Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
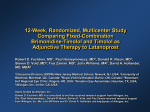
A 12-Week, Randomized, Double-Masked, Multicenter Study of the Fixed Combination of Latanoprost and Timolol in the Evening versus the Individual Components Michael Diestelhorst, MD,1 Lill-Inger Larsson, MD, PhD,2 for the European–Canadian Latanoprost Fixed Combination Study Group* Purpose: To compare the efficacy and tolerability of fixed-combination latanoprost and timolol applied in the evening with the concomitant use of the individual components. Design: Twelve-week, randomized, double-masked, multicenter study. Participants: Five hundred seventeen randomized patients with ocular hypertension; open-angle, pigmentary, or exfoliation glaucoma; and baseline (after washout) intraocular pressure (IOP) levels between 23 and 33 mmHg. Methods: Patients received either the fixed combination of latanoprost and timolol once daily in the evening and a placebo in the morning and evening or the unfixed combination of latanoprost once daily in the evening and timolol in the morning and evening. Study visits were at weeks 2, 6, and 12. Main Outcome Measures: The primary efficacy end point was mean change from baseline to week 12 in diurnal IOP (mean IOPs of 8 AM, 12 PM, and 4 PM). The fixed combination was considered noninferior to the unfixed combination if the upper limit of the 95% confidence interval (CI) of the difference was ⬍1.5 mmHg (analysis of covariance). Adverse events were recorded at each visit. Results: In all, 502 patients were included in intent-to-treat analyses (fixed combination, n ⫽ 255; unfixed combination, n ⫽ 247). For the fixed- and unfixed-combination groups, mean baseline diurnal IOP levels were 25.4 mmHg and 25.2 mmHg, respectively, and mean diurnal IOP reductions were 8.7 mmHg and 9.0 mmHg (between-treatment difference, 0.3 mmHg; 95% CI, ⫺0.1 to 0.7 mmHg; P ⫽ 0.15). Both treatments were well tolerated. Conclusions: The fixed combination of latanoprost and timolol administered once daily in the evening is not inferior to the unfixed combination of latanoprost once daily in the evening and timolol twice daily. The fixed combination provides an effective and well-tolerated alternative to multiple instillations. Ophthalmology 2006; 113:70 –76 © 2006 by the American Academy of Ophthalmology. Application of a single topical ocular hypotensive agent is the preferred initial treatment for patients with glaucoma or ocular hypertension.1 However, targeted intraocular pressure (IOP) reduction often is not obtained with monotherapy. A study of initial treatment with a -blocking agent, for example, found that one third of patients required a change in or an addition to therapy after 1 year, a proportion that increased to half after 2 years.2 When changing the Originally received: April 29, 2005. Accepted: June 25, 2005. Manuscript no. 2005-372. 1 University of Cologne, Cologne, Germany. 2 Pfizer Inc., New York, New York. The research was supported by Pfizer Inc. Correspondence to Michael Diestelhorst, MD, Department of Ophthalmology, Univerisitäts-Augenklinik, University of Cologne, Joseph-StelzmannStrasse 9, Cologne 50931, Germany. E-mail: michael.diestelhorst@ medizin.uni-koeln.de. *See “Appendix” for Study Group membership. 70 © 2006 by the American Academy of Ophthalmology Published by Elsevier Inc. therapeutic regimens of insufficiently responsive patients, it has been suggested that an agent with a complementary mode of action be added if the first-choice monotherapy is well tolerated.3 In this setting, a combined-drug preparation is preferable to maximize adherence to therapy and quality of life.3 The -adrenergic receptor antagonist timolol, which lowers IOP by reducing the production of aqueous humor,4 – 6 exhibits additive effects when combined with other ocular hypotensive agents.7–10 The complementary mechanism of action of the prostaglandin F2␣ analog latanoprost, which acts primarily by increasing outflow,11 makes it a logical choice for combination with timolol. In fact, the fixed combination of latanoprost and timolol has been shown to reduce IOP more effectively than either agent used alone and has been found to have good tolerability.12–14 We recently published the results of a double-masked, randomized, crossover study comparing fixed-combination latanoprost and timolol administered once daily in the ISSN 0161-6420/06/$–see front matter doi:10.1016/j.ophtha.2005.06.027 Diestelhorst