Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
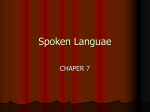
Am J Physiol Heart Circ Physiol 312: H392–H405, 2017. First published December 23, 2016; doi:10.1152/ajpheart.00644.2016. RESEARCH ARTICLE Cardiac Excitation and Contraction Cardiac sympathetic innervation via middle cervical and stellate ganglia and antiarrhythmic mechanism of bilateral stellectomy Tadanobu Irie,1,2* Kentaro Yamakawa,2* David Hamon,1,2 Keijiro Nakamura,1,2 Kalyanam Shivkumar,1,2 and Marmar Vaseghi1,2 1 UCLA Cardiac Arrhythmia Center, Los Angeles, California; and 2Neurocardiology Research Center of Excellence, Los Angeles, California Submitted 26 September 2016; accepted in final form 16 December 2016 NEW & NOTEWORTHY Sympathetic activation in myocardial infarction leads to arrhythmias and worsens heart failure. Bilateral cardiac sympathetic denervation reduces ventricular tachycardia/ventricular fibrillation inducibility and mitigates effects of sympathetic activation on dispersion of repolarization and T-peak to T-end interval in infarcted hearts. Hemodynamic stability is maintained, as innervation via the middle cervical ganglion is not interrupted. Listen to this article’s corresponding podcast at https://ajpheart. podbean.com/e/anti-arrhythmic-mechanism-of-bilateral-stellectomy/. * T. Irie and K. Yamakawa contributed equally to this work. Address for reprint requests and other correspondence: M. Vaseghi, UCLA Cardiac Arrhythmia Ctr., 100 Medical Plaza, Ste. 660, Los Angeles, CA 90095 (e-mail: [email protected]). H392 autonomic nervous system; cardiac sympathetic denervation; stellectomy; ventricular arrhythmias; sympathetic nervous system (MI) increases the risk of sudden cardiac death due to ventricular tachyarrhythmias [ventricular tachycardia (VT)/ventricular fibrillation (VF)] (13) by causing pathological cardiac (16, 34, 41) and neural (15, 44, 53) remodeling. Sympathetic activation via the right or left stellate ganglion increases T-peak to T-end (Tp-Te) interval, a marker of sudden cardiac death (8, 33), and increases dispersion of repolarization (DOR), predisposing to VT/VF (27, 44, 45, 50). Left cardiac sympathetic denervation (CSD) has been reported to decrease the burden of VT/VF in patients with hereditary channelopathies, including long QT syndrome and catecholaminergic polymorphic ventricular tachycardia, who have structurally normal hearts (4, 17, 38). In a small series of patients with structural heart disease, bilateral CSD has shown promise in reducing the burden of internal cardioverter defibrillator (ICD) shocks. This study also suggested that bilateral CSD may lead to a greater ICD shock-free survival compared with left CSD in patients with cardiomyopathy (43). However, the electrophysiological mechanisms behind the reduction in life-threatening arrhythmias with CSD are not clear. In addition, it is unknown how much of cardiac sympathetic innervation, which may be required for beat-to-beat function, is preserved after bilateral CSD. The middle cervical ganglia (MCGs), located anatomically superior to the stellate ganglia, have been reported to contain cardiac sympathetic neurons (7, 21) and could provide sympathetic innervation after CSD. However, their electrophysiological effects have not been characterized. The purpose of this study was to delineate 1) sympathetic innervation of the heart via the MCG compared with the stellate ganglia, 2) electrophysiological and antiarrhythmic effects of CSD, including VT inducibility, and 3) alterations in functional cardiac sympathetic innervation after CSD and its antiarrhythmic mechanisms in a porcine model. MYOCARDIAL INFARCTION METHODS Study procedures were approved by the UCLA Institutional Animal Research Committee and were performed in compliance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals. Creation of myocardial infarcts. Eighteen Yorkshire pigs were sedated (6 –10 mg/kg Telazol and 2–5 g/kg fentanyl), intubated, and placed under general anesthesia with inhaled isoflurane (0.5–1.5%). After femoral arterial access was obtained with an 8-F sheath, an 0363-6135/17 Copyright © 2017 the American Physiological Society http://www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 Irie T, Yamakawa K, Hamon D, Nakamura K, Shivkumar K, Vaseghi M. Cardiac sympathetic innervation via middle cervical and stellate ganglia and antiarrhythmic mechanism of bilateral stellectomy. Am J Physiol Heart Circ Physiol 312: H392–H405, 2017. First published December 23, 2016; doi:10.1152/ajpheart.00644.2016.— Cardiac sympathetic denervation (CSD) is reported to reduce the burden of ventricular tachyarrhythmias [ventricular tachycardia (VT)/ ventricular fibrillation (VF)] in cardiomyopathy patients, but the mechanisms behind this benefit are unknown. In addition, the relative contribution to cardiac innervation of the middle cervical ganglion (MCG), which may contain cardiac neurons and is not removed during this procedure, is unclear. The purpose of this study was to compare sympathetic innervation of the heart via the MCG vs. stellate ganglia, assess effects of bilateral CSD on cardiac function and VT/VF, and determine changes in cardiac sympathetic innervation after CSD to elucidate mechanisms of benefit in 6 normal and 18 infarcted pigs. Electrophysiological and hemodynamic parameters were evaluated at baseline, during bilateral stellate stimulation, and during bilateral MCG stimulation in 6 normal and 12 infarcted animals. Bilateral CSD (removal of bilateral stellates and T2 ganglia) was then performed and MCG stimulation repeated. In addition, in 18 infarcted animals VT/VF inducibility was assessed before and after CSD. In infarcted hearts, MCG stimulation resulted in greater chronotropic and inotropic response than stellate ganglion stimulation. Bilateral CSD acutely reduced VT/VF inducibility by 50% in infarcted hearts and prolonged global activation recovery interval. CSD mitigated effects of MCG stimulation on dispersion of repolarization and T-peak to T-end interval in infarcted hearts, without causing hemodynamic compromise. These data demonstrate that the MCG provides significant cardiac sympathetic innervation before CSD and adequate sympathetic innervation after CSD, maintaining hemodynamic stability. Bilateral CSD reduces VT/VF inducibility by improving electrical stability in infarcted hearts in the setting of sympathetic activation. H393 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY A B Subclavian Artery MCG Sympathetic Chain D on the epicardium was assessed in infarcted animals grossly (Fig. 1), as well as by bipolar voltage measurements with a 2-2-2 duodecapolar catheter [2-2-2 electrode spacing (mm), St. Jude Medical, St. Paul, MN]. Regions with a voltage ⬍ 0.5 mV were defined as scar, those with voltage of 0.5-1.5 mV were defined as border zone, and electrodes overlying regions with voltage ⬎ 1.5 mV were defined as viable/normal (14, 23). The location and extent of infarct were marked on the heart. The MCG were identified often above and behind the subclavian artery, at the inlet of the thorax (Fig. 1) After completion of the surgical portion of the procedure isoflurane was discontinued, and an intravenous infusion of ␣-chloralose (10 –30 mg·kg⫺1·h⫺1) was begun (5, 10, 11). During anesthesia with both ␣-chloralose and isoflurane, heart rate (HR) as well as jaw tone and eyeblink reflexes were monitored every 10 –15 min to ensure adequate sedation. Stellate and middle cervical ganglion stimulation. Bipolar needle electrodes (Fig. 1) were used for bilateral stellate ganglion stimulation and bilateral MCG stimulation with a Grass Stimulator (model S88, Grass Technologies, Warwick, RI) in both infarcted (n ⫽ 12) and normal (n ⫽ 6) animals. Threshold was defined as the current needed to increase HR or systolic blood pressure by 10% (at 4 Hz, 4 ms). Stimulation was performed at 1.5 times threshold for 30 s. In normal animals, the stimulation current used was 2.4 ⫾ 0.5 mA for the right stellate ganglion and 2.3 ⫾ 0.4 mA for the right MCG; the stimulation current was 5.6 ⫾ 0.8 mA for the left stellate ganglion and 6.0 ⫾ 0.7 mA for the left MCG. For infarcted animals, the stimulation current used was 6.7 ⫾ 1.0 mA for the right stellate ganglion and 5.9 ⫾ 1.2 mA for the right MCG; the stimulation current was Ansa Subclavia C Needle Electrode Cardiopulmonary Nerves MCG F E RV Ant RVOT LAD RV Lat RV LV Ant LAD LV LV Lat RV Post Apex LV Post Fig. 1. Isolation of the middle cervical ganglia (MCG) and Tp-Te interval and ARI recordings. A: anatomy of MCG and surrounding tissue is shown. The MCG sits just at the thoracic inlet and provides cardiopulmonary nerves that innervate the heart. B: customized bipolar needle electrodes were placed in the isolated MCG. C: method for the measurement of Tp-Te interval from surface ECG. The peak of the T wave was determined as the highest voltage of the T wave (T-p). T-end (T-e) was determined by the tangent of the T wave. D: the region of scar in infarcted hearts predominantly involved the LV apex, anterior, and anterolateral walls. E: 56-electrode sock is placed over the ventricles to obtain unipolar electrograms that are used for ARI analysis. F: template for the polar maps used to display regional ARIs from the sock electrodes. Ant, anterior; Lat, lateral; Post, posterior; RVOT, right ventricular outflow tract. