Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
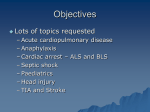
Children’s Hospital of Pittsburgh Guidelines for Clinical Effectiveness Inpatient Sickle Cell Disease Acute Chest Syndrome Guideline Fever, cough, dyspnea, wheezing, chest pain •Begin Pain Management Immediately •Patients should be treated according to their individualized management plan (Refer to ED binder). History Obtain and document associated symptoms Review any oxygen requirement, obtain baseline Oxygen sats. Review history of asthma, current medications, drug allergies Review medical history focusing on sickle cell disease, history of acute chest syndrome and pneumonia Laboratory Evaluation CBC (including WBC diff and platelet) Rapid HgbS level Chemistry profile Liver function tests Type and Screen (sickle cell negative-leukocyte depleted) PRBC’s, Rh (C,E,) and Kell antigen-matched blood. (Patients with prior history of allosensitization should receive PRBCS that are phenotypic ally identical.) • Consider ABG based on clinical condition (Severe hypoxemia PaO2 < 70 mm Hg indicates potentially life-threatening disease.) • • • • • • Transfusion Therapy • Hct < 30 %= Red cell transfusion • Multiple lobe involvement, PaO2 < 70 mm Hg= Perform an exchange transfusion • Early transfusions are indicated for patients at high risk for complications. Monitoring Continuous pulse oximetry Vital signs with blood pressure at least every 4 hours Consider cardio-respiratory monitor if suspect over-sedation Chest x-ray daily Accurate Intake and Output Guideline developed by Lakshmanan Krishnamurti, MD & staff Acute chest syndrome (ACS) is defined by the appearance of a new pulmonary infiltrate on chest X- ray with fever, chest pain or respiratory symptoms (tachypnea, wheezing, cough) Management • • • • • • • • • Oxygen to maintain sats ≥ 94% Bronchodilators Chest X-ray daily and with clinical deterioration Incentive spirometry every 2 hours while awake, every 4 hours while sleeping. Consider chest physiotherapy HCT <30, give simple transfusion –improves survival & multi-lobe involvement. Goal: Hbg 10, HCT 30. ABg<70, perform exchange transfusion – respiratory failure likely Hydration using oral and IV fluids. Total hydration should not exceed 11 ½ times maintenance. I/O and weigh daily Medications • Analgesics for pain control (refer to pain guideline) • Appropriate antibiotic combination of cephalosporin (Ceftriaxone) and macrolide (Azithromycin)- see formulary for dosing details. • Consider adding Vancomycin if clinical deterioration • Continue prophylactic penicillin • Tylenol 10-15 mg/kg/dose for fever • Laxatives for narcotic-induced constipation. • For puritis administer antihistamines such as diphehydramine or hydroxyzine • Antiemetics for nausea Discharge home with previous pain control regime when meets the discharge criteria of: • • • • Sats ≥ 94% on room air or baseline O2 requirement Afebrile for at least 24 hours Adequate oral intake, including medications Adequate pain relief (if needed) with oral analgesics CE # 210.05 Version # 1 Origination: 4/2006 Revised: Next Revision: 2008 This clinical guideline is a collaborative care plan and is not intended to construed or to serve as a standard of medical care. Rather, it is intended as a guideline to promote coordination and communication with respect to patient care and may be modified to meet individual care needs. For additional information contact the Department of Care Coordination at 412/692-7743 ©Children’s Hospital of Pittsburgh, 2006