Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
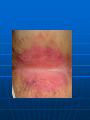
Wow that looks Pretty Bad!! Jai Gilliam, M.D. Internal medicine/Pediatrics Noon Conference 45 yo Caucasian male is coming to see you in clinic for a new rash that has developed over the past 1 month. He says that the rash itches “a lot” and that he has tried multiple over the counter creams but this has provided no relief. He describes the rash as being very dry and that it “peels” a lot. It is localized around his nose, forehead, and involves the lateral aspects of his hair line Seborrhea (Seborrheic dermatitis) Patient will present with generalized, fine, scaling (flaky) rash of the scalp, ear, nose, and occasionally lips. Rash is puritic in nature Treatment: Selenium sulfide shampoo, zinc pyrithione, and Tar What other crucial questions would you ask this patient? Have you ever been tested for HIV ? Mrs. Jackson is being seen in clinic for a “personal matter”. She states that she is really embarrassed about her weight and wants to try to loss some weight. She also would like to talk about a rash that she has had for a long time. She says that it occurs along her skin folds and that it “itches like crazy”. Patient tried some Hydrocortisone cream on the rash but the rash got worse. On her physical exam you see this. Intertrigo Contact irritant dermatitis where candida is a common fungus that causes this rash. Occurs along the folds where there is a lot of moisture making it an ideal location for fungus to grow. Commonly seen in obese patients. Treatment: Make sure that the area is dried especially after showering/bathing. Topical antifunguls and antifungal powder to prevent moisture. Mr. Powers is a 43 yo male who is coming to your clinic because he is concerned about these “Weird” circular rashes on his arm and legs. He describes the lesion as “shiny” and almost like a “irregular circular” pattern. He says that he has had it for the past 6 months but he came in because it just keeps getting worse. He denies any itching and no trauma. You review his medication and he is taking Lipitor, allegra-D, accupril, Glucophage, and glipizide. When you do your physical exam you see this Necrobiosis lipoidica Rash is commonly seen in diabetics 15% Precedes the onset of diabetes 25 % occur at the onset of diabetes 60% will occur in patients already diagnosed Etiology- 3 theories 1. Diabetic microangiopathy secondary to glycoprotien deposition. 2.Vasculitis- secondary to immunoglobulin deposition along with complement/fibrinogen deposits 3. Abnormal Collagen- defective collagen has been seen in other diabetic end organ damage Treatment: Topical & intralesional steroids. ( atrophy of skin), Aspirin & Dipyridamole (Anti-platelet therapy, platelet induced vasocclusion disease. Your next patient is a 28 yo male from the middle east who speaks very little English. He’s at this office visit with his wife who is able to translate. She says that they are being referred to you from another physician. Her concern is that her husband has developed a medium size ulcer on his ankle. It has been there for about 4 months, but it has gotten worse. The wound is now draining purulent discharge. The only other medical issue is that he has been having problems with his “bowels” for which his wife says that he is taking a special medication for his bowel problem. Pyoderma Gangrenosum 2 types: Classic PG- involving primarily the legs. Atypical PG- involves superficial skin, effecting the hands Diagnosis is based on exclusion by history/biopsy- DDx is infection, connective tissue dz, vasculitis, trauma Cause: speculated to be related immune dysregulation Prognosis is good, associated with other systemic dz: IBD, rheumatoid arthritis, chronic hepatitis, Wagener's Treatment: Mild- topical steroid. Moderate-Severe: Oral steroid, cyclosporin, methotrexate, and tacrolimus Mrs.Lenning is a 36 yo female who is bringing her 4month old infant in for well child check. The only concern on this visit is about breast feeding. She claims that she has been having some difficulty with breast feeding. She has noticed that there is a dry rash around her areola on her right breast. She has tried some Hydrocortisone cream on it because she thought it was eczema but the rash did not improve When you do her physical exam you see this Paget’s disease of the breast 1.Eczematous rash is pathoneumonic for the presence of intraepithelial breast adenocarcinoma 2.Diagnosis-confirmed by punch biopsy,showing Paget cells-(adenocarcinoma cells). 3. Prognosis: depends on the stage of disease (+) lymph nodes vs localized disease. 4.Treatment option:masectomy (rarely), breast conserving surgery(nipple-areoloa resection), Conserving surgery + whole breast irradiation provided the lowest % with recurrence You have been consulted to see a 67 yo female S/P right knee replacement for a possible wound infection of the right knee.She is complaining of right knee swelling, tenderness, and skin hyperpigmentation. Her surgery was approx 1 week ago and she is being seen today in Post-op clinic. Her entire post-op course was unremarkable and she has never had this before. Patient denies any trauma to this leg, no fever, no chills, no other systemic symptoms When you do your physical exam you see the following? What questions do you want to know about her post-op course. Where you taking any Coumadin during her recent hospitalization? Coumadin Necrosis Typically presents 7-14 days after administration of coumadin. Caused by Protein C deficiency: Bx will show fibrin thrombi within cutaneous vessels leading to interstitial hemorrhage. Clinically: Rash will develop over the trunk, arms, breast, and penis (common symptom). Treatment: Stop Coumadin, Protein C need to be replaced.(concentrated or FFP), surgical debridement if rapidly progressing necrosis. Once a patient has experienced this drug induced necrosis, Is it safe to try the patient back on Warfarin? Yes, Patient can be placed back on Warfarin but these patient need to be closely monitor. If a patient has previously had a skin reaction to coumadin there is no contraindication for subsequent doses Mr.Lewis is a 34 yo male with Hx of HTN is coming to your clinic for the first time.He is concerned of a small “bump” on his face. He says that it has been there for the past 1 year, but the bump has progressivley gotten worse. He denies any bleeding from the lesion or trauma. Overall, he says he has been healthy but says that for the past 2 month he has really felt very tired and that his “smokers” cough has gotten worse over the same duration. He denies any fever, chills, or wt loss. When you do your physical exam you notice this on his face? Lupus Pernio No relation to SLE, term Lupus= Chronic autoantibody inflammatory disease and Pernio associated with SARCOIDOSIS. 25% of patients with Sarcoidosis will develop some form of skin rash. Biopsy of skin lesion in Sarcoid reveal the classic finding of non-necrotizing granulomas Mimics other disease, systemic involvement: eyes, heart, skin, muscle, CNS, kidney, spleen Treatment: Prednisone and other immunosupresive Anything in the History that you should ask about for this patient? Have You Ever been tested for HIV? Bullous Pemphigoid Pemphigus Vulgaris Starwars Episode III Secrets Revealed Thank You Sources 1 Medstudy: Internal medicine core curriculum section on Dermatology, 11th edition 2005/2006 2.Uptodate 3.Lawrence, Cox Physical signs in Dermatology 2nd edition chapter on hair/scalp disease. Pg 334350. copyright 2002