Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
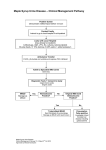
MAPLE SYRUP URINE DISEASE Brittany Taylor Rebecca Linstead Overview of Disorder The body is unable to process leucine, isoleucine and valine because at least one of the four genes that code for the enzyme responsible for breaking down these amino acids has a mutation. Four Forms of MSUD Enzyme activity = <2% Classic neonatal form: Most common; most severe Absence or significant decrease in function of the enzyme branched-chain ketoacid dehydrogenase, which is needed to break down the branched-chain amino acids Infants don’t show symptoms until days four to seven of life Intermediate Form Enzyme activity = 3-30% A higher level of enzyme is present than in the classical form, therefore allowing a higher tolerance of leucine Management is the same in both intermediate and classical forms of MSUD Intermittent Form Enzyme activity = 5-20% Mild form of MSUD Greater amount of enzyme activity is present An affected child will not show symptoms until around 12-24 months of age Symptoms are usually brought on by a surge in protein intake or illness Thiamine-Responsive Form Enzyme activity = 2-40% Most rare form A child with this form may take large doses of thiamine to increase their enzyme activity Diagnosis Suspect of MSUD results from the characteristic odor of maple syrup in the urine Confirmed diagnosis with abnormal amounts of keto acids and amino acids in blood and urine Serum alanine levels may also be depressed Genetic Inheritance Autosomal recessive Each parent carries one normal copy and one mutated copy of the gene but does not show symptoms themselves Signs and Symptoms Poor appetite Irritability Maple smelling urine Mental retardation Seizures Coma and death if left untreated Infants will… Lose their sucking reflex Become limp with episodes of rigidity Incidence In the US = 1 in 185,000 births The Mennonite population in Lebanon and Lancaster counties of Pennsylvania have an incidence of 1 in 176 newborns Founder’s effect? Prognosis Overall very poor if left undetected/untreated With treatment and proper dietary management, the prognosis is good However, severe stress and illness can cause a surge of certain amino acids Medical Management of MSUD Long-term management via diet Restriction of leucine, isoleucine and valine Treatment of acute metabolic decompensation Liver transplant may be an option but is associated with other consequences (transplant mediations for life) Goal of Nutritional Management Ultimate goal is to restrict branched-chain amino acids while avoiding impairment of growth and intellectual development Maintain normal levels of branched-chain amino acids, particularly leucine General Nutritional Management Lifelong nutrition support via formulas and foods with minimal (if any) branched-chain amino acids Leucine intake is carefully monitored and calculated following the measurement of plasma branchedchain amino acids Nutritional Management during Acute Illness Situational stress and illness may result in metabolic decompensation Initiate IV glucose to promote anabolism Stop intake of branched-chain amino acids; resume when levels normalize If possible, continue additional dietary support including lipids and formulas free of branched-chain amino acids Hemodialysis may be necessary to remove toxic metabolites Supplements, Formulas and Medications Powdered protein supplements that are similar to whey protein Leucine, isoleucine and valine removed Major source of protein for patient Ketonex makes an infant formula in powdered and liquid forms that are suitable for infants with MSUD No medications available for specific treatment of MSUD Isoleucine diet and valine may be supplemented back into Case Study Anthropometrics: Born full term Born 7 lb 3 oz, 19 inches Age: 3 years, 1 month Height: 94 cm (37 in) 50th percentile Weight: 14.3 kg (31.5 lb) 50th percentile Length for weight: 75-90th percentile Growth patterns have been consistently normal Family and Social History Patient lives with mother, step father, two older sisters (13 and 14 years of age) and three stepsiblings (14 y/o male, two 12 y/o females) Family receives WIC services and had an appointment scheduled with Early Intervention as of last visit Insurance coverage through Medicaid; Children’s Special Services provides low protein foods and helps cover medical expenses if not covered by Medicaid Family and Social History Family seems to care for patient very well Dad is literate and understands ROSS Family Guide booklet as well as need for diet changes Feeds patient through G-tube Mother attends G-tube clinic and changes is G-tube Grandparents assist in care Patient is enrolled in HeadStart Receptive language increasing; says approximately six words Prenatal History Normal Pregnancy! Prenatal vitamin and iron supplement Visited doctor regularly Gained 30 lbs No family hx of DM, heart disease or food allergies Health History Had problems with poor suckling and electrolyte imbalances Received breast milk and Ketonex via NG tube due to his poor suck Initiated thickened liquids and some solid foods but was not obtaining enough nutrients PEG tube was placed to provide patient with nutrients due to dysphagia As of most recent visit, mother reports dysphagia has resolved but no notation of latest swallow test; patient now with some PO intake but still with EN via PEG Health History (cont) No food allergies 8 teeth on both top and bottom row Current medications: isoleucine and valine No mention of smoking or alcohol abuse in home Activity level: cannot ride a tricycle; is able to partially dress himself; goes up and down the stairs; No lifestyle modifications needed at this time as patient is at appropriate height and weight Feeding Skills and Behavior Will feed himself with his fingers but will not use a fork or spoon – there may be some fine-motor delay; may also have a language delay Has full range of motion Parenting skills are good Advanced formula preparation Eating Habits Good appetite Eating more solid foods but is still dependent on PEG tube Enjoys cereal, oatmeal and pizza Present Intake Last food record: Captain Crunch, Kool-aide, chicken nuggets, fruit rollup, apple juice, grape soda, cheese pizza, oatmeal Evaluation of intake: 100% of kcal, 402% of protein, 148% of CHO Isoleucine: 326 mg (165-325 mg/day)100% Leucine: 593 mg (275-535 mg/day)111% Valine: 396 (190-400 mg/day) 100% Biochemical Information Most recent data: Prealbumin: 18 mg/dl Glucose: 68 mg/dl Bicarb: 28 mEq/L All normal! Findings ICD-9 Codes 270.3= MSUD V44.1= G-Tube Inadequate oral intake related to dysphagia and feeding difficulties as evidenced by majority of nutritional needs met through enteral feedings Altered nutrient utilization related to inborn error of metabolism-MSUD as evidenced by hx of elevated leucine with restrictions needed to keep within range Recommendations Continue with current regimen of 125 g of Ketonex1, 55 g of Ketonex-2 and 32 g of Good Start, 3 ml of isoleucine and 6 ml of valine with water to total 40 ounces Administer 5-8oz feedings throughout the day into PEG tube Encourage low protein PO intake Presenting Information to Family No barriers noted in chart regarding literacy or ability to care for patient All their ducks are in a row Role of MNT Rationale for recommendations: Dietary restrictions will limit branched-chain amino acids, specifically leucine Prevention of toxic build-up of these amino acids and their metabolites Enteral nutrition continued as we are unsure of dysphagia status and patient still has difficulty feeding himself Maintain adequate calorie and protein intake to promote growth Role of RD To provide family and patient with support and recommendations regarding MNT To modify the diet as needed to keep amino acids within target ranges To act as a resource References http://ghr.nlm.nih.gov/condition/maple-syrup-urine-disease http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2044.1996.tb12568.x/pdf http://emedicine.medscape.com/article/946234-medication#2 http://newenglandconsortium.org/for-professionals/acute-illness-protocols/organic-aciddisorders/maple-syrup-urine-disease-msud http://www.wvdhhr.org/nbms/diseases/Maple_Syrup_Urine_Disease.asp http://www.uic.edu/classes/phar/phar332/Clinical_Cases/aa%20metab%20cases/MSUD/ Diagnostics_of_MSUD.html http://www.newbornscreening.info/Parents/aminoaciddisorders/MSUD.html