Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Epidemiology of metabolic syndrome wikipedia , lookup
Public health genomics wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Epidemiology wikipedia , lookup
Preventive healthcare wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
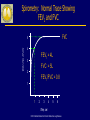
The spectrum of pulmonary diseases Abubakr A Bajwa. MD, FCCP Associate Professor of Medicine Division Chief Pulmonary, Critical Care and Sleep Medicine Director Pulmonary Hypertension and Interstitial Lung Disease Clinic University of Florida College of Medicine/Jacksonville Objectives n n n n Describe the spectrum of common pulmonary diseases Explain physiology of diseases Describe various manifestations Discuss briefly about evaluation and management of various pulmonary disorders Slovenia Germany Brazil Ireland United States Australia Canada Philippines Mongolia Moldova Norway Thailand Kazakhstan United Kingdom Syria Italy New Zealand Argentina Mexico United Arab Emirates Poland Korea Portugal Greece Bangladesh Saudi Arabia Yugoslavia Croatia Austria Taiwan ROC Yeman Malta China South Africa Hong Kong ROC Nepal Chile Israel Pakistan Russia GOLD National Leaders Peru Japan Netherlands Egypt France Venezuela KyrgyzstanGeorgia Macedonia Albania Iceland Denmark Turkey Czech Belgium Slovakia Republic Singapore Spain Columbia Ukraine Romania Sweden Uruguay © 2014 Global Initiative for Chronic Obstructive Lung Disease Vietnam Switzerland India GOLD Website Address http://www.goldcopd.org © 2014 Global Initiative for Chronic Obstructive Lung Disease Confusion Over Pulmonary Diagnosis G lobal Initiative for Chronic O bstructive L ung D isease © 2014 Global Initiative for Chronic Obstructive Lung Disease GOLD Objectives n n Increase awareness of COPD among health professionals, health authorities, and the general public Improve diagnosis, management and prevention n Decrease morbidity and mortality n Stimulate research © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD, 2014: Chapters Updated 2014 n Definition and Overview n Diagnosis and Assessment n Therapeutic Options n Manage Stable COPD n Manage Exacerbations n Manage Comorbidities n Asthma COPD Overlap Syndrome (ACOS) © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD, 2014: Chapters Updated 2014 n Definition and Overview n Diagnosis and Assessment n Therapeutic Options n Manage Stable COPD n Manage Exacerbations n Manage Comorbidities n Asthma COPD Overlap Syndrome (ACOS) © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Definition of COPD n n COPD, a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Mechanisms Underlying Airflow Limitation in COPD Small Airways Disease Parenchymal Destruction • Airway inflammation • Airway fibrosis, luminal plugs • Increased airway resistance • Loss of alveolar attachments • Decrease of elastic recoil AIRFLOW LIMITATION © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Burden of COPD COPD is a leading cause of morbidity and mortality worldwide. The burden of COPD is projected to increase in coming decades due to continued exposure to COPD risk factors and the aging of the world’s population. COPD is associated with significant economic burden. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Risk Factors for COPD Genes Infections Socio-economic status Aging Populations © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD, 2014: Chapters Updated 2014 n Definition and Overview n Diagnosis and Assessment n Therapeutic Options n Manage Stable COPD n Manage Exacerbations n Manage Comorbidities n Asthma COPD Overlap Syndrome (ACOS) © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis and Assessment: Key Points A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and a history of exposure to risk factors for the disease. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis and Assessment: Key Points The goals of COPD assessment are to determine the severity of the disease, including the severity of airflow limitation, the impact on the patient’s health status, and the risk of future events. Comorbidities occur frequently in COPD patients, and should be actively looked for and treated appropriately if present. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis of COPD SYMPTOMS shortness of breath chronic cough sputum EXPOSURE TO RISK FACTORS tobacco occupation indoor/outdoor pollution è SPIROMETRY: Required to establish diagnosis © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of Airflow Limitation: Spirometry Spirometry should be performed after the administration of an adequate dose of a shortacting inhaled bronchodilator to minimize variability. A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation. Where possible, values should be compared to age-related normal values to avoid overdiagnosis of COPD in the elderly. © 2014 Global Initiative for Chronic Obstructive Lung Disease Spirometry: Normal Trace Showing FEV1 and FVC FVC Volume, liters 5 4 FEV1 = 4L 3 FVC = 5L 2 FEV1/FVC = 0.8 1 1 2 3 4 5 6 Time, sec © 2014 Global Initiative for Chronic Obstructive Lung Disease Spirometry: Obstructive Disease Normal 5 Volume, liters 4 3 FEV1 = 1.8L 2 FVC = 3.2L FEV1/FVC = 0.56 1 1 2 3 4 5 6 Time, seconds © 2014 Global Initiative for Chronic Obstructive Lung Disease Obstructive Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD: Goals Determine the severity of the disease, its impact on the patient’s health status and the risk of future events (for example exacerbations) to guide therapy. Consider the following aspects of the disease separately: current level of patient’s symptoms severity of the spirometric abnormality frequency of exacerbations presence of comorbidities. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Symptoms of COPD The characteristic symptoms of COPD are chronic and progressive dyspnea, cough, and sputum production that can be variable from day-to-day. Dyspnea: Progressive, persistent and characteristically worse with exercise. Chronic cough: May be intermittent and may be unproductive. Chronic sputum production: COPD patients commonly cough up sputum. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry COPD Assessment Test (CAT) Assess risk of exacerbations Assess comorbidities or Clinical COPD Questionnaire (CCQ) or mMRC Breathlessness scale © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of Symptoms COPD Assessment Test (CAT): An 8-item measure of health status impairment in COPD (http://catestonline.org). Clinical COPD Questionnaire (CCQ): Self- administered questionnaire developed to measure clinical control in patients with COPD (http://www.ccq.nl). © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of Symptoms Breathlessness Measurement using the Modified British Medical Research Council (mMRC) Questionnaire: relates well to other measures of health status and predicts future mortality risk. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Modified MRC (mMRC)Questionnaire © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Use spirometry for grading severity Assess comorbidities according to spirometry, using four grades split at 80%, 50% and 30% of predicted value © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Classification of Severity of Airflow Limitation in COPD* In patients with FEV1/FVC < 0.70: GOLD 1: Mild FEV1 > 80% predicted GOLD 2: Moderate 50% < FEV1 < 80% predicted GOLD 3: Severe 30% < FEV1 < 50% predicted GOLD 4: Very Severe FEV1 < 30% predicted *Based on Post-Bronchodilator FEV1 © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities Use history of exacerbations and spirometry. Two exacerbations or more within the last year or an FEV1 < 50 % of predicted value are indicators of high risk. Hospitalization for a COPD exacerbation associated with increased risk of death. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Assess Risk of Exacerbations To assess risk of exacerbations use history of exacerbations and spirometry: Two or more exacerbations within the last year or an FEV1 < 50 % of predicted value are indicators of high risk. One or more hospitalizations for COPD exacerbation should be considered high risk. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Combine these assessments for the purpose of improving management of COPD © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD 4 (C) (D) 3 2 (A) (B) 1 or > 1 leading to hospital admission 1 (not leading to hospital admission) 0 CAT < 10 CAT > 10 Symptoms mMRC > 2 mMRC 0–1 Breathlessness © 2014 Global Initiative for Chronic Obstructive Lung Disease (Exacerbation history) ≥2 Risk (GOLD Classification of Airflow Limitation)) Risk Combined Assessment of COPD Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess symptoms first (C) (D) (A) (B) CAT < 10 CAT > 10 Symptoms mMRC 0–1 mMRC > 2 Breathlessness If CAT < 10 or mMRC 0-1: Less Symptoms/breathlessness (A or C) If CAT > 10 or mMRC > 2: More Symptoms/breathlessness (B or D) © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD 4 3 (C) (D) or > 1 leading to hospital admission (B) 1 (not leading to hospital admission) 0 2 (A) 1 CAT < 10 (Exacerbation history) ≥2 Risk (GOLD Classification of Airflow Limitation) Risk Assess risk of exacerbations next If GOLD 3 or 4 or ≥ 2 exacerbations per year or > 1 leading to hospital admission: High Risk (C or D) If GOLD 1 or 2 and only 0 or 1 exacerbations per year (not leading to hospital admission): Low Risk (A or B) CAT > 10 Symptoms mMRC 0–1 mMRC > 2 Breathlessness © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD 4 (C) (D) 3 2 (A) (B) 1 or > 1 leading to hospital admission 1 (not leading to hospital admission) 0 CAT < 10 CAT > 10 Symptoms mMRC > 2 mMRC 0–1 Breathlessness © 2014 Global Initiative for Chronic Obstructive Lung Disease (Exacerbation history) ≥2 Risk (GOLD Classification of Airflow Limitation)) Risk Combined Assessment of COPD Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. One or more hospitalizations for COPD exacerbations should be considered high risk.) Patient Characteristic Spirometric Classification Exacerbations per year CAT mMRC A Low Risk Less Symptoms GOLD 1-2 ≤1 < 10 0-1 B Low Risk More Symptoms GOLD 1-2 ≤1 > 10 >2 C High Risk Less Symptoms GOLD 3-4 >2 < 10 0-1 D High Risk More Symptoms GOLD 3-4 >2 > 10 © 2014 Global Initiative for Chronic Obstructive Lung Disease >2 Global Strategy for Diagnosis, Management and Prevention of COPD Assess COPD Comorbidities COPD patients are at increased risk for: • • • • • • • Cardiovascular diseases Osteoporosis Respiratory infections Anxiety and Depression Diabetes Lung cancer Bronchiectasis These comorbid conditions may influence mortality and hospitalizations and should be looked for routinely, and treated appropriately. © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Differential Diagnosis: COPD and Asthma COPD ASTHMA • Onset in mid-life • Symptoms slowly • • Onset early in life (often childhood) progressive • Symptoms vary from day to day Long smoking history • Symptoms worse at night/early morning • Allergy, rhinitis, and/or eczema also present • Family history of asthma © 2014 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Additional Investigations Chest X-ray: Seldom diagnostic but valuable to exclude alternative diagnoses and establish presence of significant comorbidities. Lung Volumes and Diffusing Capacity: Help to characterize severity, but not essential to patient management. Oximetry and Arterial Blood Gases: Pulse oximetry can be used to evaluate a patient’s oxygen saturation and need for supplemental oxygen therapy. Alpha-1 Antitrypsin Deficiency Screening: Perform when COPD develops in patients of Caucasian descent under 45 years or with a strong family history of COPD. © 2013 Global Initiative for Chronic Obstructive Lung Disease Global Strategy for Diagnosis, Management and Prevention of COPD Additional Investigations Exercise Testing: Objectively measured exercise impairment, assessed by a reduction in self-paced walking distance (such as the 6 min walking test) or during incremental exercise testing in a laboratory, is a powerful indicator of health status impairment and predictor of prognosis. Composite Scores: Several variables (FEV1, exercise tolerance assessed by walking distance or peak oxygen consumption, weight