Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
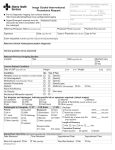
PLACE LABEL HERE PREVENTION OF CONTRAST INDUCED NEPHROPATHY (CIN) ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 1. Weigh patient and record: ______ Kg 2. Procedure Name:__________________________________Date/Time of Procedure:_________/________ 3. If GFR < 30, notify physician to determine if holding contrast or using alternative study without contrast is feasible. MONITORING: 4. Chem-7 daily x 2 days starting day after procedure, unless discharged. 5. Monitor urine output post-procedure x 48 hrs or until discharge. Notify physician if urine output < 250 ml per 8 hr shift. HOLD MEDICATIONS: 6. Hold metformin containing medications on day of procedure and resume 48 hrs post-procedure. 7. Hold NSAIDs on day of procedure 8. Hold diuretics on day of procedure 9. Hold other meds on day of procedure: ______________________________________________________ MEDICATIONS: 10. Inpatient Orders: Normal Saline (NS) infusion: Start NS infusion 12 hrs pre-procedure and continue 12 hrs post- procedure at a rate of: 1 ml/kg/hr IV or 0.5 ml/kg/hr IV (for patients with EF < 40% or CHF, max rate 65 ml/hr) (Procedure does not need to be delayed if patient has not completed 12 hrs of pre-procedure IV fluids, however, an additional fluid bolus pre-contrast may be warranted.) 11. Outpatient or Emergent Orders: Normal Saline infusion: Pre-Procedure: 3 ml/kg/hr IV for 1-3 hrs prior to procedure (min of 300 ml pre-procedure is suggested), then Post-Procedure: Decrease rate to: 1.5 ml/kg/hr IV x 4 hrs or 1 ml/kg/hr IV x ____hrs (6-12 hrs depending on deposition) ______________ Date ______________ Time _________________________________ Physician Signature ___________ PID Number Copy to pharmacy *1-18540* FORM 1-18540 REV. 08/2014 Page 1 of 1