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 Amplatz guide catheter (Boston Scientific, Marlborough, MA) was advanced over a J-tipped guide wire under fluoroscopic guidance and used to cannulate the left main coronary artery from the left femoral artery. A coronary angiogram was performed to delineate the branches of the left anterior descending coronary artery (LAD). A 3-mm luminal angioplasty balloon (Armada 35 PTA, Abbott Vascular, Temecula, CA) was advanced past the first diagonal branch of the LAD over a 0.014-in. coronary guide wire (Balance Middle Weight wire, Abbott Vascular) and inflated. Polystyrene microspheres (5.0 – 7.5 ml, Polysciences, Warrington, PA) were injected through the lumen of the percutaneous balloon catheter (26). Repeat coronary angiography after microsphere injection showed confirmed poor blood flow in the LAD after the first diagonal branch. Continuous electrocardiogram (ECG) monitoring was performed. ECG changes including ST segment elevation and or T-wave inversions were also used to confirm MI acutely. If sustained VT/VF was observed, resuscitation with chest compressions and external direct-current cardioversion was performed. Animals were then extubated and monitored until they could ambulate without assistance. Surgical preparation. Four to six weeks after MI, 18 infarcted (48 ⫾ 2 kg) and 6 normal (43 ⫾ 1 kg) animals were sedated (6 –10 mg/kg Telazol and 2–5 g/kg fentanyl) and placed under general anesthesia with isoflurane (0.8 –1.5%). Normal animals had not undergone a percutaneous interventional procedure before terminal experiments. Median sternotomy was performed, and isolation of bilateral stellate ganglia and T2 thoracic ganglia (all animals) and bilateral MCG (12 of 18 animals) was performed. Presence and extent of scar H394 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY A Timeline of Experimental Protocol in Normal Animals B 350 300 P < 0.05 350 300 LAD 12 LV 10 Apex BL 8 6 LAD RV 2 200 200 BL BSGS BL BMCGS LAD 376 364 352 340 327 315 303 291 279 266 254 242 RV 4 250 250 P = 0.4 14 Change in ARI (%) 400 Global ARI (ms) Global ARI (ms) P < 0.05 0 LV BSGS BMCGS Apex RV LV Apex BL LAD RV LV ARI (ms) BSGS Apex BMCGS Fig. 2. Experimental protocol in normal hearts and effect of bilateral stellate ganglion stimulation (BSGS) compared with bilateral MCG stimulation (BMCGS). A: timeline of the experimental protocol in 6 normal animals. HEX, hexamethonium. *BMCGS or BSGS was performed in a random order. B: in all normal animals, BMCGS had an effect on ARI similar to that of BSGS. C: polar maps from a normal animal show the effects of MCG and stellate ganglion stimulation on ARI. Blue dashed lines indicate course of left anterior descending coronary artery (LAD). BL, baseline. 9.8 ⫾ 1.0 mA for left stellate ganglion stimulation and 10.0 ⫾ 1.0 mA for left MCG. In normal animals, a second stellate and MCG stimulation was performed before CSD for 60 s and electrophysiological effects were compared at 5, 10, 15, 20, 30, 45, and 60 s. A 30-min period was allowed for return of hemodynamic parameters to baseline in between stimulations. The timeline for the experimental protocol in normal animals is shown in Fig. 2. Hemodynamic and electrocardiogram recordings. Hemodynamic parameters were continuously recorded with a 12-pole conductance pressure catheter in the left ventricle (LV), connected to a MPVS Ultra Pressure Volume Loop System (Millar Instruments, Houston, TX). ECG was continuously obtained with the GE Cardiolab System (GE Healthcare). Tp-Te interval was assessed in the inferior leads with the clearest T wave off-line manually from the electrocardiograms obtained from the Cardiolab System at 400 mm/s paper speed. Tp-Te interval was measured from the peak of T wave to the end of T wave. The peak of the T wave was visually determined, and the end of the T wave was defined as the intersection of the tangent to the slope of the T wave and the isoelectric line, when not followed by a U wave (Fig. 1). If a U wave followed the T wave, the offset of the T wave was measured as the nadir between the T and U waves. This method is similar to what has been described in the literature (29, 50). Bilateral cardiac sympathetic denervation. Bilateral CSD was performed in 18 infarcted and 6 normal animals after isolation of bilateral stellate and T2 thoracic ganglia. T3 and T4 thoracic ganglia were not removed, as it has been shown previously that cardiac fibers from these ganglia traverse through the stellate and T2 ganglia before reaching the heart (12). The lungs on each side were retracted, the sympathetic chain was again identified, and its connections to the spinal cord and cardiopulmonary nerves were transected. Both stellate ganglia and T2 thoracic ganglia were removed. A 30-min stabilization Table 1. Hemodynamic parameters in normal animals BL (PreBSGS) BSGS BL (PreMCGS) BMCGS (PreCSD) HR, bpm 84 ⫾ 17 98 ⫾ 13* 89 ⫾ 14 1,178 ⫾ 166 2,391 ⫾ 724* 1,086 ⫾ 116 dP/dtmax, mmHg/s dP/dtmin, mmHg/s ⫺1,126 ⫾ 317 ⫺1,149 ⫾ 462 ⫺1,172 ⫾ 337 LVESP, mmHg 103 ⫾ 20 147 ⫾ 23* 99.5 ⫾ 21 103 ⫾ 10* 2,364 ⫾ 531* ⫺1,174 ⫾ 302 134 ⫾ 24*§ PreCSD PostCSD 86 ⫾ 12 89 ⫾ 8 1,032 ⫾ 157 1,087 ⫾ 296 ⫺1,121 ⫾ 353 ⫺1,094 ⫾ 286 97.5 ⫾ 22 94 ⫾ 16 BL (PreMCGS PostCSD) BMCGS (PostCSD) 90 ⫾ 12 1,007 ⫾ 228 ⫺984 ⫾ 266 87 ⫾ 13 104 ⫾ 10* 2,232 ⫾ 467* ⫺1,149 ⫾ 382 125 ⫾ 20*† Values represent mean ⫾ SD % change in parameters from prestimulation value (n ⫽ 6). PreCSD represents hemodynamic values immediately before removal of the stellate ganglia. PostCSD values represent hemodynamic parameters after a 30-min period of stabilization after removal of stellate ganglia. HR, heart rate; bpm, beats per minute; dP/dtmax, dP/dtmin, maximum and minimum dP/dt; LVESP, left ventricular end-systolic pressure; BL, baseline; BSGS, bilateral stellate ganglion stimulation; BMCGS, bilateral middle cervical ganglion stimulation. *P value ⬍ 0.05 for % change from baseline (prestimulation). †P ⫽ 0.08 for % increase in LVESP with BMCGS PreCSD vs. PostCSD. §P ⫽ 0.02 for comparison of % change in LVESP for BSGS vs. BMCGS. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 400 C ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY Table 2. Norepinephrine levels in normal and infarcted animals Normal pigs (CS) Normal pigs (IVC) Infarct pigs (CS) Infarct pigs (IVC) Baseline BSGS Baseline 0.38 ⫾ 0.09 0.58 ⫾ 0.22 1.35 ⫾ 0.41 1.97 ⫾ 0.54 8.70 ⫾ 2.28* 1.52 ⫾ 0.29* 7.47 ⫾ 1.48* 2.53 ⫾ 0.28 BMCGS 0.54 ⫾ 0.16 13.73 ⫾ 4.47* 0.55 ⫾ 0.07 1.61 ⫾ 0.29* 1.79 ⫾ 0.51 7.83 ⫾ 2.16* 1.89 ⫾ 0.46 3.78 ⫾ 0.95* Values (in ng/ml) are means ⫾ SE. CS, coronary sinus; IVC, inferior vena cava; BSGS, bilateral stellate ganglion stimulation; BMCGS, bilateral middle cervical ganglion stimulation. *P ⬍ 0.05 compared with baseline. BSGS Percent Change in ARI (%) A BMCGS Pre-CSD 0 -5 -10 -15 -20 -25 5sec B 10sec 15sec 20sec 30sec 45sec 30 Change in ARI (%) connected to a MicroPace stimulator (MicroPace EP, Santa Ana, CA). Current was set at two times the ventricular capture threshold in each animal with a pulse duration of 1 ms. If VT/VF was not induced from the RV endocardium at baseline before CSD, a second site on the LV epicardium close to the scar was used before CSD. The same or a very similar site was used for induction of VT/VF after CSD as had been used to induce VT/VF before CSD. The induction protocol was as follows: an extrastimulus was placed after 8 