loss and reduction in the arterial oxygen tension) identify patients at increased risk for mortality. © 2013 Global Initiative for Chronic Obstructive Lung Disease Bronchiectasis Abubakr A. Bajwa MD, FCCP Pulmonary, Critical Care, Sleep Medicine Objectives • Recognize bronchiectasis with its pulmonary and systemic manifestations • Review diagnostic evaluation • Review treatment strategies for acute and chronic phase Case 1 • 59 woman with TB in past in her 20s • Now with cough and sputum production since her 40s • 1-2 hospitalizations/yr Case 2 • • • • 24 woman with chronic cough and wheezing Diagnosed with asthma/chronic bronchitis/chronic sinusitis Intermittent treatment with BDs and antibiotics Greenish-yellow phlegm production Case 3 • 71 woman non smoker with chronic cough for 4 years • Persistant cough and 15 lbs weight loss • Sputum has MAI Prevalence of non-CF bronchiectasis Definition • Permanently dilated airways • Result from various processes – Congenital – Post-infectious – Anatomical Other signs • Signet ring • Lack of bronchial tapering Clinical picture • Most common: – Chronic cough – Mucopurulent sputum • Less common: – – – – – – Dyspnea Hemoptysis Chest pain Fever Fatigue Weight loss Bronchiectasis and COPD • Out of 54 stable patients with COPD 50% had bronchiectasis on HRCT – – – – – Mean age 69 Mean FEV1 0.96L More severe exacerbations More bacterial colonizations Increased sputum inflammatory markers Focal bronchiectasis • Post-infectious: – Bacterial – Viral – Tuberculous (MTB, NTM) • Airway obstruction: – Foreign body – Bronchial stricture (RML syndrome) – Endobronchial mass Diffuse bronchiectasis • Post infectious: – Measeles, pertussis – Mycobacterial • Postinflammatory: – Sarcoidosis • Inhalation: – Aspiration – Inhalation injury • Congenital syndromes: – CF – Primary ciliary dyskinesia • Immunodeficiency states: – Immunoglobulin deficiency – HIV • Immune mediated diseases: – ABPA – RA – IBD Natural history • Martinez-Garcia Chest 2007 – Mean age 70, 48.7% males – 52.7 ml decline in FEV1 per year – Faster decline: • Psuedomonas • Frequent exacerbations • Increased inflammatory markers – If in ICU then 40% mortality Transplantation • Royal Brompton Hospital: – 22 patients from 1998-2001 – 1 year survival 68% Pulmonary Manifestations of Connective Tissue Diseases Abubakr A Bajwa MD Pulmonary , Critical Care and Sleep Medicine Types of Pulmonary Manifestations Pulmonary Vascular and Alveolar HGE syndromes Interstitial Pleural Airway 1. Vascular Pulmonary Arterial Hypertension Alveolar Hemorrhage Syndrome/Vasculitis/Capillaritis Pulmonary Arterial Hypertension Pathogenesis RISK FACTORS AND ASSOCIATED CONDITIONS VASCULAR INJURY Endothelial Dysfunction Collagen Vascular Disease Congenital Heart Disease Portal Hypertension HIV Infection SUSCEPTIBILITY Drugs and Toxins Abnormal BMPR2 Gene Pregnancy Loss of Response to Short-Acting Vasodilator Trial ↓Nitric Oxide Synthase ↓Prostacyclin Production ↑Thromboxane Production ↑Endothelin 1 Production Other Genetic Factors Smooth Muscle Hypertrophy Vascular Smooth Muscle Dysfunction Impaired Voltage-Gated Potassium Channel (KV1.5) Adventitia Smooth Muscle Hypertrophy Media DISEASE PROGRESSION In Situ Thrombosis Intima Early Intimal Proliferation Plexiform Lesion Vasoconstriction NORMAL Adapted from Gaine S. JAMA. 2000;284:3160-3168. Adventitial and Intimal Proliferation REVERSIBLE DISEASE Advanced Vascular Lesion IRREVERSIBLE DISEASE Limited scleroderma (CREST) Most common Prevalence of PH, ranging from 4.9% to 38% with a mean 16% PH is the cause of death in up to 50% of patients Diffuse scleroderma Less common Often seen with patients with the nucleolar antibody, anti-U3-RNP REVEAL Database: Most Frequent Symptoms at Diagnosis 11% 11% 13% 13.0% 14% 16.0% 20% 23.0% 20% 21.0% 20% 23% 27% 24.0% 29% 26.0% Dyspnea at rest Cough Dizzy/lightheaded Presyncope/syncope Edema Chest pain/discomfort Other Fatigue IPAH APAH n = 1479 83% 84.0% Dyspnea on exertion 0 Elliott EG, et al. Chest. 