and Larsson 䡠 Fixed Combination of Latanoprost and Timolol in the Evening morning versus once-daily evening latanoprost and twicedaily timolol in patients with open-angle glaucoma and ocular hypertension.15 Both regimens were found to be well tolerated and effective. The 1.1-mmHg difference in mean within-patient diurnal IOP levels favoring the unfixed combination may have reflected the fact that latanoprost was administered in the evening, whereas the fixed combination was instilled in the morning. Previous studies have shown better diurnal IOP control with evening dosing of both latanoprost16,17 and latanoprost and timolol,18 probably reflecting the fact that latanoprost’s maximum effect occurs 8 to 12 hours after dosing. The purpose of the present study was to assess the efficacy and tolerability of the fixed combination of latanoprost and timolol administered in the evening versus those of an evening dose of latanoprost and twice-daily doses (morning and evening) of timolol. Materials and Methods Study Design This 12-week, randomized, double-masked study was conducted at 53 centers throughout Europe and Canada. The protocol was reviewed by an institutional review board/independent ethics committee before the study, and the research was conducted in accordance with the ethical standards maintained in the Declaration of Helsinki. All patients were fully informed and provided written consent for participation before enrollment. Patients See Table 1 for study inclusion and exclusion criteria. Treatments and Assessments Potentially eligible patients were assessed at a screening visit 4 weeks to 5 days before study entry. Medical and ocular histories were recorded; visual acuity (VA) was measured; and visual field (if not performed within the previous year), lid and slit-lamp examination, and ophthalmoscopy were performed. Intraocular pressure was measured using a calibrated Goldmann applanation tonometer. All ocular measurements were performed in both eyes. Required washout periods before the baseline visit were 5 days for cholinergic agonists and carbonic anhydrase inhibitors, 2 weeks for adrenergic agonists, and 4 weeks for -adrenergic antagonists and prostaglandin analogs. Patients requiring a 4-week washout returned after 2 weeks for an IOP safety check. If the IOP was ⬎33 mmHg at the safety visit, the patient was either excluded from the study or treated with an IOP-lowering medication with a shorter washout period. If an alternative ocular hypotensive medication was used, a washout period was required before the baseline visit. Patients with IOP levels of ⬍33 mmHg at the safety visit could continue in the study. Study visits occurred at baseline and weeks 2, 6, and 12. At the baseline visit, VA measurement and lid and slit-lamp examinations were repeated, and masked evaluators performed 3 IOP measurements in each eye starting with the right at 8 AM, 12 PM, and 4 PM. The masked evaluator recorded IOP readings. Statistical analyses included the mean of these IOP measurements at each time point. To be eligible for randomization, an 8 AM IOP level between 23 mmHg and 33 mmHg was required. After the 4 PM IOP level was obtained, eligible patients were assigned consecutively to 1 of the 2 treatment groups 1:1 using randomization codes generated by Pharmacia Global Pharmaceutical Sciences. Patients assigned to receive the fixed combination instilled 1 drop (active ingredients: latanoprost 0.005% and timolol maleate 0.5%) once daily in the evening and 1 drop of a placebo (vehicle of the fixed combination) in the morning and evening. Patients in the unfixed-combination group administered 1 drop of latanoprost 0.005% once daily in the evening and 1 drop of timolol maleate 0.5% in the morning and evening. At baseline and week 6, each patient received a kit containing study drugs packaged in 2.5-ml bottles. Each kit held 3 cartons: 1 contained the morning medication bottle (labeled 8 AM), and 2 contained the evening medication bottles (labeled 8 PM bottle A and 8 PM bottle B). Patients were instructed to administer 1 drop of study drug to the affected eye(s) every morning from the bottle labeled 8 AM and 1 drop every evening from each of the 2 bottles Table 1. Study Criteria Inclusion Criteria Exclusion Criteria ● Age ⱖ 18 yrs ● Unilateral or bilateral ocular hypertension or primary open-angle, pigmentary, or exfoliative glaucoma ● Naive to IOP-lowering medication ● Closed or barely open anterior