beats of drive cycle length (at 500 ms) at an interval of 400 ms (S2). The premature extrastimulus interval (S2) was reduced by 10 ms until either an interval of 200 ms or an ERP was reached or VT/VF was induced. If VT/VF was not induced, then S2 was fixed at 20 ms above the ERP or at 220 ms (if ERP was ⬍200 ms) and a second premature extrastimulus (S3) was added at an interval of 400 ms. The S3 interval was then reduced by 10 ms until an S2–S3 interval of 200 ms or ERP was reached or VT/VF was induced. Finally, if no VT/VF was induced, then the S3 interval was set at 220 ms (if ERP was ⬍200 ms) or 20 ms above ERP and an S4 interval (triple extrastimulus) was added at an S3–S4 interval of 400 ms. This S4 interval was then reduced by 10 ms until a coupling interval of 200 ms or effective period was reached or VT/VF was induced. Inducibility was defined 60sec BSGS BMCGS Pre-CSD 25 20 15 10 5 0 Apex Ant Lat Post Post Lat LV C Global ARI (ms) 260 Ant RVOT RV P < 0.05 Fig. 3. A: the time course of ARI shortening with bilateral stellate ganglion stimulation (BSGS) was similar to that with bilateral MCG stimulation (BMCGS) (n ⫽ 6). B: there were no significant regional differences between BSGS and BMCGS in normal hearts (P values ⬎ 0.05 for all regions, n ⫽ 6). C: apical ventricular pacing before CSD demonstrated shorter global ARIs than right atrial (RA) pacing in normal animals (n ⫽ 6) at the same cycle lengths. However, after CSD there was no significant difference in ARI between ventricular and atrial pacing, suggesting that apical pacing may cause reflex sympathetic activation that is prevented by CSD. Ant, anterior; Lat, lateral; Post, posterior wall; RV, right ventricle; LV, left ventricle. RA Pacing Apical Pacing P = 0.6 250 P = 0.5 240 P < 0.05 230 220 210 200 BL Pre-CSD BMCGS Pre-CSD Pre-CSD BL Post-CSD BMCGS Post-CSD Post-CSD AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 period after CSD was allowed before repeat stimulation or inducibility testing. VT/VF inducibility was tested before and after CSD. Inducibility testing for ventricular tachyarrhythmias. In 18 infarcted hearts, programmed ventricular stimulation up to triple extrastimuli to a minimum coupling interval of 200 ms or an effective refractory period (ERP) was performed before and after CSD first from the right ventricular (RV) endocardium at the mid- to apical septum with an endocardial quadripolar electrophysiology catheter H395 H396 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY as hemodynamically tolerated VT that lasted ⬎30 s or that degenerated into VF requiring direct cardioversion. Measurement of norepinephrine levels. Norepinephrine (NE) levels in the inferior vena cava (IVC) and coronary sinus (CS) were measured to confirm adequate ganglion stimulation. Venous blood was obtained from a luminal catheter inserted in the IVC, superior to the adrenal veins and close to the right atrium. CS blood was obtained by cannulation of the CS with a luminal catheter (St. Jude Medical, St. Paul, MN) from the right external jugular vein. Blood samples at baseline and in the last 5 s of stellate ganglion and MCG stimulation before CSD were immediately centrifuged (3,000 rpm, 15 min) to separate the plasma portion. Quantification of NE was performed with A B PreCSD PostCSD ARI (ms) C 300 BMCGS Post-CSD * * * * * 250 200 Apex Ant Lat Post 300 250 BL 20 P = 0.6 15 10 5 0 BMCGS PreCSD Post Lat LV Ant RVOT BMCGS Pre-CSD BMCGS Post-CSD 20 10 0 Apex Ant RV Lat Post Post Lat Ant RVOT RV LV D PostCSD 30 E 800 800 P<0.05 700 600 600 DOR (ms2) 700 500 400 300 Normal Hearts Post-CSD - Normal Hearts 80 P<0.05 Tp-Te Interval (ms) Pre-CSD - Normal Hearts 500 400 P=0.1 P=0.1 60 40 20 300 200 200 BL BMCGS BMCGS 80 P=0.9 60 40 20 0 0 BL Percent Change in Tp-Te (%) ARI (ms) * 350 25 Post-CSD BL * P < 0.03 200 400 350 Percent Change in ARI (%) Global ARI (ms) 250 Pre-CSD Percent change in ARI (%) Global ARI (ms) 300 400 BMCGS BL BMCGS Pre-CSD BL BMCGS Post-CSD PreCSD PostCSD Fig. 4. Effects of CSD in normal animals. A: there was no difference in global ARI in normal heart before compared with after CSD. B: bilateral MCG stimulation after CSD had similar effects on global ARI compared with before CSD, with significant ARI shortening observed. C: there were no differences in the regional effects of MCG stimulation after CSD compared with before CSD. *P ⬍ 0.05; †P ⬍ 0.1. D: before CSD bilateral MCG stimulation increased dispersion of repolarization in normal hearts, and this effect was not modified by CSD. E: bilateral MCG stimulation in normal hearts also increased Tp-Te interval, with no differences observed in this parameter before compared with after CSD in normal hearts. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 350 200 Post-CSD 355 349 342 336 329 323 316 310 303 297 291 284 P = 0.2 400 DOR (ms2) an ultrasensitive enzyme-linked immunoassay (ELISA) (BA E-5200, sensitivity 1.3 pg/ml, Labor Diagnostika Nord, Nordhorn, Germany) and an ELISA microplate reader (Fisher Scientific, Waltham, MA). Activation recovery interval recordings. In 12 infarcted and 6 normal animals, detailed electrophysiological mapping was performed. A 56-electrode sock (Fig. 1) was placed over the ventricles to assess activation recovery interval (ARI), a surrogate of local action potential duration. Unipolar electrograms were recorded (0.05–500 Hz) with the GE Cardiolab System. ARIs were calculated with customized software (ScalDyn, University of Utah, Salt Lake City, UT) as previously described (44, 46). Briefly, activation time (AT) was defined as the interval from electrogram onset to most negative ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY H397 Preganglionic vs. postganglionic neural fibers within MCG. To evaluate presence of pre- vs. postganglionic fibers within the MCG in normal animals after CSD, bilateral MCG stimulation was repeated after infusion of hexamethonium, a nicotinic receptor blocker. Right vagal nerve stimulation (VNS) was also performed before and after hexamethonium infusion to ensure nicotinic receptor blockade, as vagal efferent parasympathetic fibers are known to be preganglionic. The right cervical vagal trunk was isolated via a lateral neck cutdown, and bipolar needle electrodes (Cyberonics, Houston, TX) attached to a Grass stimulator were used for right VNS (10 Hz, 1 ms). Threshold was defined as the current at which HR decreased by 10%, and stimulation was performed at 1.2 times threshold for 20 s, before and after hexamethonium. Hexamethonium was infused for 30 min (0.025– 0.2 mg·kg⫺1·min⫺1, dose titrated by response to right VNS in each animal). Statistical analysis. Unless specified otherwise, data are presented as means ⫾ SE. Global ARI was calculated as the mean ARI across all 56 electrodes. Global DOR was calculated as the variance in ARIs across all 56 electrodes. For comparison of paired variables, Wilcoxon signed-rank test or paired t-test was used was used. Sample size of infarcted animals was driven by the assumption of a 40% reduction in VT/VF inducibility after CSD with 80% power to detect this reduction at an ␣ of 0.05. McNemar’s test was used to compare VT inducibility before and after CSD. Sample size of normal animals was driven by 80% power to detect a 10% difference in the effects of MCG vs. stellate ganglion stimulation on global ARI in the same animal at an ␣ of 0.05. The Mann-Whitney test was used for comparison of A MCG Stim B Right VNS P < 0.05 400 400 P < 0.05 Global ARI (ms) Global ARI (ms) P = 0.6 350 300 350 300 250 250 C Percent Change in ARI (%) P = 0.3 12 10 8 P < 0.05 Fig. 5. Effects of hexamethonium on MCG stimulation. A: the increase in global ARI during right vagal nerve stimulation (VNS) was no longer observed after infusion of hexamethonium (Hex) in normal animals (n ⫽ 6). B: global ARI during bilateral MCG stimulation significantly decreased even after administration of hexamethonium in all normal hearts (n ⫽ 6). C: % change in global ARI during right VNS and bilateral MCGS stimulation showed that hexamethonium significantly blocked nicotinic receptors but did not affect the response to bilateral MCG stimulation. P < 0.05 6 4 2 0 AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 dV/dt of the activation wave, and repolarization time (RT) was defined as the interval from electrogram onset to the most positive dV/dt of the repolarization wave. ARI was