2007;132(4 suppl):631S. 25 50 75 Incidence (%) 100 PAH Disease Progression: Prognostic Factors for Risk Lower Risk No Higher Risk Yes Progression Gradual Rapid WHO Class II, III IV 6-minute walk distance > 380 m < 325 m Brain natriuretic peptide < 180 pg/mL Minimal right ventricular dysfunction > 180 pg/mL Pericardial effusion; significant right ventricular dysfunction Normal/near normal RAP (< 12 mm Hg) and CI (> 2.5 L/min/m2) High RAP, Low CI Evidence of RV failure Echo findings Hemodynamics McLaughlin VV, et al. Circulation. 2006;114:1417-1431. DAH /Vasculitis/Capillaritis Definitions Diffuse alveolar hemorrhage Syndrome of diffuse bleeding into the lungs at the alveolar level Histopathologically - flooding of alveoli with RBCs Pulmonary Vasculitis Histopathologic occurrence of vasculitis occurring at any level of the pulmonary vasculature Pulmonary Capillaritis Histopathologic occurrence of vasculitis occurring at the capillary/alveolar level DAH DAH is a Syndrome, not a diagnosis A search for underlying cause is imperative Fluminant presentations are frequent Should always be considered life threatening Symptoms Dyspnea and cough Hemoptysis (absent in up to 1/3) Fever usually due to underlying illness Findings Anemia (if chronic or subacute) Hypoxemia DAH - radiographs Bilateral alveolar infiltrates Can start unilateral Can be patchy in more sub-acute presentations A consideration of possible causes… Exposures Trimellitic anhydride, pyromellitic dianhydrate, crack cocaine, smoking, … Abciximab, penicillamine, sirolimus … Underlying diseases / conditions Autoimmune / rheumatologic conditions Cardiac disease – e.g. mitral stenosis Coagulopathy (severe and rare as isolated cause) Post-trauma Recent BMT or hematologic malignancies Immunosuppression Endobronchial bleed Treatment Concepts Stabilization of respiratory status Exclusion of infection Confirmation of DAH Identification of contributing comorbidities or underlying systemic disorders Timely implementation of therapy Treatment concepts Autoimmune / Vasculitic processes Induction of remission… Maintenance of remission… Methotrexate Azathioprine Mycophenolate mofetil 2. Interstitial Scleroderma Rheumatoid Arthritis Dermatopolymyositis Sjogren’s Syndrome Mixed Connective Tissue Disease Scleroderma ILD may occur in either limited or diffuse cutaneous . 70–80% of patients exhibit pathological abnormalities of pulmonary fibrosis at autopsy. The incidence of radiographically detectable ILD varies from 25–65%. Pathologically similar to UIP. Rheumatoid Arthritis Initial radiographical studies found a low incidence of 1.6 –5% of ILD in RA. Decreased Dlco found in 41% of patients 50% exhibited features of fibrosis associated with lymphoid infiltrates in lung biopsy. Lung biopsy performed in a group of unselected patients demonstrated interstitial lesions in 80% of cases Nearly half were asymptomatic . Arthritis precedes lung disease in 80%. Risk Factors: Rheumatoid nodules High RF titres ANA titres Non M1M1 alpha 1 antitrypsin phenotypes Radiological Pattern Early acinar pattern. Nodular-reticular infiltrates. Lower lobe predominance. End-stage fibrosis results in the classical honeycombing pattern. Pathological pattern in RA-ILD UIP – predominant Peribronchovascular and interlobular lymphoid hyperplasia Cellular NSIP DIP Ig and RF deposit on immuno-staining Rheumatoid-pneumoconiosis Circulating rheumatoid factors are found in: 25% of patients with pneumoconiosis. 70% of those with Caplan's syndrome. Progressive massive fibrosis develops in 50% of miners with RA. Dermatopolymyositis ILD seen in 5-9% of cases. Lung involvement may precede muscle involvement in 30%. 