chamber angle, history of acute angle-closure glaucoma, ocular surgery on the globe of the eye, or history of any ocular filtering surgical intervention (unfiltered eye could be enrolled) ● Argon laser trabeculoplasty, selective laser trabeculoplasty in the study eye(s), or ocular inflammation in either eye during the 3 mos before screening ● Insufficient response to current IOP-lowering monotherapy or dual therapy at screening (opinion of investigator) ● Baseline mean 8 AM IOP in study eye(s) between 23 mmHg and 33 mmHg after washout of previous therapy ● Best-corrected visual acuity ⱖ 20/200 ● Able to adhere to the treatment/visit plan ● Known hypersensitivity to benzalkonium chloride or any other component in either study drug solution ● Any abnormal ocular conditions or symptoms that would prevent study eligibility (opinion of investigator), conditions in which treatment with -blocking therapies was contraindicated, an ocular infection in either eye within 3 weeks before screening, or use of an investigational medication within the month preceding screening ● Use of a systemic medication known to affect IOP levels unless patient and medication dosage had been stable for 3 mos before screening and unless the dosage was not expected to change during the study period ● Woman of childbearing potential who was not using adequate contraceptive methods or was pregnant or nursing IOP ⫽ intraocular pressure. 71 Ophthalmology Volume 113, Number 1, January 2006 labeled 8 PM. The evening regimen was to be administered with a 5-minute interval between drops from bottle A and bottle B. The first dose of study medication was instilled the evening of the baseline visit, and patients were instructed not to instill study medication on the morning of their next study visit. Each patient’s IOP level was measured by a masked observer at any time during the week 2 visit and at 8 AM, 12 PM, and 4 PM during the week 6 and week 12 visits. As at baseline, masked evaluators performed 3 IOP measurements in each eye starting with the right at each measurement time. It was requested that the same examiner measure IOP using the same calibrated tonometer at each time point and at each visit for a given patient. At weeks 6 and 12, patients instilled the 8 AM dose of study medication after IOP measurement. Visual acuity measurement and lid and slit-lamp examinations were repeated at weeks 6 and 12, and ophthalmoscopy was performed at week 12. Throughout the study, all adverse events were recorded and monitored by investigators. The intensity of each adverse event was graded using defined criteria, and events were classified as serious or nonserious. Patients with serious adverse events, adverse events related to study medication, or ocular adverse events at the week 12 visit had an additional follow-up visit 2 weeks later. Variables and Analyses Only data for study eyes, which met all inclusion and no exclusion criteria, were included in the efficacy analyses. If both eyes qualified as study eyes, the average IOP of the 2 eyes was used in the analyses. The primary efficacy variable was the mean change between baseline and week 12 in mean diurnal IOP. The mean diurnal IOP of a patient at any visit was calculated as the mean value of the IOPs recorded at 8 AM, 12 PM, and 4 PM. If data for any time point were missing, the mean diurnal IOP was calculated as the mean of the nonmissing IOP measurements. Between-group differences were analyzed using an analysis of covariance model with baseline IOP as a covariate and treatment and center as factors. The treatment difference (fixed combination ⫺ unfixed combination) and a 95% confidence interval (CI) for the difference were calculated, and the fixed combination was considered noninferior to the unfixed combination if the upper limit of the 95% CI of the difference was ⬍1.5 mmHg. This noninferiority design was chosen to determine whether the fixed combination was no less effective (either more or similarly effective) than the unfixed combination. Treatment differences for secondary efficacy variables, such as mean change in diurnal IOP at week 6 and percent change from baseline in diurnal IOP at weeks 6 and 12, were tested using an analysis of covariance model with baseline, treatment, and center in the model. Differences in proportions of patients with prespecified percentages of mean diurnal IOP reductions from baseline to week 12 and achieving prespecified diurnal IOP