Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
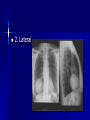
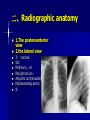
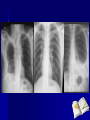
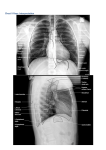
Part 3 How to read a chest X-ray HU 胡春峰 chunfeng Including: The standard CXR projections Normal radiographic anatomy Assessment of a few important techniqual aspects Common radiographic findings and patterns Differential diagnosis 一、Projections performed 1.The posteroanterior(PA) erect diagram Why? Accurate assessment of cardiac size as a result of minimal magnification . Scapulae can be rotated out of the way. Why? Physiological representation of blood vessels of mediastinum and lung. Gas passes upwards (pneumothorax, free gas beneath diaphragm) Fluid passes downwards (pleural effusion) 2. Lateral Why? Further view of lungs, especially those areas obscured on the PA film. Further assessment of cardiac configuration. Further anatomical localization of lesions. More sensitive for pleural effusions Good view of thoracic spine 二、Radiographic anatomy 1.The posteroanterior view 2.the lateral view Tr (trachea) SVC RH(hilum) , LH RA(right atrium) AA(aortic arch/knuckle) DA(descending aorta) St 3.Diagnostic assessment of the CXR Accurate interpretation of the CXR may be difficult or impossible in the absence of relevant and accurate clinical information. PA and lateral film (several important aspects) ①Lung fields: these should be of equal transradiancy and one should not be any whiter or darker than the other. Look particularly at difficult areas where lesions are easily missed: Behind the heart Behind each hilum Behind the diaphragms Lung apics ②Look at the hilum. The left hilum should be higher than right though the difference should be less than 2.5cm. Compare the shape and density of the hila. They should be concave in shape and look similar to each other. The hilum is formed by main bronchi, pulmonary artery and their lobar divisions. ③look at the heart Check that the heart is of a normal shape and that the maximum diameter is less than half of the transthoracic diameter. Check that there are no abnormally dense areas of the heart shadow. CARDIAC POSITION The apex is directed towards the patient’s left chest wall Malpositioned too far to the left by collapse of the left lung or by a space-occupying process (i.e. tension pneumothorax or a large pleural effusion) on the right. pulled to the right by right-sided collapse or by a leftsided space-occupying process. Dextrocardia refers to reversal of the normal orientation of the heart with the cardiac apex directed to the patient’s right. Dextrocardia with the gastric bubble lying beneath the right diaphragm CARDIAC SIZE The cardiothoracic ratio (CTR) is the ratio between maximum transverse diameter of the heart and the maximum transverse diameter of the chest. a CTR of greater than 0.5 indicates cardiac enlargement The cardiothoracic ratio (CTR) is less than 0.5 ④check the rest of the mdiastinum The edge of the mediastinum should be clear though some fuzziness is acceptable at the angle between the heart and the diaphragm, the apices and the right hilum. A fuzzy edge to any other parts of the mediastinum suggests a problem with the neighbouring lung(either collapse or consolidation). ⑤look at the diaphragms The right diaphragm should be higher than the left and this can be remembered by thinking of the heart pushing the left diaphragm down. The difference should be less than 1.2 inch/3cm. The outline of the diaphragm should be smooth. The highest point of the right diaphragm should be in the middle of the right lung field and the highest point of the left diaphragm slightly more lateral. ⑥look specifically at the costophrenic angle They should be well-defined acute angles. Posterior costophrenic angle: very small pleural effusions are seen with greater sensitivity than on the PA film ⑦look at the trachea This should be central but deviates slightly to the right around the aortic knuckle. If the trachea has been shifted it suggests a problem within the mediastinum or pathology within one of the lungs. ⑧look at the bones and chest wall Look at the ribs, scapulae, clavicles, sternum and thoracic vertebrae. Follow the edges of each individual bone to look for fracture. Look for areas of blackness within each bone and compare the density of the bones which should be the same on both sides. Soft tissues: check that both breast shadows are present or mastectomy ⑨Pleural space: Check around the periphery of each lung in the pleural spaces for pneumothorax, pleural effusion, pleural thickening or calcification. 4.Technical assessment We should assess the technical quality of the PA film before making a diagnostic assessment. The patient should be properly centred on the film. With an adequate inspiration X-ray exposure should be appropriate Degree of inspiration To judge the degree of inspiration, count the number of ribs above the diaphragm. The midpoint of the right hemidiaphragm shuld be between the 5th and 7th ribs anteriorly. The anterior end of the 6th rib should be above the diaphragm as should the posterior end of the 10th rib. If more ribs are visible the patient is hyperinflated. If fewer are visible the patient has not managed a full intake of breath perhaps due to pain, exhaustion or disease. The questions: The standard CXR projections. Do you know what form the hilum?