3 distinct patterns seen: Rapidly progressive with acute fever, dyspnea and lung infiltrates similar to a Hamman- Rich-syndrome. Slowly progressive dyspnea upon exertion with chest radiographical abnormalities. Some patients may have no pulmonary symptoms, but abnormal radiographs and/or PFTs. Evaluation Anti-Jo-1 antibody – although maybe absent in some. Anti PL-7 or PL-12 antibody. Cardiopulmonary exercise testing to differentiate cause of dyspnea: Muscular weakness. ILD. Pulmonary HTN. Pathological Patterns Cryptogenic Organizing Pneumonia (COP) – Consolidation. UIP – Parenchymal bands, sub-pleural bands, peri-bronchovascular and inter-septal thickening. DAD – Ground glass. Treatment Concepts Steroids – for all presentations except UIP. UIP - DPM 5 yr survival – 33%. Cyclophosphamide. Sjögren's syndrome Lymphocytic Interstitial Pneumonitis – LIP. Psuedolymphoma Lymphoma UIP Management concepts BAL CD4/CD8 ratio is reduced – more frequent dyspnea, cough, PFTs abnormalities and radiological ILD. Steroids for extraglandular involvement. Chlorambucil. LIP or Psuedolymphomas may evolve into lymphomas. Mixed Connective Tissue Disease Pulmonary involvement has been described in 20–85% of patients. Spectrum of ILD predominantly similar to that of scleroderma i.e. UIP. DLCo decreased in 67%. Restrictive TLC in 50%. Management concepts Steroids for acute excerbation Chlorambucil or cyclophosphamide in combination with steroids effective in 2/3 of patients in a series of 34. Sullivan WD, Hurst DM, Harmon CE. A prospective evaluation emphasizing pulmonary involvement in patients with mixed connective tissue disease. Medicine 1984;63:92–107 3. Pleural Pleural effusions/pleuritis Fibrothorax Pleural effusion Typically exudative. Seen with: SLE Sjögren's syndrome Rheumatoid arthritis Type of Effusion Incidence Congestive heart failure 500,000 Pneumonia (bacterial) 300,000 Malignant disease 200,000 Lung 60,000 Breast 50,000 Lymphoma 40,000 Other 50,000 Pulmonary embolization 150,000 Viral disease 100,000 Post-coronary artery bypass surgery 60,000 Cirrhosis with ascites 50,000 Gastrointestinal disease 25,000 Collagen vascular disease 6,000 Tuberculosis 2,500 Asbestos exposure 2,000 Mesothelioma 1,500 Disease Diagnostic pleural fluid tests Empyema Observation (pus, putrid odor); culture Malignancy Positive cytology Lupus pleuritis LE cells present; pleural fluid serum ANA >1.0 Tuberculous pleurisy Positive AFB stain, culture Esophageal rupture High salivary amylase, pleural fluid acidosis (often as low as 6.00) Fungal pleurisy Positive KOH stain, culture Chylothorax Triglycerides (>110 mg/dL); lipoprotein electrophoresis (chylomicrons) Hemothorax Hematocrit (pleural fluid/blood >0.5) Urinothorax Creatinine (pleural fluid/serum >1.0) Peritoneal dialysis Protein (<1 g/dL); glucose (300 to 400 mg/dL) Extravascular migration of central venous catheter Observation (milky if lipids are infused); pleural fluid/serum glucose >1.0 Rheumatoid pleurisy Characteristic cytology Management concepts Diagnostic thoracentesis. Therapeutic thoracentesis – symptomatic relief. Rarely pleurodesis required for large recurrent effusions. Treat the underlying cause. Fibrothorax Usually follows intense inflammation of the pleura Empyema or a hemothorax Tuberculosis Collagen vascular disease Uremia Paragonimiasis Drug reactions Ergot alkaloids (e.g., bromocriptine, pergolide, and methysergide). Asbestos exposure 4. Airway Bronchiolitis OP Bronchiolitis Generic term is Bronchiolitis. Classification Scheme* Primary bronchiolar disorders Interstitial lung disease with a prominent bronchiolar component Large airways disease with a bronchiolar component * Proposed by Ryu et al. Am J Respir Crit Care Med. 2003 Clinical picture Variable symptoms of dyspnea and cough. Obstruction on PFT’s. Normal chest radiograph. High resolution CT scan Direct signs: Bronchiolar wall thickening (2-4 mm nodular and linear branching centrilobular opacities) Bronchiolectasis Luminal impaction (tree-in-bud opacities) Indirect signs Subsegmental atelectasis Mosaic attenuation (expiratory films helpful) Air trapping Perfusion changes Constrictive Bronchiolitis Also termed bronchiolitis obliterans, obliterative bronchiolitis. Pathologically characterized by a pattern of peribronchiolar fibrosis with complete cicatrization of the bronchiolar lumen. Typically seen in RA. OP 6/40 lung biopsies in RA Predominantly reticonodular pattern Prognosis better if RA-OP compared to RA-ILD Management concepts Consider addition of azithromycin in constrictive bronchiolitis when immunosuppression alone fails. OP – highly responsive to steroids.