Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
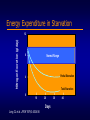
Metabolic Response to Starvation and Trauma: Nutritional Requirements Objectives • • • Explain the differences between metabolic responses to starvation and trauma Explain the effect of trauma on metabolic rate and substrate utilization Determine calorie and protein requirements during metabolic stress Metabolic Response to Fasting GLUCOSE UTILIZED (g/hora) I II III 40 IV V Exogenous Glycogen Gluconeogenesis 30 20 10 LEGEND I II III FUEL FOR BRAIN GLUCOSE GLUCOSE GLUCOSE IV GLUCOSE, KETONES V GLUCOSE, KETONES Ruderman NB. Annu Rev Med 1975;26:248 Fasting – Early Stage Muscle Alanine / Pyruvate Brain Glucose Glutamine Glycerol Gluconeogenesis Ketogenesis Fat AGL Ketones Liver Ureagenesis Ketones Urea NH3 Intestine Kidney Fasting – Late Stage Muscle Alanine / Pyruvate Brain Glucose Glutamine Glycerol Gluconeogenesis Ketogenesis Fat AGL Ketones Liver Ureagenesis Ketones Urea NH3 Intestine Kidney Metabolic Reaction to Starvation Hormone Source Norepinephrine Norepinephrine Epinephrine Thyroid Hormone T4 Sympathetic Nervous System Adrenal Gland Adrenal Gland Thyroid Gland (changes to T3 peripherally) Landberg L, et al. N Engl J Med 1978;298:1295. Change in Secretion Energy Expenditure in Starvation Nitrogen Excretion (g/day) 12 Normal Range 8 Partial Starvation 4 Total Starvation 0 10 20 Days Long CL et al. JPEN 1979;3:452-456 30 40 Metabolic Response to Trauma Flow Phase Energy Expenditure Ebb Phase Time Cutherbertson DP, et al. Adv Clin Chem 1969;12:1-55 Metabolic Response to Trauma: Ebb Phase • Characterized by hypovolemic shock • Priority is to maintain life/homeostasis Cardiac output Oxygen consumption Blood pressure Tissue perfusion Body temperature Metabolic rate Cuthbertson DP, et al. Adv Clin Chem 1969;12:1-55 Welborn MB. In: Rombeau JL, Rolandelli RH, eds. Enteral and Tube Feeding. 3rd ed. 1997 Metabolic Response to Trauma: Flow Phase • • • • • Catecholamines Glucocorticoids Glucagon Release of cytokines, lipid mediators Acute phase protein production Cuthbertson DP, et al. Adv Clin Chem 1969;12:1-55 Welborn MB. In: Rombeau JL, Rolandelli RH, eds. Enteral and Tube Feeding. 3rd ed. 1997 Metabolic Response to Trauma Endocrine Response Fatty Deposits Fatty Acids Liver & Muscle (glycogen) Glucose Muscle (amino acids) Amino Acids Metabolic Response to Trauma Nitrogen Excretion (g/day) 28 24 20 16 12 8 4 0 10 Long CL, et al. JPEN 1979;3:452-456 20 Days 30 40 Severity of Trauma: Effects on Nitrogen Losses and Metabolic Rate Nitrogen Loss in Urine Major Cirugía mayor Surgery Quemadura Moderate to Severe moderadaBurn a grave Infección Infection Sepsis Severe grave Sepsis Cirugía Elective electiva Surgery Basal Metabolic Rate Adapted from Long CL, et al. JPEN 1979;3:452-456 Metabolic Response to Starvation and Trauma Metabolic rate Body fuels Body protein Urinary nitrogen Weight loss Starvation Trauma or Disease conserved conserved wasted wasted slow rapid The body adapts to starvation, but not in the presence of critical injury or disease. Popp MB, et al. In: Fischer JF, ed. Surgical Nutrition. 