Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
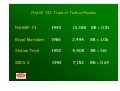
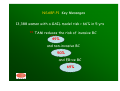
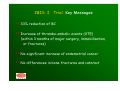
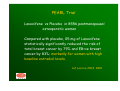
THE RATIONALE AND POTENTIAL OF BREAST CANCER CHEMOPREVENTION IN HIGH RISK WOMEN G. Giardina, L. Bascialla, G. Bini, I. Marcon Oncologia Senologica e Farmacoprevenzione ONCOLOGIA MEDICA - Varese VARESE - 20 gennaio 2012 EPIDEMIOLOGY of Breast Cancer (BC) * The most common cancer in women (45,000 cases/yr) * The second most common cause of death (12,000/yr) * 5%-10% of women who develop BC have a highly penetrance genetic predisposition * BRCA1/2 mutations occur in about one in 250 women * Worldwide incidence and mortality rate in 2008 1,200,000 -- 400,000 * 5 years survival : 85% I numeri del Cancro in Italia-AIOM 2011 INCIDENCE RATE seems levelled MORTALITY RATE has declined since 1990 * early detection * adjuvant therapies * reduction in HRT use * prevention strategies 5 years survival rate (Varese) : 84.3 (Modena 86.9 ; Romagna 85.1 ; Biella 85.9) SEIZING THE OPPORTUNITY Clinicians have long recognised that individuals with a family history of Breast Cancer are themselves at increased risk for developing the disease. The description of kindreds in which there appears to be an autosomal dominant pattern of predisposition (BRCA1,BRCA2) is more recent. The most striking feature of these families is the often marked degree to which the risk is increased and the young ages at which the cancer occur. M.Robson, MSK Cancer Center,2009 Some cancer predisposition syndrome are probably under-recognised, such as Cowden syndrome, which can be highly variable in its presentation. Knowledge of the specific range of cancer risk is crucial to proper women management. R.Dent, Sem. Oncol.,2008 The majority of breast cancer are sporadic, endocrine-responsive (70%) and risk factors are primarily related to OESTROGEN EXPOSURE BRCA 1 and BRCA2 mutations carriers Women with inherit mutations in the BRCA 1 and BRCA2 genes have : * 5-20 fold increased risk ** 45%-65% life-time probabilities for Breast Cancer and *** 11%-40% life-time probabilities for Ovarian cancer A.Curian, JCO, 2011 Pathology of Hereditary BC * BC with BRCA1 germ-line mutations can often be distinguished from non-BRAC1 related BC : TRIPLE NEGATIVE PHENOTYPE * BC associated with BRCA2 germ-line mutations appear to be less specific morphologically W.D. Foulkes, Sem. Oncol. 2007 VARIANT of UNCERTAIN SIGNIFICANCE (VUS) VUS are sequence variations in a gene where the effect of the sequence change on the function of the protein is not known. Between 10% and 15% of individuals undergoing genetic testing for BRCA1/2 mutations will be found to have VUS. S.Domchek,JCO,2008 VUS is a clinically and emotionally difficult situation and advising individuals with VUS on surveillance, prophylactic surgery and chemoprevention is challenging for providers, confusing to families and distressing for everyone. S.Domchek,JCO,2008 LIFE TIME RISK for BC GENERAL POPULATION 12% STRONG FAMILY HISTORY BRCA mutations 85% R.Dent, Sem.Oncol. 2008 Preclinical and epidemiological data indicate that breast cancer can be prevented or, at least significantly delayed. The rationale is based on the hypothesis that the use of natural, synthetic or biological chemical agents can reverse, suppress or prevent either the initial phase of cancerogenesis or the progression of neoplastic cells to cancer. KEY CONCEPT UNDERLYING CHEMOPREVENTION Cancerogenesis is : *MULTISTEP (accumulation of genetic and epigenetic alterations) *MULTIPATH (self-sufficiency in growth signals, insensitivity to antigrowth signals, apoptosis evasion, limitless replicative potential, tissue invasion and sustained angiogenesis) * MULTIFOCAL (multi-clonal : field cancerization clonal : expansion leading to intraepithelial spread) KIND OF CHEMOPREVENTION * PRIMARY : to prevent the onset of disease in healthy individuals at risk * SECONDARY : to treat a population with premalignant condition in order to arrest the developement of cancer * TERTIARY : to protect subjects cured of an initial cancer against second primary tumour INTRAEPITHELIAL NEOPLASIA (IEN) Is a premalignant lesion occurring in most epithelial tissues as moderate to severe dysplasia Phenotype changes (genetic mutations, loss of cellular control functions) early dysplasia severe dysplasia superficial cancer invasive cancer TIME TO PROGRESSION May happen within months to a few years when the process is relatively aggressive, i.e. : * DNA repair-deficient genotype * Viral transformant (HPV) BUT ………… These changes generally appear to occur over A LONG PERIOD OF TIME In BREAST CANCER : atypical hyperplasia ductal intraepithelial neoplasia (DIN or DCIS) lobular intraepithelial neoplasia (LIN or LCIS) invasive cancer REQUIRES 10-20 yrs or more SO ……… Subjects with IEN, particularly severe IEN, are at significantly higher risk than unaffected population and exceeds other measurable risk factors with the exception of germ-line mutations that occur in genetyc syndromes. Selective oestrogen receptor modulators (SERMs) * established role in the treatment and chemoprevention of hormone-related BC * antagonise oestrogens in some tissues and mimic their action in others PHASE III Trials of TAM vs Placebo NSABP- P1 1992 13,388 RR = 0.51 Royal Marsden 1986 2,494 RR = 1.06 Italian Trial 1992 5,408 RR = NS IBIS-I 1992 7,152 RR = 0.67 NSABP-P1 Key Messages 13,388 women with a GAIL model risk > 66% in 5 yrs ** TAM reduces the risk of invasive BC 49% 49% and non-invasive BC 50% 50% and ER+ve BC 69% 69% ** In Lobular carcinoma in situ (LCIS or LIN) 56% 56% ** In Athypical Hyperplasia 86% 86% ** The effect was seen in all age groups ** TAM produced a reduction in osteoporotic fractures 20% 20% However ……… In women aged 50 or older endometrial cancer risk + 4 -fold pulmonary embolism + 3 -fold and a signicant excess of cataract NO EFFECT ON IN ER-ve TUMOURS !!!!!!! NO EFFECT ER-ve TUMOURS IBIS. I Trial Key Messages ** 33% reduction of BC ** Increase of thrombo-embolic events (VTE) (within 3 months of major surgery, immobilisation, or fractures) ** No-significant increase of endometrial cancer ** No differences in bone fractures and cataract ROYAL MARSDEN and ITALIAN Trial ** At a median follow-up of 70 and 81 months no-difference in risk reduction BUT ……… significant reduction in women taking HRT PHASE III Trials of RALOXIFEN MORE Ral vs Plac 7,705 osteop. women RR = 0.24 (no increase of endometrial cancer, VTE = TAM) CORE MORE+4yrs 4,011 osteop. women RR = 0.41 (no increase of endometrial cancer, VTE = TAM) RUTH Ral vs Plac 10,101 CHD women RR = 0.56 STAR Ral vs Tam 19,747 high risk RR = 1.02 (no diffrence between arms : 50% reduction. endometrial cancer 38% lower in Raloxifen arm no protective effect of Ral on non-invasive cancer) MORE, CORE, RUTH, STAR Trial Key Messages ** Raloxifen is a SERM with a marked effect on : - incidence reduction of invasive BC - no effect on non-invasive BC - no increase of endometrial cancer - VTE risk similar to Tamoxifen PEARL Trial Lasoxifene vs Placebo in 8556 postmenopausal osteoporotic women Compared with placebo, 05 mg of Lasoxifene statistically significantly reduced the risk of total breast cancer by 79% and ER+ve breast cancer by 83%; markedly for women with high baseline estradiol levels. A.Z.Lacroix,JNCI, 2010 Other agents ** AROMATASE Inhibithors or Inactivators (data from ATAC, BIG-1, IES, ARNO Trials) - lower risk of controlateral BC - lack of increase in VTE and endometrial cancer - increase in risk of osteoporosis and fractures Ongoing Trials : IBIS-II (prevention/DCIS) NCIC-MAP.3 ** NON STEROIDAL ANTI-INFLAMMATORY DRUGS Epidemiological studies have produced mixed results and a direct relationship cannot be demonstrated yet Evidence for an interaction of genetic polymorphism of COX-2 (allele 8473) with NSAIDs to reduce risk of HR+ve BC has been found in a population-based case-control study. Future research **** Research are needed to identify molecular biomarkers that accurately predict an agent’s cancer incidence-reducing effect ***** Actually, Tamoxifen at lower doses, seems