defined as the difference between RT and AT. Map3D software (University of Utah, Salt Lake City, UT, http://www.sci.utah.edu/cibc-software/map3d.html) was used to map the epicardial pattern of activation and ARI with a sock-electrode polar map template (Fig. 1F). Global DOR was calculated as the variance of ARIs recorded across all epicardial electrodes. In this article, “anterior” refers to the ventral and “posterior” to the dorsal aspect of the heart. In normal animals, mean ARIs in the following regions were analyzed on the basis of electrode location: LV apex, LV anterior, LV lateral, and LV posterior wall and RV anterior, RV lateral, RV posterior wall, and RV outflow tract. A median of three electrodes (range 2– 4) per region were used for regional ARI and AT analysis. Atrial and ventricular pacing. To evaluate the effect of CSD on ARI during ventricular pacing compared with atrial pacing, ventricular pacing was performed at baseline and during MCG stimulation before and after CSD (pacing cycle length ⫽ 400 ms or 500 ms, depending on HR during stimulation) in six normal and five infarcted animals. To compare differences to ventricular pacing, right atrial pacing at the same cycle length was performed in normal animals at baseline and during bilateral MCG stimulation, before and after CSD. In addition, Map3D software (University of Utah) was used to map the epicardial pattern of activation and ARI during scar pacing in five infarcted hearts. The template, with sock electrode locations, used for creation of these polar maps is shown in Fig. 1. H398 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY continuous variables in different groups. Percent change in regional ARIs for stellate ganglion vs. MCG stimulation were analyzed with repeated-measures ANOVA after controlling for false discovery rate at 5%. SPSS (version 22, IBM, Armonk, NY) was used for statistical analysis. P ⬍ 0.05 was considered statistically significant. RESULTS A Timeline of Creation of Myocardial Infarct and Mapping Experiments in Infarcted Animals C B 350 300 400 Apex 20 BL 15 300 LAD 10 250 200 200 BSGS 424 402 379 357 334 312 289 267 244 222 200 177 25 350 250 BL LAD RV LV Change in ARI (%) Global ARI (ms) Global ARI (ms) P < 0.01 400 P = 0.02 P < 0.01 RV 5 LV 0 BL BMCGS BSGS BMCGS Apex ARI (ms) BSGS LAD RV LV Apex BL LAD RV LV Apex BMCGS Fig. 6. Experimental protocol in infarcted hearts and effect of bilateral stellate ganglion stimulation (BSGS) compared with bilateral MCG stimulation (BMCGS). A: timeline of the experimental protocol in 12 infarcted animals. *BMCGS or BSGS was performed in a random order. B: in all infarcted animals BSGS significantly decreased ARI, as did BMCGS. BMCGS, however, caused greater ARI shortening than BSGS. C: polar maps from an infarcted animal show the effects of MCG and stellate ganglion stimulation on ARI. Black dashed circle indicates region of the infarct/scar on polar maps. Blue dashed lines indicate course of left anterior descending coronary artery (LAD). BL, baseline. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 Thoracic sympathetic innervation in normal hearts. The timeline for the experimental protocol in normal animals is shown in Fig. 2. In normal hearts bilateral stellate ganglion and bilateral MCG stimulation significantly increased HR, maximum dP/dt (dP/dtmax) and LV end-systolic pressure (LVESP) (Table 1). Comparison of bilateral stellate ganglion to bilateral MCG stimulation demonstrated no differences in the HR or dP/dtmax increase. However, bilateral stellate ganglion stimulation had a greater effect on LVESP than bilateral MCG stimulation. CS NE levels increased in a similar fashion during bilateral stellate and bilateral MCG stimulation compared with prestimulation values (Table 2). Both bilateral stellate ganglion and MCG stimulation decreased epicardial ARI (Fig. 2). There was no significant difference in the time course of ARI shortening during the 60 s of stimulation between the stellate ganglia and MCG (Fig. 3), and no differences in regional ARIs were detected between bilateral stellate ganglion and bilateral MCG stimulation (Fig. 3). Compared with right atrial pacing, LV apical pacing at baseline and during MCG stimulation at the same cycle length led to significantly shorter epicardial ARIs (P ⬍ 0.05), sug- gesting that ventricular pacing alone led to cardiac sympathetic activation (Fig. 3). CSD and residual sympathetic innervation in normal hearts. CSD did not cause hemodynamic deterioration in normal hearts (Table 1). No difference in global ARI was observed before compared with after CSD (Fig. 4). MCG continued to exert significant sympathetic effects after CSD. Global ARI continued to decrease during MCG stimulation after CSD (Fig. 4). Effects of bilateral MCG stimulation after CSD on HR and dP/dtmax were unchanged compared with before CSD (Table 1). Of note, comparison of atrial to ventricular pacing at the same cycle length showed that the differences in ARI shortening between right atrial pacing and LV pacing were no longer significant after CSD, with or without MCG stimulation (Fig. 3). DOR and Tp-Te interval, which increased during MCG stimulation, were unaffected by CSD in normal hearts (Fig. 4). Furthermore, CSD had no effect on activation time [pre-CSD: baseline 26.1 ⫾ 1.5 ms vs. MCG stimulation 30.4 ⫾ 4.1 ms (P ⫽ 0.3); post-CSD: baseline 26.1 ⫾ 1.1 ms vs. MCG stimulation 28.2 ⫾ 1.5 ms (P ⫽ 0.2)]. To evaluate presence of preganglionic fibers within the MCG, response to hexamethonium was evaluated. Right VNS was also performed to ensure adequate nicotinic receptor blockade. Global ARI significantly increased during right VNS before hexamethonium infusion (Fig. 5). After hexamethonium infusion, there was no change in global ARI during right VNS. However, the effects of MCG stimulation after hexamethonium were unchanged, suggesting the presence of predominantly postganglionic sympathetic fibers in the MCG (Fig. 5). H399 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY Table 3. Hemodynamic parameters in infarcted animals BL (PreBSGS) BSGS BL (PreBMCGS) BMCGS (PreCSD) PreCSD BL (PreMCGS PostCSD) PostCSD HR, bpm 85 ⫾ 10.7 94 ⫾ 21* 84 ⫾ 11.8 112 ⫾ 22*§ 83 ⫾ 13 84 ⫾ 13 84 ⫾ 13 1,246 ⫾ 390 2,127 ⫾ 315* 1,123 ⫾ 332 2271 ⫾ 9678*† 984 ⫾ 349 880 ⫾ 337 878 ⫾ 338 dP/dtmax, mmHg/s ⫺1,090 ⫾ 571 ⫺1,025 ⫾ 634 ⫺1,027 ⫾ 630 dP/dtmin, mmHg/s ⫺1,280 ⫾ 582 ⫺1,157 ⫾ 542 ⫺1,179 ⫾ 537 ⫺1,093 ⫾ 635 LVESP, mmHg 90 ⫾ 20 123 ⫾ 28 86 ⫾ 21 99 ⫾ 21§ 78 ⫾ 25 69 ⫾ 22‡ 69 ⫾ 22 BMCGS (PostCSD) 114 ⫾ 24* 1797 ⫾ 937* ⫺958 ⫾ 574 86 ⫾ 26 Values represent mean ⫾ SD % change in parameters from prestimulation value (n ⫽ 12). PostCSD values represent hemodynamic parameters after a 30-min period of stabilization after removal of stellate ganglia. PreCSD represents hemodynamic values immediately before removal of the stellate ganglia. HR, heart rate; dP/dtmax, dP/dtmin, maximum and minimum dP/dt; LVESP, left ventricular end-systolic pressure; BSGS, bilateral stellate ganglion stimulation; BMCGS, bilateral middle cervical ganglion stimulation. *P value ⬍ 0.05 for % change from baseline (prestimulation). †P ⫽ 0.06 for % increase in dP/dtmax with BMCGS compared with BSGS. ‡P ⫽ 0.02 for comparison of PreCSD vs. PostCSD. §P ⬍ 0.01 for comparison of BMCGS vs. BSGS. A glion stimulation (MCG stimulation: 24.7 ⫾ 3.5% vs. stellate stimulation: 12.0 ⫾ 2.8%; P ⫽ 0.02; Fig. 6) The increase in HR was also greater during bilateral MCG stimulation compared with bilateral stellate ganglion stimulation (Table 3), LAD Global ARI (ms) 400 350 300 250 PreCSD PostCSD 444 432 421 409 397 385 374 362 350 339 327 315 ARI (ms) P < 0.05 LV Pre-CSD LAD RV VT/VF Inducibility (%) P < 0.05 0.05 B RV 60 40 20 0 LV Pre-CSD Post-CSD Post-CSD C Post-CSD Pre-CSD 500ms 500ms III II V1 V1 V3 V3 RVD RVD RVP RVP Fig. 7. Effects of CSD and VT inducibility before and after CSD. A: epicardial global ARI from infarcted animals significantly increased with CSD (n ⫽ 12). Blue dashed circle indicates region of the infarct on polar maps. B: inducibility of VT/VF was reduced after CSD in infarcted animals (n ⫽ 18: 12 were inducible at baseline; of these 12 only 6 were inducible after CSD). C: example of VT induction with ventricular extrastimulus pacing. VT/VF was induced before CSD with double extrastimuli at cycle lengths of 600/320/200 ms. After CSD, ERP was reached at an interval of 600/340 ms with double extrastimuli. Therefore, the S2 stimulus was increased by 20 ms to 600/360 ms (to allow for consistent capture) and S3 was added and the interval reduced by 10 ms. The animal reached ERP at 270 ms with triple extrastimuli (S3). Therefore, the S3 coupling interval was increased to 290 ms (to allow for consistent capture), and S4 was reduced by 10 ms, starting at 600/360/290/400 ms. Despite reduction of S4 extrastimulus (triple extrastimulus testing) to a coupling interval of 200 ms, no ventricular arrhythmias could be induced. RVD, distal poles of right ventricular endocardial catheter; RVP, proximal poles of right ventricular endocardial catheter. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 Thoracic sympathetic innervation in infarcted hearts. The timeline for the experimental protocol in infarcted animals is shown in Fig. 6. In infarcted animals, changes in ARI were greater during MCG stimulation compared with stellate gan- H400 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY A B INFARCTED HEARTS Post-CSD BMCGS P < 0.01 Percent Change in ARI (%) P = 0.4 Global ARI (ms) 400 350 300 250 200 20 15 10 5 ARI (ms) 0 BMCGS PreCSD LAD LV LV Apex Apex Post-CSD BMCGS Post-CSD PostCSD D Pre-CSD- Infarcted Hearts 1400 Infarcted Hearts Post-CSD – Infarcted Hearts 80 1400 P=0.03 P=0.02 P=0.4 1200 1000 800 600 400 Tp-Te Interval (ms) DOR (ms2) 1200 1000 800 600 400 200 200 BL BMCGS BL BMCGS P<0.05 P=0.01 60 40 20 Percent Change in Tp-Te (%) C DOR (ms2) LAD RV RV 80 60 40 20 0 0 BL BMCGS Pre-CSD BL BMCGS Post-CSD PreCSD PostCSD Fig. 8. MCG stimulation and its effects before and after CSD on infarcted hearts. A: global ARI at baseline (BL) and during bilateral MCG stimulation (BMCGS) after CSD and % change in ARI before vs. after CSD during BMCGS in infarcted hearts (n ⫽ 12). MCG stimulation decreased ARI despite CSD. B: examples of polar maps at baseline and during MCG stimulation after CSD in infarcted hearts. Black dashed lines indicate course of left anterior descending coronary artery (LAD). Blue dashed circle indicates region of scar. C: although MCG stimulation significantly increased DOR before CSD, this effect was mitigated after CSD in infarcted hearts (n ⫽ 12). D: the prolongation in Tp-Te interval during MCG stimulation was reduced by CSD in infarcted hearts. while the increase in LVESP was greater with stellate ganglion stimulation. Finally, the rise in CS NE levels was similar during bilateral MCG and bilateral stellate ganglion stimulation (Table 2). CSD and residual sympathetic innervation in infarcted hearts. In infarcted hearts, CSD led to a prolongation of global ARI (pre-CSD: 385 ⫾ 17 ms vs. post-CSD: 392 ⫾ 17 ms; P ⬍ 0.05; Fig. 7). CSD had no effect on HR or dP/dtmax. However, a decrease in LVESP was observed after CSD in infarcted hearts (P ⫽ 0.02; Table 3). In 66.7% of MI animals (12/18), VT/VF was inducible before CSD. After CSD, VT/VF was inducible in 6 of these 12 animals, reducing VT inducibility by 50% (P ⬍ 0.05; Fig. 7). Of note, the six animals that were not inducible for VT/VF before CSD remained noninducible after CSD. Residual cardiac sympathetic pathways after CSD. In infarcted animals, global ARI continued to decrease during MCG stimulation (Fig. 8). No significant differences in the effects of MCG stimulation on hemodynamic parameters were observed before vs. after CSD (Table 3). Of note, CSD mitigated the increase in DOR during bilateral MCG stimulation in infarcted animals. Before CSD, bilateral MCG stimulation increased DOR by 356 ⫾ 222 ms2 (P ⬍ 0.05; Fig. 8). However, after CSD the increase in DOR with MCG stimulation was no longer significant (Fig. 8). Before CSD, MCG stimulation increased Tp-Te interval from 44 ⫾ 4 ms to 68 ⫾ 7 ms (mean ⫾ SE) in infarcted hearts. After CSD, MCG stimulation increased Tp-Te interval from 44 ⫾ 5 ms to 58 ⫾ 6 ms. Therefore, the percent increase in this interval after CSD during MCG stimulation was significantly reduced (P ⬍ 0.05; Fig. 8). Given that premature ventricular contractions that cause ventricular arrhythmias in infarcted hearts often originate from the myocardium, we qualitatively assessed activation patterns during apical pacing in five infarcted hearts (Fig. 9), which suggested improvement in epicardial conduction/activation and decrease in functional block after CSD, or during MCG stimulation after CSD, in two of the five infarcted hearts. DISCUSSION Major findings. In this study the MCG provided significant innervation to the ventricles, and these sympathetic pathways remained intact in normal and infarcted animals after CSD. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 BL 25 371 353 334 316 298 279 261 243 224 206 187 169 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY A 78 72 66 61 55 49 43 37 32 26 20 14 Pre-CSD Post-CSD AT (ms) 73 67 61 55 48 42 36 30 24 17 11 5 AT (ms) BL Pre-CSD BMCGS Pre-CSD BL Post-CSD BMCGS Post-CSD Fig. 9. Modulation of propagation and activation time by CSD. A: polar maps of activation time/sequence obtained during scar/apical pacing in this infarct animal demonstrated a localized region at the septal border zone of the infarct that was activated late as compared with the surrounding area. This area of functional block (localized regions of late activation, delineated as “II”) before CSD was no longer observed after CSD, and the entire area was activated more homogeneously. B: polar maps of activation time/sequence during scar pacing at baseline (BL) and during bilateral MCG stimulation (BMCGS) before and after CSD in a different infarcted animal. During MCG stimulation, 2 localized regions of late activation are seen at the border zone of the infarct, creating a potential isthmus or area of slow conduction that could serve as the substrate for a reentrant circuits. Both of these regions of late myocardial activation are no longer observed during MCG stimulation after CSD. After CSD, the entire region is more uniformly activated. Black dashed circle indicates region of the infarct on polar maps. Furthermore, bilateral CSD reduced VT inducibility acutely in the setting of chronic MI, without compromising hemodynamic stability, a finding that can have implications for cardiomyopathy patients with recurrent ICD shocks. An important mechanism behind the antiarrhythmic benefit of CSD in infarcted hearts was the mitigation of the effects of sympathetic activation on DOR and on prolongation of Tp-Te interval, a marker of sudden cardiac death. Cardiac sympathetic innervation. Contribution of the MCG to cardiac sympathetic innervation has previously been over- looked. Cardiac neurons that fire in specific phases of the cardiac cycle had been previously described in the MCG (7), but the degree of functional sympathetic innervation to the heart from the MCG was unknown. In this study, the effects of bilateral MCG stimulation in normal hearts were similar to those of bilateral stellate ganglion stimulation. However, in infarcted animals, MCG stimulation led to significantly greater effects on ARI and HR, while stellate ganglion stimulation had greater effects on LVESP. Given multiple other fibers to the head and neck that traverse through the MCG, removal of the MCG, unlike the lower half of stellate ganglia, is not feasible clinically. MCG stimulation continued to show significant cardiac effects after hexamethonium infusion, suggesting that the cardiac neural fibers from the MCG are postganglionic, similar to the stellate ganglia. Antiarrhythmic effects of CSD. Previous reports had shown that left CSD can reduce ischemia-driven ventricular arrhythmias (30, 39). In this study, the rationale for performing bilateral rather than just left CSD was driven by emerging evidence in patients with structural disease and refractory VT/VF. It has been noted that, unlike patients with channelopathies, case series of patients who undergo bilateral CSD for refractory ventricular arrhythmias in the setting of structural heart disease (i.e., MI) have greater VT-free survival compared with patients who undergo left-side-only procedures (43). Furthermore, right stellate ganglion stimulation is also proarrhythmic, increasing DOR (50) and Tp-Te interval, an independent marker of sudden cardiac death in patients (29, 33). Therefore, in this model bilateral CSD was performed both to assess hemodynamic stability after bilateral (rather than just leftsided) CSD and to