levels were tested using center-stratified Cochran–Mantel–Haenszel tests. Intentto-treat (ITT) efficacy analyses included all patients who received study medication, had a baseline IOP measurement, and had at least 1 valid week 6 or week 12 IOP measurement. The lastobservation-carried-forward method was used to impute missing data. The per protocol population included all patients in ITT analyses who completed the 12-week study with no major protocol deviations. Safety analyses included randomized patients receiving at least 1 dose of study medication (safety population). The Medical Dictionary for Regulatory Activities coding system was used to classify adverse events, and frequencies of ocular and systemic adverse events were tabulated. The sample size was calculated using a t test with a 1-sided significance level of 0.025 and 80% power. To test an equivalence limit of 1.5 mmHg, it was determined before the study that a 72 Table 2. Demographic Data (Intent-to-Treat Population) Treatment Group Demographic Characteristic Gender [n (%)]* Male Female Age (yrs) Mean SD Range Ethnic origin [n (%)] White Black Other Study eye(s) [n (%)] Right Left Both Treated eye(s) [n (%)] Right Left Both Diagnosis of study eye(s) [n (%)] Primary open-angle glaucoma Ocular hypertension Exfoliative glaucoma Pigmentary glaucoma Mixed† Visual field—any glaucomatous damage in study eye(s) [n (%)] Yes Color of treated eye [n (%)] Homogeneously brown Homogeneously blue, gray, or green Blue–brown or gray–brown Green–brown Yellow–brown Fixed Combination (n ⫽ 255) Unfixed Combination (n ⫽ 247) 129 (50.6) 126 (49.4) 99 (40.1) 148 (59.9) 65 10.9 33–94 65 11.2 22–89 251 (98.4) 3 (1.2) 1 (0.4) 242 (98.0) 3 (1.2) 2 (0.8) 27 (10.6) 26 (10.2) 202 (79.2) 33 (13.4) 24 (9.7) 190 (76.9) 8 (3.1) 4 (1.6) 243 (95.3) 7 (2.8) 3 (1.2) 237 (96.0) 163 (63.9) 70 (27.5) 12 (4.7) 5 (2.0) 5 (2.0) 163 (66.0) 60 (24.3) 10 (4.0) 4 (1.6) 10 (4.0) 122 (47.8) 121 (49.0) 107 (42.0) 87 (34.1) 32 (12.5) 22 (8.6) 7 (2.7) 100 (40.5) 99 (40.1) 21 (8.5) 18 (7.3) 9 (3.6) SD ⫽ standard deviation. *P ⫽ 0.018 for difference between groups. † Different diagnosis in right eye and left eye. sample of 194 evaluable patients per treatment group was required assuming a difference of 0.5 mmHg in mean IOP reduction and a common standard deviation (SD) of 3.5 mmHg. A minimum of 430 patients was planned to allow for patient withdrawals, and 588 were actually enrolled. Overenrollment reflected the fact that patients were entered into a 4-week washout period before randomization. Towards the end of recruitment, investigators started to increase the number of patients entered to fulfill enrollment goals. When sufficient patients were randomized, there were still many undergoing the 4-week washout. Although notices to stop enrollment were sent to investigators, it was felt appropriate that these patients should be allowed to continue into the study, having been taken off their standard medication for the purposes of the trial. Results Of the 588 patients enrolled between March 27 and December 5, 2003, 517 were randomized (fixed combination, n ⫽ 263; unfixed combination, n ⫽ 254). Eight patients randomized to receive the fixed combination and 7 to be treated with the unfixed combination Diestelhorst and Larsson 䡠 Fixed Combination of Latanoprost and Timolol in the Evening Table 3. Intraocular Pressure (IOP) and IOP Reduction from Baseline to Week 12 (Intent-to-Treat Population) Baseline IOP (mmHg) (Mean ⴞ SD) Diurnal 8 AM 12 PM 4 PM IOP Change from Baseline to Week 12 (mmHg) (Least Square Mean ⴞ SE) Fixed Combination (n ⫽ 255) Unfixed Combination (n ⫽ 247) Fixed Combination (n ⫽ 255) Unfixed Combination (n ⫽ 247) Difference (95% CI) P Value 25.4⫾2.3 26.0⫾2.3 25.4⫾2.7 24.7⫾2.9 25.2⫾2.4 26.0⫾2.3 25.3⫾2.9 24.5⫾2.9 ⫺8.7⫾0.2 ⫺9.1⫾0.2 ⫺8.7⫾0.2 ⫺8.2⫾0.2 ⫺9.0⫾0.2 ⫺9.5⫾0.2 ⫺9.1⫾0.2 ⫺8.3⫾0.2 0.3 (⫺0.1–0.7) 0.4 (⫺0.1–0.8) 0.4 (⫺0.0–0.9) 0.1 (⫺0.4–0.5) 0.15 0.12 0.06 0.78 CI ⫽ confidence interval; SD ⫽ standard deviation; SE ⫽ standard error. were excluded from ITT analyses because they either did not receive study medication or did not have required measurements; thus, the ITT population included 255 and 247 patients, respectively. An additional 28 patients in the fixed-combination group and 18 in the unfixed-combination group were excluded from the per protocol population primarily due to major protocol violations. One patient randomized to fixed combination did not receive study