to be a simple and economic approach reducing the risk of HR+ve BC. The rationale is : - binding to HR follows saturation kinetics - 20 mg/day is as effective as 30-40 mg/day - endometrial effect is dose-dependent - animal data show complete inibition at a dose equivalent to 1 mg/day in humans - preoperative trials show similar antiproliferative effects of 1 mg and 5 mg/day compared to 20mg * Most BRCA1 related BC are of Basal Phenotype and are ER-negative, while BRCA2 related BC are much more like sporadic tumors and are frequently ER-positive. * Hence, one might anticipate that hormonal chemoprevention strategies such as Tamoxifen may have more benefit for BRCA2 carriers compared to BRCA1 mutation carriers. E.Rodriquez, Sem.Oncol, 2007 *There are a significant amount of data that hormonal manipulation strategies such as bilateral oophorectomy and Tamoxifen do affect BC risk in BRCA1 carriers. * Future studies will need to stratify for mutation type and include a longer follow-up period, because riskreducing strategies may have different effects in these two related but different cancer susceptibilty syndrome. E.Rodriquez, Sem.Oncol, 2007 STRATEGIES…… nowadays * MRI based screening starting at age 25 yrs * Bilateral salpingo-oophorectomy by age 40 yrs (risk reduction: BC = 50%, Ov. Ca = 80%) * Bilateral Mastectomy (risk reduction: BC > 90%) and CHEMOPREVENTION .. is the future ???? C.Touboul,The Oncologist,2011 FENRETINIDE: background Retinoids regulate cell growth, differentiation and apoptosis. Fenretinide is a synthetic amide derivative of retinoic acid which: * accumulates in the human breast * can selectively induce apoptosis in vitro * has antiangiogenic and antitumor effects * has shown a good toxicity profile in clinical studies RETINOIDS (vitamin-A analogues) data from PHASE III Trial (U.Veronesi et al.) (ER-ve pts.; median follow-up of 15 yrs) 50% reduction in women aged 40 yrs or younger (persistent for 10 yrs after retinoid cessation) U.Veronesi, Ann.Oncol.,2006 INCIDENCE OF SECOND BREAST CANCER PREMOPAUSE ** HR = 0.62 95% C.I. 0.46-0.83 POSTMENOPAUSE ** HR = 1.23 95% C.I. 0.63-2.40 U.Veronesi, Ann.Oncol.,2006 TAKE HOME MESSAGES * Breast Cancer prevention is feasible ** Toxicity concerns strongly affect the acceptability of actually available agents *** Salpingo-oophorectomy/prophylactic mastectomy are effective in BRCA1/2 carriers but the impact on quality of life, body image, sexuality and longterm well-being must be considered prior to surgery. G.Wickman, Breast, 2010 **** Prevention strategies in selected high risk women are needed to make chemoprevention safe and widely used. IL NOSTRO CONTRIBUTO STUDIO TAM-01 (A. DeCensi) - Tamoxifene a basse dosi x 3 anni - Pazienti con DCIS G 1/2 STUDIO “Fenretinide” – IEO (U.Veronesi,B.Bonanni) - Pazienti di età 25/44 anni - Mutazione BRCA1/2 o BRCA-Pro > 20% IBIS- II (Int. Breast Cancer Prevention Study; J. Cuzick) - PREVENTION : Anastrozolo vs Placebo - DCIS : Tamoxifene vs Anastrozolo) Solo insieme possiamo dare il massimo !!!!! grazie per l’attenzione CASO CLINICO F.R.S. , 42 anni mutazione BRCA1 mentre stava pensando di partecipare allo studio IE0 con Fenretinide, esegue controllo MxEco: QSE Dx, nodulo 1.0 cm, FNAC = C 5 cT1b cN0 M0 QUALI OPZIONI HIRURGICHE discutere con la paziente ?????? (TENENDO CONTO CHE LA PROGNOSI NON SEMBRA ESSERE NEGATIVAMENTE INFLUENZATA DA BRCA1 POSITIVITA’ ) P.Goodwin,JCO, 2011 A) MASTECTOMIA bilaterale + salpingoovariectomia riduzione rischio BC > 90% riduzione rischio Ovaio 80% B) MASTECTOMIA monolaterale o QUADRANTECTOMIA + salpingoovariectomia rischio di ricaduta locale eguale (Mastec/Quad +RT) riduzione 50% rischio BC mammella controlaterale con salpingoovariectomia












































![“Basic and translational oncology” [Selezionare la data] Italian](http://s1.studyres.com/store/data/003369983_1-0c2f97f3754c36ff0d6a75a322ab9225-150x150.png)



![Genistein [446-72-0] - Università degli Studi di Roma "Tor Vergata"](http://s1.studyres.com/store/data/001069358_1-826841ed5b5b39775155b3058987503a-150x150.png)