assess VT inducibility acutely after bilateral CSD. However, acute effects of CSD on ventricular arrhythmias in the setting of a chronic remodeled infarct were unknown. Furthermore, hemodynamic compromise with bilateral CSD remained a concern (43). In this study, hemodynamic parameters were not compromised, while arrhythmia inducibility decreased after CSD. Although this study was performed in the swine model, significant similarities between canine and human autonomic nervous systems exist. As in canines and in humans, the sympathetic chain on each side consists of a superior cervical, a middle cervical, and a stellate ganglion, followed by a ganglion located at the level of each rib (20). As in the canine model, sympathetic stimulation via the stellate ganglion increases DOR (45, 50). Direct and indirect sympathetic activation in humans increases DOR, similar to pigs and dogs (44). Vagal nerve stimulation and decentralization in pigs has effects similar to those in canines (6, 51). Furthermore, we have shown that in the pig, similar to the dog, intrinsic cardiac ganglia remodel in the setting of MI. In addition, pig stellate ganglia show evidence of pathological neural remodeling similar to that in humans in the setting of MI (1, 2). Of note, the cardiac neurons in the MCG were first detected in the canine model (7). The fact that the coronary circulation in the pig is more similar to that in humans (than canine to human) is important in that the scars that are generated in the porcine myocardial infarct model are very similar to scars observed in humans with ischemic cardiomyopathy, carrying the same electrical signature (25). In humans, as in pigs, the right and left stellate ganglia provide significant innervation to the heart (20, 45). AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 B H401 H402 ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY flow could play an important role in the antiarrhythmic benefit of CSD. A framework for the current understanding of the effect of CSD on cardiac neurotransmission via afferent and efferent fibers is shown in Fig. 10. Although CSD prolonged global ARI in infarcted animals, this effect was not observed in normal animals. This may be due to the heightened sympathetic tone and neural remodeling that occurs in infarcted hearts (2), which can be improved by interruption of efferent and afferent fibers through the stellate ganglia and removal of these cardiac neurons. It has been demonstrated both in this infarct model (26) and in patients with ischemic and nonischemic cardiomyopathy that scar regions are rarely composed of homogeneous and dense fibrotic tissue (which would not give rise to any electrical signal) and contain many islands of live myocardium (24, 26, 32, 49). These regions of live myocardium or channels within “scar” give rise to fractionated bipolar electrograms, which have been shown to be good targets of catheter ablation in patients with VT (19, 32, 40). However, these same scar regions with intermingling myocytes have heterogeneous innervation (9, 44) that can lead to regions of delayed activation and conduction block, allowing for reentry and ventricular arrhythmias to occur (3, 34). In this study, we noted that in two animals regions of slow activation along the septal border zones of infarcts were improved after CSD, either at baseline or during MCG stimulation, suggesting that CSD allowed for more uniform cardiac activation, an antiarrhythmic effect. More homogeneous activation could be either due to earlier activation of “late” areas or, more likely, due to slower activation of the surrounding regions as a result of disruption of sympathetic efferent fibers. MCG stimulation after CSD. A theoretical concern with performing bilateral CSD in patients with cardiomyopathy had been the possibility of eliminating sympathetic pathways that may be necessary for day-to-day activities and exercise. In this study, efferent innervation from the MCG remained intact after Brainstem MCG Fig. 10. Efferent and afferent cardiac sympathetic pathways. Afferent fibers from the myocardium that traverse through the MCG pass through the stellate ganglia before reaching the spinal cord, and some of these pathways are interrupted by CSD. In addition, preganglionic efferent fibers that pass from the spinal cord through the stellate ganglia and to the MCG and any postganglionic fibers that arise from the stellate ganglia and innervate the myocardium are also interrupted. However, efferent postganglionic fibers from MCG neurons to the myocardium remain intact despite CSD. Aff, afferent neurons; Eff, efferent neurons; DRG, dorsal root ganglion; IML, intermediolateral nucleus; DH, dorsal horn of the spinal cord. Stellate DRG Eff DH Eff IML Aff Aff DH IML HEART DH IML CSD Pre-ganglionic efferent sympathetic fibers Post-ganglionic efferent sympathetic fibers Afferent sympathetic fibers Intraganglionic Information Processing AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Sympathetic Chain Spinal Cord Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 As in canines, the right stellate ganglion provides predominant innervation to the anterior aspect of the heart and the left stellate ganglion provides innervation to the posterior/ dorsal aspect of the heart (45, 52). As in canines, sympathetic stimulation via the stellate ganglia in pigs increases DOR and predisposes to arrhythmias (28, 50). In addition to interrupting efferent fibers, some of the beneficial effects of CSD are likely due to interruption of afferent neurotransmission. Cardiac sympathetic afferent fibers exist throughout the cardiac chambers and sense mechano-chemical stimuli (22). Disruption of these afferent fibers reduces sympathetic outflow and has been shown to decrease the number of ectopic beats that occur with brief episodes of ischemia (36). Ventricular pacing leads to activation of cardiac mechanoreceptors and increased sympathetic tone, and alteration of processing through the intrinsic cardiac ganglia can be observed (18, 31). Afferent fiber activation subsequently increases sympathetic efferent outflow (37) and can explain the shorter ARIs that were observed with apical ventricular pacing compared with right atrial pacing before CSD, despite a fixed pacing cycle length. This effect was eliminated after CSD. Therefore, a portion of the antiarrhythmic benefit of CSD is likely due to interruption of afferent neurotransmission, which then alters subsequent efferent neurotransmission via the stellate and middle cervical ganglia. Sympathetic activation during VT inducibility testing (18, 35, 42), which by its nature involves ventricular pacing, is reduced by CSD in infarcted hearts, leading to fewer observed arrhythmias. In fact, it has been shown that sympathetic afferent responses to noxious stimuli are enhanced in heart failure dogs and increase renal sympathetic outflow more than in normal animals (48). Furthermore, chemical cardiac sympathetic deafferentation by epicardial application of resiniferatoxin decreases cardiac sympathetic nerve activity and attenuates cardiac remodeling in rats with heart failure (47). Therefore, reduction in afferent transduction leading to decreased efferent out- ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY GRANTS This study was supported by National Heart, Lung, and Blood Institute (NHLBI) Grant 1DP2 HL-132356 and American Heart Association Award 11FTF755004 to M. Vaseghi and NHLBI Grant R01 HL-084261 to K. Shivkumar. DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the author(s). AUTHOR CONTRIBUTIONS T.I., K.Y., D.H., K.N., and M.V. performed experiments; T.I., K.Y., and M.V. analyzed data; T.I., K.Y., and M.V. interpreted results of experiments; T.I. and M.V. prepared figures; T.I. and M.V. drafted manuscript; K.Y., D.H., K.N., K.S., and M.V. approved final version of manuscript; D.H., K.S., and M.V. edited and revised manuscript; M.V. conceived and designed research. REFERENCES 1. Ajijola OA, Wisco JJ, Lambert HW, Mahajan A, Stark E, Fishbein MC, Shivkumar K. Extracardiac neural remodeling in humans with cardiomyopathy. Circ Arrhythm Electrophysiol 5: 1010 –1116, 2012. doi: 10.1161/CIRCEP.112.972836. 2. Ajijola OA, Yagishita D, Reddy NK, Yamakawa K, Vaseghi M, Downs AM, Hoover DB, Ardell JL, Shivkumar K. Remodeling of stellate ganglion neurons after spatially targeted myocardial infarction: neuropeptide and morphologic changes. Heart Rhythm 12: 1027–1035, 2015. doi:10.1016/j.hrthm.2015.01.045. 