medication and was excluded from analyses of tolerability. Treatment groups were well matched with regard to age, ethnic origin, and baseline ocular characteristics (Table 2). The gender distributions differed significantly (P ⫽ 0.02), but when gender was added to the analysis of covariance model for the primary analysis, the conclusion regarding noninferiority was not affected. The most common IOP-reducing medications at screening were -blockers (fixed combination, n ⫽ 109; unfixed combination, n ⫽ 107) and prostaglandins (fixed combination, n ⫽ 114; unfixed combination, n ⫽ 102). Efficacy In the ITT population, mean baseline diurnal IOP levels were approximately 25 mmHg in both treatment groups (Table 3). The reduction in mean diurnal IOP from baseline to week 12 was 8.7 mmHg in the fixed-combination group and 9.0 mmHg in the unfixed-combination group. The between-group difference was 0.3 mmHg, and the upper bound of the 95% CI was ⬍1.5 mmHg, indicating noninferiority of the fixed combination (P ⫽ 0.15). At week 12, the fixed combination was noninferior at each measurement time (Table 3), and mean diurnal IOP levels were similar (fixed combination, 16.7 mmHg; unfixed combination, 16.4 mmHg; P ⫽ 0.15). At week 6, the mean diurnal IOP reduction from baseline was noninferior in the fixed-combination group (fixed combination [mean ⫾ SD], 8.7⫾0.1; unfixed combination, 8.9⫾0.1; difference [95% CI]: 0.2 [⫺0.2 to 0.6]; P ⫽ 0.36). Percent reductions in mean diurnal IOP levels were similar at week 12 (fixed combination, 34.0⫾0.6%; unfixed combination, 35.1⫾0.6%; P ⫽ 0.18) and week 6 (fixed combination, 34.3⫾0.6%; unfixed combination, 34.9⫾0.6%; P ⫽ 0.42). No statistically significant difference was observed with regard to numbers of patients reaching prespecified percentages of mean diurnal IOP reduction at the end of treatment (Fig 1). Numbers achieving specific mean diurnal IOP levels at week 12 also were similar (Fig 2), except for the percentage reaching ⱕ15 mmHg, where borderline statistical significance was noted (P ⫽ 0.05) in favor of the unfixed combination. The results of the per protocol analyses confirmed those in the ITT population, except that the difference in percentages of patients reaching ⱕ15 mmHg was not statistically significant (P ⫽ 0.19). Safety Both treatments were well tolerated, but the fixed combination demonstrated a better tolerability profile with regard to percentages of patients reporting at least 1 adverse event and reporting an ocular adverse event (Table 4). The majority of adverse events were mild Figure 1. Patients reaching prespecified percentages of mean diurnal intraocular pressure (IOP) reduction at week 12 (intent-to-treat population). 73 Ophthalmology Volume 113, Number 1, January 2006 Figure 2. Patients achieving prespecified mean diurnal intraocular pressure (IOP) levels at week 12 (intent-to-treat population). *P ⫽ 0.05. to moderate in intensity, and most patients recovered completely. Eye disorders were the most frequently reported adverse events and occurred more frequently in the unfixed-combination group (fixed combination, 27/262 [10.3%]; unfixed combination, 43/254 [16.9%]). With the exception of ocular hyperemia (fixed combination, 6/262 [2.3%]; unfixed combination, 18/254 [7.1%]) and eye irritation (fixed combination, 6/262 [2.3%]; unfixed combination, 11/254 [4.3%]), no other individual ocular adverse event was reported in ⱖ3% of patients in either treatment group. The majority of ocular adverse events were related to hyperemia (Medical Dictionary for Regulatory Activities preferred terms hyperemia, ocular hyperemia, and red eye), which was reported in 8 of 262 (3.1%) patients receiving the fixed combination and in 22 of 254 (8.7%) of those treated with the unfixed combination. Few discontinuations due to adverse events occurred in either treatment group (Table 4). Five serious adverse events occurred in the fixedcombination group, and 2 in the unfixed-combination group; 1 was considered possibly related to study medication (toxic keratoconjunctivitis in a patient receiving the fixed combination). One patient died of a myocardial infarction. No systemic adverse event was considered related to study medication. Discussion The results of this 12-week study provide evidence that the fixed combination applied in the evening is noninferior to the unfixed combination of latanoprost applied in the evening and timolol twice daily. The mean between-group