1983. Metabolic Response to Surgical Trauma Metabolic Changes after Trauma Muscle Alanine / Pyruvate Brain Glucose Glutamine Glycerol Gluconeogenesis Ketogenesis Fat AGL Ketones Liver Ureagenesis Ketones Urea NH3 Intestine Kidney Determining Calorie Requirements • • • Indirect calorimetry Harris-Benedict x stress factor x activity factor 25-30 kcal/kg body weight/day Metabolic Response to Starvation and Trauma: Nutritional Requirements Injury Minor surgery Long bone fracture Cancer Peritonitis/sepsis Severe infection/multiple trauma Multi-organ failure syndrome Burns Activity Confined to bed Out of bed Stress Factor 1.00 – 1.10 1.15 – 1.30 1.10 – 1.30 1.10 – 1.30 1.20 – 1.40 1.20 – 1.40 1.20 – 2.00 Example: Energy requirements for patient with cancer in bed = BEE x 1.10 x 1.2 Activity Factor 1.2 1.3 ADA: Manual Of Clinical Dietetics. 5th ed. Chicago: American Dietetic Association; 1996 Long CL, et al. JPEN 1979;3:452-456 Metabolic Response to Overfeeding • • • • • Hyperglycemia Hypertriglyceridemia Hypercapnia Fatty liver Hypophosphatemia, hypomagnesemia, hypokalemia Barton RG. Nutr Clin Pract 1994;9:127-139 Macronutrients during Stress Carbohydrate • • • At least 100 g/day needed to prevent ketosis Carbohydrate intake during stress should be between 30%-40% of total calories Glucose intake should not exceed 5 mg/kg/min Barton RG. Nutr Clin Pract 1994;9:127-139 ASPEN Board of Directors. JPEN 2002; 26 Suppl 1:22SA Macronutrientes during Stress Fat • • • Provide 20%-35% of total calories Maximum recommendation for intravenous lipid infusion: 1.0 -1.5 g/kg/day Monitor triglyceride level to ensure adequate lipid clearance Barton RG. Nutr Clin Pract 1994;9:127-139 ASPEN Board of Directors. JPEN 2002;26 Suppl 1:22SA Macronutrients during Stress Protein • • Requirements range from 1.2-2.0 g/kg/day during stress Comprise 20%-30% of total calories during stress Barton RG. Nutr Clin Pract 1994;9:127-139 ASPEN Board of Directors. JPEN 2002;26 Suppl 1:22SA Determining Protein Requirements for Hospitalized Patients No Stress Moderate Stress Severe Stress Calorie:Nitrogen Ratio > 150:1 150-100:1 < 100:1 Percent Potein / Total Calories < 15% protein 15-20% protein Protein / kg Body Weight 0.8 g/kg/day 1.0-1.2 g/kg/day Stress Level > 20% protein 1.5-2.0 g/kg/day Role of Glutamine in Metabolic Stress • • • • Considered “conditionally essential” for critical patients Depleted after trauma Provides fuel for the cells of the immune system and GI tract Helps maintain or restore intestinal mucosal integrity Smith RJ, et al. JPEN 1990;14(4 Suppl):94S-99S; Pastores SM, et al. Nutrition 1994;10:385-391 Calder PC. Clin Nutr 1994;13:2-8; Furst P. Eur J Clin Nutr 1994;48:607-616 Standen J, Bihari D. Curr Opin Clin Nutr Metab Care 2000;3:149-157 Role of Arginine in Metabolic Stress • • • • • Provides substrates to immune system Increases nitrogen retention after metabolic stress Improves wound healing in animal models Stimulates secretion of growth hormone and is a precursor for polyamines and nitric oxide Not appropriate for septic or inflammatory patients. “Giving arginine to a septic patient is like putting gasoline on an already burning fire. ” - B. Mizock, Medical Intensive Care Unit, Cook County Hospital, Chicago, IL Barbul A. JPEN 1986;10:227-238; Barbul A, et al. J Surg Res 1980;29:228-235 Key Vitamins and Minerals Vitamin A Vitamin C B Vitamins Pyridoxine Zinc Vitamin E Folic Acid, Iron, B12 Wound healing and tissue repair Collagen synthesis, wound healing Metabolism, carbohydrate utilization Essential for protein synthesis Wound healing, immune function, protein synthesis Antioxidant Required for synthesis and replacement of red blood cells Summary • • Metabolic response to starvation is an adaptive mechanism Nutritional requirements increase during trauma