3. Allessie MA, Bonke FI, Schopman FJ. Circus movement in rabbit atrial muscle as a mechanism of tachycardia. II. The role of nonuniform recovery of excitability in the occurrence of unidirectional block, as studied with multiple microelectrodes. Circ Res 39: 168 –177, 1976. doi:10.1161/01.RES.39.2.168. 4. Antiel RM, Bos JM, Joyce DD, Owen HJ, Roskos PL, Moir C, Ackerman MJ. Quality of life after videoscopic left cardiac sympathetic denervation in patients with potentially life-threatening cardiac channelopathies/cardiomyopathies. Heart Rhythm 13: 62–69, 2016. doi:10.1016/j. hrthm.2015.09.001. 5. Ardell JL, Cardinal R, Beaumont E, Vermeulen M, Smith FM, Armour JA. Chronic spinal cord stimulation modifies intrinsic cardiac synaptic efficacy in the suppression of atrial fibrillation. Auton Neurosci 186: 38 –44, 2014. doi:10.1016/j.autneu.2014.09.017. 6. Ardell JL, Rajendran PS, Nier HA, KenKnight BH, Armour JA. Central-peripheral neural network interactions evoked by vagus nerve stimulation: functional consequences on control of cardiac function. Am J Physiol Heart Circ Physiol 309: H1740 –H1752, 2015. doi:10.1152/ ajpheart.00557.2015. 7. Armour JA. Activity of in situ middle cervical ganglion neurons in dogs, using extracellular recording techniques. Can J Physiol Pharmacol 63: 704 –716, 1985. doi:10.1139/y85-116. 8. Bachmann TN, Skov MW, Rasmussen PV, Graff C, Pietersen A, Lind B, Struijk JJ, Olesen MS, Haunso S, Kober L, Svendsen JH, Holst AG, Nielsen JB. Electrocardiographic Tpeak-Tend interval and risk of cardiovascular morbidity and mortality: results from the Copenhagen ECG study. Heart Rhythm 13: 915–924, 2016.10.1016/j.hrthm.2015.12.027. 9. Barber MJ, Mueller TM, Henry DP, Felten SY, Zipes DP. Transmural myocardial infarction in the dog produces sympathectomy in noninfarcted myocardium. Circulation 67: 787–796, 1983. doi:10.1161/01.CIR.67.4. 787. 10. Beam DM, Neto-Neves EM, Stubblefield WB, Alves NJ, Tune JD, Kline JA. Comparison of isoflurane and ␣-chloralose in an anesthetized swine model of acute pulmonary embolism producing right ventricular dysfunction. Comp Med 65: 54 –61, 2015. 11. Beaumont E, Salavatian S, Southerland EM, Vinet A, Jacquemet V, Armour JA, Ardell JL. Network interactions within the canine intrinsic cardiac nervous system: implications for reflex control of regional cardiac function. J Physiol 591: 4515–4533, 2013. doi:10.1113/jphysiol.2013. 259382. 12. Buckley U, Yamakawa K, Takamiya T, Andrew Armour J, Shivkumar K, Ardell JL. Targeted stellate decentralization: implications for sympathetic control of ventricular electrophysiology. Heart Rhythm 13: 282–288, 2016. doi:10.1016/j.hrthm.2015.08.022. 13. Bunch TJ, Hohnloser SH, Gersh BJ. Mechanisms of sudden cardiac death in myocardial infarction survivors: insights from the randomized trials of implantable cardioverter-defibrillators. Circulation 115: 2451– 2457, 2007. doi:10.1161/CIRCULATIONAHA.106.683235. 14. Cesario DA, Vaseghi M, Boyle NG, Fishbein MC, Valderrábano M, Narasimhan C, Wiener I, Shivkumar K. Value of high-density endocardial and epicardial mapping for catheter ablation of hemodynamically unstable ventricular tachycardia. Heart Rhythm 3: 1–10, 2006. doi:10. 1016/j.hrthm.2005.10.015. 15. Chen PS, Chen LS, Cao JM, Sharifi B, Karagueuzian HS, Fishbein MC. Sympathetic nerve sprouting, electrical remodeling and the mecha- AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 CSD, and CSD did not lead to any hemodynamic compromise in the porcine model. Stellate ganglion stimulation has been reported to increase DOR and Tp-Te interval (45, 50). Tp-Te interval represents both transmural and whole heart DOR and increases the risk of sudden cardiac death (8, 27, 33). In this study, MCG stimulation also increased DOR and Tp-Te interval in infarcted hearts. Importantly, CSD mitigated the effects of MCG stimulation on DOR and Tp-Te interval in the setting of chronic MI, a novel finding of this study. The electrical stability that results from CSD in infarcted hearts during sympathetic activation and the lack of hemodynamic compromise is reassuring. Limitations. Electrograms were recorded only from ventricular epicardium. Therefore, intramural and endocardial effects were not assessed. This study was performed in a porcine model, and given interspecies differences direct interpolation to humans requires additional studies. In addition, isoflurane, which can suppress autonomic activity, was used for general anesthesia during the surgical portion of the protocol. However, anesthesia was switched to ␣-chloralose during the stimulation and CSD portions of the protocol. In addition, ARI and Tp-Te interval were not corrected for increases in HR. Therefore, increases in Tp-Te interval observed with stimulation are likely a conservative estimate of the actual effects. Given different stimulation currents to achieve the same hemodynamic threshold, direct comparison of parameters in MI vs. normal hearts was not performed. However, stimulation currents for right and left stellate ganglia vs. MCG were similar. Finally, direct comparison of ARI values at baseline or after CSD in infarcted compared with normal hearts cannot be made, as normal animals did not undergo a sham MI procedure, did not have VT inducibility testing, and had an additional bilateral stellate ganglion and MCG stimulation where the time courses of effects of bilateral stellate ganglion stimulation and MCG stimulation were compared. Finally, VT inducibility was not tested during MCG stimulation. However, VT inducibility, by the nature of its ventricular pacing, does cause sympathetic activation (18, 35, 42), suggesting that the beneficial effects of CSD are most influential during a state of elevated sympathetic tone. Conclusions. Both MCG and stellate ganglia contribute significantly to cardiac sympathetic innervation. In addition, VT inducibility in animals with chronic MI is significantly reduced by bilateral CSD, even acutely. A mechanism for this benefit is the improvement in the increase in DOR and Tp-Te interval prolongation observed with sympathetic activation. Furthermore, efferent innervation via the MCG remains intact after bilateral CSD and hemodynamic parameters remain stable. H403 H404 16. 17. 18. 19. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. nisms of sudden cardiac death. Cardiovasc Res 50: 409 –416, 2001. doi:10.1016/S0008-6363(00)00308-4. de Bakker JM, van Capelle FJ, Janse MJ, Tasseron S, Vermeulen JT, de Jonge N, Lahpor JR. Slow conduction in the infarcted human heart. “Zigzag” course of activation. Circulation 88: 915–926, 1993. doi:10. 1161/01.CIR.88.3.915. De Ferrari GM, Dusi V, Spazzolini C, Bos JM, Abrams DJ, Berul CI, Crotti L, Davis AM, Eldar M, Kharlap M, Khoury A, Krahn AD, Leenhardt A, Moir CR, Odero A, Olde Nordkamp L, Paul T, Rosés I Noguer F, Shkolnikova M, Till J, Wilde AA, Ackerman MJ, Schwartz PJ. Clinical management of catecholaminergic polymorphic ventricular tachycardia: the role of left cardiac sympathetic denervation. Circulation 131: 2185–2193, 2015. doi:10.1161/CIRCULATIONAHA.115.015731. Herre JM, Thames MD. Responses of sympathetic nerves to programmed ventricular stimulation. J Am Coll Cardiol 9: 147–153, 1987. doi:10.1016/S0735-1097(87)80093-1. Jaïs P, Maury P, Khairy P, Sacher F, Nault I, Komatsu Y, Hocini M, Forclaz A, Jadidi AS, Weerasooryia R, Shah A, Derval N, Cochet H, Knecht S, Miyazaki S, Linton N, Rivard L, Wright M, Wilton SB, Scherr D, Pascale P, Roten L, Pederson M, Bordachar P, Laurent F, Kim SJ, Ritter P, Clementy J, Haïssaguerre M. Elimination of local abnormal ventricular activities: a new end point for substrate modification in patients with scar-related ventricular tachycardia. Circulation 125: 2184 –2196, 2012. doi:10.1161/CIRCULATIONAHA.111.043216. Kawashima T. Anatomy of the cardiac nervous system with clinical and comparative morphological implications. Anat Sci Int 86: 30 –49, 2011. doi:10.1007/s12565-010-0096-0. Kostreva DR, Armour JA, Bosnjak ZJ. Metabolic mapping of a cardiac reflex mediated by sympathetic ganglia in dogs. Am J Physiol Regul Integr Comp Physiol 249: R317–R322, 1985. Malliani A, Recordati G, Schwartz PJ. Nervous activity of afferent cardiac sympathetic fibres with atrial and ventricular endings. J Physiol 229: 457–469, 1973. doi:10.1113/jphysiol.1973.sp010147. Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation 101: 1288 –1296, 2000. doi:10.1161/01.CIR.101.11.1288. Nakahara S, Tung R, Ramirez RJ, Gima J, Wiener I, Mahajan A, Boyle NG, Shivkumar K. Distribution of late potentials within infarct scars assessed by ultra high-density mapping. Heart Rhythm 7: 1817– 1824, 2010. doi:10.1016/j.hrthm.2010.07.032. Nakahara S, Tung R, Ramirez RJ, Michowitz Y, Vaseghi M, Buch E, Gima J, Wiener I, Mahajan A, Boyle NG, Shivkumar K. Characterization of the arrhythmogenic substrate in ischemic and nonischemic cardiomyopathy implications for catheter ablation of hemodynamically unstable ventricular tachycardia. J Am Coll Cardiol 55: 2355–2365, 2010. doi:10.1016/j.jacc.2010.01.041. Nakahara S, Vaseghi M, Ramirez RJ, Fonseca CG, Lai CK, Finn JP, Mahajan A, Boyle NG, Shivkumar K. Characterization of myocardial scars: electrophysiological imaging correlates in a porcine infarct model. Heart Rhythm 8: 1060 –1067, 2011. doi:10.1016/j.hrthm.2011.02.029. Opthof T, Coronel R, Wilms-Schopman FJ, Plotnikov AN, Shlapakova IN, Danilo P Jr, Rosen MR, Janse MJ. Dispersion of repolarization in canine ventricle and the electrocardiographic T wave: Tp-e interval does not reflect transmural dispersion. Heart Rhythm 4: 341–348, 2007. doi:10.1016/j.hrthm.2006.11.022. Opthof T, Misier AR, Coronel R, Vermeulen JT, Verberne HJ, Frank RG, Moulijn AC, van Capelle FJ, Janse MJ. Dispersion of refractoriness in canine ventricular myocardium. Effects of sympathetic stimulation. Circ Res 68: 1204 –1215, 1991. doi:10.1161/01.RES.68.5.1204. Panikkath R, Reinier K, Uy-Evanado A, Teodorescu C, Hattenhauer J, Mariani R, Gunson K, Jui J, Chugh SS. Prolonged Tpeak-to-Tend interval on the resting ECG is associated with increased risk of sudden cardiac death. Circ Arrhythm Electrophysiol 4: 441–447, 2011. doi:10. 1161/CIRCEP.110.960658. Puddu PE, Jouve R, Langlet F, Guillen JC, Lanti M, Reale A. Prevention of postischemic ventricular fibrillation late after right or left stellate ganglionectomy in dogs. Circulation 77: 935–946, 1988. doi:10. 1161/01.CIR.77.4.935. Rajendran PS, Nakamura K, Ajijola OA, Vaseghi M, Armour JA, Ardell JL, Shivkumar K. Myocardial infarction induces structural and functional remodelling of the intrinsic cardiac nervous system. J Physiol 594: 321–341, 2016. doi:10.1113/JP271165. 32. Reddy VY, Wrobleski D, Houghtaling C, Josephson ME, Ruskin JN. Combined epicardial and endocardial electroanatomic mapping in a porcine model of healed myocardial infarction. Circulation 107: 3236 –3242, 2003. doi:10.1161/01.CIR.0000074280.62478.E1. 33. Rosenthal TM, Stahls PF 3rd, Abi Samra FM, Bernard ML, Khatib S, Polin GM, Xue JQ, Morin DP. T-peak to T-end interval for prediction of ventricular tachyarrhythmia and mortality in a primary prevention population with systolic cardiomyopathy. Heart Rhythm 12: 1789 –1797, 2015. doi:10.1016/j.hrthm.2015.04.035. 34. Rutherford SL, Trew ML, Sands GB, LeGrice IJ, Smaill BH. Highresolution 3-dimensional reconstruction of the infarct border zone: impact of structural remodeling on electrical activation. Circ Res 111: 301–311, 2012. doi:10.1161/CIRCRESAHA.111.260943. 35. Schwartz L, Sole MJ, Vaughan-Neil EF, Hussain NM. Catecholamines in coronary sinus and peripheral plasma during pacing-induced angina in man. Circulation 59: 37–43, 1979. doi:10.1161/01.CIR.59.1.37. 36. Schwartz PJ, Foreman RD, Stone HL, Brown AM. Effect of dorsal root section on the arrhythmias associated with coronary occlusion. Am J Physiol 231: 923–928, 1976. 37. Schwartz PJ, Pagani M, Lombardi F, Malliani A, Brown AM. A cardiocardiac sympathovagal reflex in the cat. Circ Res 32: 215–220, 1973. doi:10.1161/01.RES.32.2.215. 38. Schwartz PJ, Priori SG, Cerrone M, Spazzolini C, Odero A, Napolitano C, Bloise R, De Ferrari GM, Klersy C, Moss AJ, Zareba W, Robinson JL, Hall WJ, Brink PA, Toivonen L, Epstein AE, Li C, Hu D. Left cardiac sympathetic denervation in the management of high-risk patients affected by the long-QT syndrome. Circulation 109: 1826 –1833, 2004. doi:10.1161/01.CIR.0000125523.14403.1E. 39. Schwartz PJ, Stone HL. Left stellectomy in the prevention of ventricular fibrillation caused by acute myocardial ischemia in conscious dogs with anterior myocardial infarction. Circulation 62: 1256 –1265, 1980. doi:10. 1161/01.CIR.62.6.1256. 40. Soejima K, Suzuki M, Maisel WH, Brunckhorst CB, Delacretaz E, Blier L, Tung S, Khan H, Stevenson WG. Catheter ablation in patients with multiple and unstable ventricular tachycardias after myocardial infarction: short ablation lines guided by reentry circuit isthmuses and sinus rhythm mapping. Circulation 104: 664 –669, 2001. doi:10.1161/hc3101. 093764. 41. St John Sutton M, Lee D, Rouleau JL, Goldman S, Plappert T, Braunwald E, Pfeffer MA. Left ventricular remodeling and ventricular arrhythmias after myocardial infarction. Circulation 107: 2577–2582, 2003. doi:10.1161/01.CIR.0000070420.51787.A8. 42. Taylor JA, Morillo CA, Eckberg DL, Ellenbogen KA. Higher sympathetic nerve activity during ventricular (VVI) than during dual-chamber (DDD) pacing. J Am Coll Cardiol 28: 1753–1758, 1996. doi:10.1016/ S0735-1097(96)00389-0. 43. Vaseghi M, Gima J, Kanaan C, Ajijola OA, Marmureanu A, Mahajan A, Shivkumar K. Cardiac sympathetic denervation in patients with refractory ventricular arrhythmias or electrical storm: intermediate and long-term follow-up. Heart Rhythm 11: 360 –366, 2014. doi:10.1016/j. hrthm.2013.11.028. 44. Vaseghi M, Lux RL, Mahajan A, Shivkumar K. Sympathetic stimulation increases dispersion of repolarization in humans with myocardial infarction. Am J Physiol Heart Circ Physiol 302: H1838 –H1846, 2012. doi:10.1152/ajpheart.01106.2011. 45. Vaseghi M, Yamakawa K, Sinha A, So EL, Zhou W, Ajijola OA, Lux RL, Laks M, Shivkumar K, Mahajan A. Modulation of regional dispersion of repolarization and T-peak to T-end interval by the right and left stellate ganglia. Am J Physiol Heart Circ Physiol 305: H1020 –H1030, 2013. doi:10.1152/ajpheart.00056.2013. 46. Vaseghi M, Zhou W, Shi J, Ajijola OA, Hadaya J, Shivkumar K, Mahajan A. Sympathetic innervation of the anterior left ventricular wall by the right and left stellate ganglia. Heart Rhythm 9: 1303–1309, 2012. doi:10.1016/j.hrthm.2012.03.052. 47. Wang HJ, Wang W, Cornish KG, Rozanski GJ, Zucker IH. Cardiac sympathetic afferent denervation attenuates cardiac remodeling and improves cardiovascular dysfunction in rats with heart failure. Hypertension 64: 745–755, 2014. doi:10.1161/HYPERTENSIONAHA.114.03699. 48. Wang W, Zucker IH. Cardiac sympathetic afferent reflex in dogs with congestive heart failure. Am J Physiol Regul Integr Comp Physiol 271: R751–R756, 1996. 49. Watanabe A, Seki A, Fishbein MC, Shivkumar K, Vaseghi M. Arrhythmogenic right ventricular cardiomyopathy: electroarchitecture of the AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 20. ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY ANTIARRHYTHMIC MECHANISM OF BILATERAL STELLECTOMY substrate. HeartRhythm Case Rep 2: 47–51, 2016. doi:10.1016/j.hrcr. 2015.09.004. 50. Yagishita D, Chui RW, Yamakawa K, Rajendran PS, Ajijola OA, Nakamura K, So EL, Mahajan A, Shivkumar K, Vaseghi M. Sympathetic nerve stimulation, not circulating norepinephrine, modulates T-peak to T-end interval by increasing global dispersion of repolarization. Circ Arrhythm Electrophysiol 8: 174 –185, 2015. doi:10.1161/CIRCEP.114.002195. 51. Yamakawa K, Rajendran PS, Takamiya T, Yagishita D, So EL, Mahajan A, Shivkumar K, Vaseghi M. Vagal nerve stimulation activates vagal afferent fibers that reduce cardiac efferent parasympathetic H405 effects. Am J Physiol Heart Circ Physiol 309: H1579 –H1590, 2015. doi:10.1152/ajpheart.00558.2015. 52. Yanowitz F, Preston JB, Abildskov JA. Functional distribution of right and left stellate innervation to the ventricles. Production of neurogenic electrocardiographic changes by unilateral alteration of sympathetic tone. Circ Res 18: 416 –428, 1966. doi:10.1161/01.RES.18.4.416. 53. Zhou S, Jung BC, Tan AY, Trang VQ, Gholmieh G, Han SW, Lin SF, Fishbein MC, Chen PS, Chen LS. Spontaneous stellate ganglion nerve activity and ventricular arrhythmia in a canine model of sudden death. Heart Rhythm 5: 131–139, 2008. doi:10.1016/j.hrthm.2007.09.007. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 14, 2017 AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00644.2016 • www.ajpheart.org