nature of the infection is unclear and the culture yields mixed growth or usual microbiota (wherein the isolates usually bear little relationship to the actual infectious process), AST is usually unnecessary and results may, in fact, be dangerously misleading. Phenotypic methods for detection of specific antimicrobial resistance mechanisms are increasingly being used to complement AST (i.e., inducible clindamycin resistance among several gram-positive bacteria) and to provide clinicians with preliminary direction for antibiotic selection pending results generated from standardized AST (i.e., β-lactamase tests). In addition, molecular methods are being developed and incorporated by microbiology laboratories into resistance detection algorithms for rapid, sensitive assessment of carriage states of epidemiologically and clinically important pathogens, often directly from clinical specimens (i.e., presence of vancomycin-resistant enterococci in fecal specimens). 6 Glossary The illumigene® Molecular Diagnostic System— Is simple, delivering the power of molecular technology in a "rapid test" type format; flexible, integrating easily into any facility regardless of volume or expertise; and cost-effective, allowing addition of molecular assays without the cost of additional labor or capital expenditures. References Professional society guidelines/other: Infectious Diseases Society of America (IDSA) http://www.idsociety.org/uploadedFiles/IDSA/GuidelinesPatient_Care/PDF_Library/2012%20Strep%20Guideline.pdf American Society for Microbiology (ASM). Rapid diagnosis of Pharyngitis caused by Group A streptococci Clinical Microbiology Reviews. doi: 10.1128/CMR.17.3.571-580.2004 Clin. Microbiol. April 2016, volume 29, issue 2 1 April 2016, Rev. July 2004 vol. 17 no. 3 571-580 .1 July 2004. Clin Microbiol Infect. 2010 Aug; 16(8):1054-61. doi: 10.1111/j.1469-0691.2010.03281.x. Routine use of point-of care tests: usefulness and application in clinical microbiology. Clerc O, Greub G. Mayo Clin Proc. 2012 Mar; 87(3):290-308. doi: 10.1016/j.mayocp.2012.01.007. Current concepts in laboratory testing to guide antimicrobial therapy. Jenkins SG, Schuetz AN. PMCID: PMC3496983 PMID: 22386185 [PubMed - indexed for MEDLINE]. Peer-reviewed references: Badgett JT, Hesterberg LK. Management of group streptococcus pharyngitis with a second-generation rapid strep screen: Strep A OIA. Microb Drug Resist. 1996 Fall; 2(3):371-6. Review.PMID:9158797. Bisno AL, Gerber MA, Gwaltney JM Jr, Kaplan EL, Schwartz RH. Practice guidelines for the diagnosis and management of group a streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis 2002; 35:113–25. Bisno AL. Acute pharyngitis: etiology and diagnosis. Pediatrics 1996; 97:949–54. BMJ Open. Streptococcal pharyngitis in children: a meta-analysis of clinical decision rules and their clinical variables 2013; 3:e001482 doi: 10.1136/bmjopen-2012-001482. http://bmjopen.bmj.com/content/3/3/e001482. Accessed February 4, 2016. Brien JH, Bass JW. Streptococcal pharyngitis: optimal site for throat culture. J Pediatr 1985; 106:781–3. Felsenstein S, Faddoul D, Sposto R, Batoon K, et al. Molecular and clinical diagnosis of group A streptococcal pharyngitis in children. J Clin Microbiol. 2014 Nov; 52(11):3884-9. doi: 10.1128/JCM.01489-14. Epub 2014 Aug 20. PMID: 25143573 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4313219/. Assessed January 22, 2016. 7 Gerber MA. Diagnosis of pharyngitis: methodology of throat cultures.In: Shulman ST, ed. Pharyngitis: management in an era of declining rheumatic fever. New York: Praeger, 1984:61–72. Gerber MA. Comparison of throat cultures and rapid strep tests for diagnosis of streptococcal pharyngitis. Pediatr Infect Dis J 1989; 8:820–4. Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococci. Clin Microbiol Rev 2004; 17:571–80. Guilherme L, Faé KC, Higa F, Chaves L, et al. Towards a vaccine against rheumatic fever. Clin Dev Immunol. 2006 Jun-Dec;13(2-4):125-32. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008; 336:924-6. Hayes Inc., Hayes Medical Technology Report. Lansdale, Pa. Hayes Inc.; February, 2016. Kaplan EL, Top FH Jr., Dudding BA, Wannamaker LW. Diagnosis of streptococcal pharyngitis: differentiation of active infection from the carrier state in the symptomatic child. J Infect Dis 1971; 123:490-501. Langlois DM, Andreae M. 2011. Group A streptococcal infections. Pediatr. Rev. 32:423–429. Mitchell MS, Sorrentino A, Centor RM. 2011. Adolescent pharyngitis: a review of bacterial causes. Clin. Pediatr. (Phila.) 50:1091–1095. Neuner JM, Hamel MB, Phillips RS, Bona K, et al. Diagnosis and management of adults with pharyngitis. A cost-effectiveness analysis. .Ann Intern Med. 2003 Jul 15;139(2):113-22.PMID:12859161. Randolph MF, Gerber MA, DeMeo KK, Wright L. Effect of antibiotic therapy on the clinical course of streptococcal pharyngitis. J Pediatr 1985; 106:870–5. Rogo T, Schwartz RH, Ascher DP. Comparison of the Inverness Medical Acceava Strep A tests with the Genzyme OSOM and Quidel QuickVue Strep A tests. Clin Pediatr (Phila). 2011 Apr; 50(4):294-6. doi: 10.1177/0009922810385675. Epub 2010 Nov 22.PMID: 21098521. Schmuziger N, Schneider S, Frei R. Reliability and general practice value of 2 rapid Streptococcus A tests HNO. 2003 Oct; 51(10):806-12. Epub 2003 Apr 11. German. PMID: 1452353. Schwartz RH, Gerber MA, McCoy P. Effect of atmosphere of incubation on the isolation of group A streptococci from throat cultures. J Lab Clin Med 1985; 106:88–92. Schunemann HJ, Oxman AD, Brozek J, et al. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ 2008; 336:1106-10. Snow V, Mottur-Pilson C, Cooper RJ, Hoffman JR. Principles of appropriate antibiotic use for acute pharyngitis in adults. Ann Intern Med 2001; 134:506–8. 8 Uhl JR, Adamson SC, Vetter EA, Schleck CD, Harmsen WS, Iverson LK, Santrach PJ, Henry NK, Cockerill FR. 2003. Comparison of LightCycler PCR, rapid antigen immunoassay, and culture for detection of group A streptococci from throat swabs. J. Clin. Microbiol. 41:242–249. Abstract/FREE Full Text. Clinical trials: Searched clinicaltrials.gov on February 01, 2016 using terms molecular test, strep A | Open Studies. None studies found, none relevant. CMS National Coverage Determinations (NCDs): No NCDs identified as of the writing of this policy. Local Coverage Determinations (LCDs): No LCDs identified as of the writing of this policy Commonly submitted codes Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and bill accordingly. CPT Code Description 87651 Illumigene for Group A Streptococcus ICD-10 Code Description A49.1 Streptococcus infection, unspecified site HCPCS Code Description Comments Comments Comments N/A 9