Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
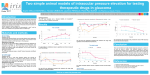
Diagnosis of Essential Iris Atrophy in a patient with uncontrolled unilateral intraocular pressure Shikha Yadav, O.D. Ocular Disease Resident Baltimore Veterans Affairs, MD This case report describes the diagnosis of essential iris atrophy (ICE syndrome) in a young patient with corneal edema, progressive corectopia and uncontrolled unilateral intraocular pressure despite multiple topical medical therapy. I. Case History A 41-year-old white female presents for a glaucoma evaluation with the chief complaint of blurred vision in her left eye. The patient was previously managed by her optometrist for increased intraocular pressure of her left eye, and was given Lumigan and Brimonidine ophthalmic solutions. Ocular History: sudden onset of corectopia after child birth, 11 years ago. Medical History: seasonal allergies Medications: birth control pill, Lumigan and Brimonidine. II. Pertinent findings Clinical findings o VA: OD CC 20/15-, OS CC 20/20o EOM: normal o CVF: normal o Pupils: normal OD, corectopia OS, (-) RAPD OU o SLE: Normal OU, unless noted otherwise below. o Cornea: fine, beaten metal appearance of corneal endothelium and mild corneal edema o Iris: subtle iris transillumination defects with localized iris-corneal adhesion OS o IOP: 13 OD, 40 OS o DFE: Normal OU o Optic Nerve: 0.3 C/D OD; 0.6 C/D OS o NFL grossly intact OU External photos Gonioscopy Specular Microscopy o OD: Normal, hexagonal shaped cells. Normal cell count (2684) o OS: Abormal endothelium with large spaces between cells and low cell count (1899). The color of the cells are reversed with black surrounded by a white border. Fundus photos III. Differential diagnosis Essential Iris Atrophy Chandler’s syndrome Cogan-Reese syndrome Axenfeld-Reiger Syndrome Posterior polymorphous corneal dystrophy (PPMD) Fuchs endothelial dystrophy IV. Diagnosis and discussion Essential iris atrophy o Anterior segment presentation o Ruling out differentials with specular microscopy and gonioscopy o Medical and surgical techniques to control intraocular pressure. Proposed viral etiology for ICE syndromes Endothelial keratoplasty for corneal edema Prognosis of long term corneal and IOP management V. Treatment Initial management o Continue Lumigan qhs OS and Brimonidine BID OS. Add Combigan BID OS. Target pressure set to <21. o RTC 1 month for IOP check Follow-up examinations: o IOP reduced to 22 in OS but diurnal fluctuation considered. o Patient was followed every 6 weeks for IOP checks. o 3 months after initial presentation, IOP spiked to 40mmHg with good medication compliance. Pilocarpine 1% TID was added to current topical therapy. o IOP remained below target pressure for another 4 months. o 7 months after initial presentation, patient’s IOP spiked to 37 mmHg and major change in optic nerve appearance was noted. o Trabeculotomy was performed in OS. Final post-op: 5 months post Trabeculotomy o Vision: 20/20 OS o IOP: 12mmHg on Lumigan qpm OS VI. Conclusion Clinical pearls of essential iris atrophy o Always consider ICE syndrome on your list of differentials for unilateral glaucoma o Know when to consider surgical management for uncontrolled IOP Bibliography