Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Speech perception wikipedia , lookup
Hearing loss wikipedia , lookup
Telecommunications relay service wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
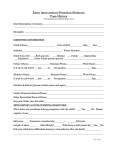
Office Use Only: MR identification label The Charity League Hearing and Speech Center Referral for Hearing and/or Speech Evaluation Appointments: Call (205) 638-7527 Physician Office Instructions: This form must be faxed to Julie Beals at (205)638-6740 prior to the patient’s appointment. Patient Name: _________________________________________________________ Birthdate: _______________________________ Parent(s) : ____________________________________________________________ Phone: _________________________________ Patient Appointment Date: ______________________________________________ Appointment Time: _______________________ Appointment Location: (please check one) Children’s Hospital (Clinic 2) 1600 7th Avenue South Birmingham, AL 35233 Phone (205) 638-9149 Children’s South 1940 Elmer J. Bissell Road Birmingham, AL 35243 Phone (205) 638-9149 Children’s on 3rd Outpatient Center 1208 3rd Avenue South Birmingham, AL 35233 Phone (205) 638-7500 Referring Physician: (please print) __________________________________________________________________________________ Referring Physician Address: _______________________________________________ Office Phone:___________________________ ________________________________________________FAX:__________________________________ Please note: Reason for referral, diagnosis and physician’s signature are required from the physician’s office prior to the patient being seen in the Hearing and Speech Center. Patient referred for: hearing test speech evaluation (only performed at Children’s on 3rd) Reason(s) for referral: failed hearing test in office/at school delayed speech/language milestones (check any and all that apply) failed newborn hearing screen speech difficult to understand parental concern of hearing loss swallowing/feeding difficulty teacher/school concern of hearing loss abnormal resonance or voice recurrent and/or chronic ear infections modified barium swallow developmental delay Passy-Muir speaking valve disease/syndrome (list)___________________________________________________________ other (list)______________________________________________________________________ Diagnosis (please list ICD-9 code): _______________________________________________________ Current Medications (list): ______________________________________________________________ MRSA Positive? yes no Type of Insurance:________________________________________________ Insurance authorization number:____________________________________ Physician signature:_________________________________________________________ Date:_______________________________ Rev 08/12