difference in mean diurnal IOP reduction from baseline was 0.3 mmHg, demonstrating noninferiority of the fixed combination. Although the noninferiority criterion for the present study was 1.5 mmHg, the upper bound of the 95% CI was ⬍1.0 mmHg, allowing us to conclude noninferiority at that level of difference as well. These findings support the impression that the 1.1-mmHg difference favoring the unfixed combination found in our previous study15 (which had a noninferiority criterion of 1.0 mmHg) was related, at least in part, to the fact that the fixed combination was instilled in the morning, whereas latanoprost was instilled in the evening as part of the unfixed combination. Previous studies have documented the effectiveness of once-daily fixed-combination latanoprost and timolol in comparison with other 2-drug regimens. For example, fixed-combination latanoprost and timolol has been shown to be more effective than either the twice-daily administration of fixed-combination dorzolamide and timolol19 or the unfixed combination of brimonidine and timolol both dosed twice daily.20,21 Fixed-combination latanoprost and timolol also has been shown to provide diurnal IOP reductions statistically similar to those of the unfixed combination of brimonidine twice daily and latanoprost once daily.22 In contrast, concomitant travoprost once daily in the evening and twice-daily brinzolamide were reported to lower IOP levels more effectively than the once-daily morning administration of fixed-combination latanoprost and timolol23; however, the evening versus morning dosing schedules of travoprost and the fixed combination, respectively, may Table 4. Treatment-Emergent Adverse Events (Safety Population) Fixed Combination (n ⴝ 262) Unfixed Combination (n ⴝ 254) Patients with n (%) No. of Events n (%) No. of Events P Value At least 1 adverse event Ocular adverse events Systemic adverse events Adverse events related to study medication Discontinuation due to an adverse event 44 (16.8) 31 (11.8) 16 (6.1) 21 (8.0) 6 (2.3) 58 39 19 25 6 62 (24.4) 51 (20.1) 17 (6.7) 33 (13.0) 7 (2.8) 91 70 21 45 12 0.04 0.01 0.86 0.08 0.80 74 Diestelhorst and Larsson 䡠 Fixed Combination of Latanoprost and Timolol in the Evening have contributed to this finding. It is notable that in all of these comparisons the fixed combination of latanoprost and timolol was instilled once daily, whereas comparator regimens required 2, 3, or 4 instillations per day. More complex medication regimens have been associated with poorer compliance in patients with glaucoma or ocular hypertension.24,25 As in previous studies,12–14 both the fixed and unfixed combinations of latanoprost and timolol were found to be well tolerated. The fixed combination had a somewhat better tolerability profile, though, possibly because only a single dose of medication was instilled each day, compared with 3 doses for patients in the unfixed-combination group. Although no systemic adverse event was related to study medication, long-term adverse events could be reduced with once-daily dosing of timolol. It is worth noting that the final number of randomized patients was higher than planned due to an unexpectedly high recruitment rate near the end of enrollment and an unexpectedly low attrition rate during screening. The larger sample provided additional power to detect differences between groups if they existed. The research was limited by its relatively short timeframe. Twelve weeks is sufficient to observe changes in IOP levels and to document the presence or absence of many potential adverse events. However, follow-up periods of several years are required to assess differences between therapies with regard to changes in VA or cup-to-disc ratio, the occurrence of long-term side effects, and patient compliance and persistency with treatment. In summary, the fixed combination of latanoprost and timolol applied in the evening is noninferior to the unfixed combination of latanoprost applied in the evening and timolol twice daily. Compared with published data of the fixed combination applied in the morning, our study implies an additional IOP-lowering effect of latanoprost when applied in the evening. The fixed combination provides a once-daily alternative to the 3 instillations needed with the individual components, which may interfere with patient compliance. References 1. Alward WL. Medical management of glaucoma. N Engl J Med 1998;339:1298 –307. 2. Kobelt-Nguyen G, Gerdtham UG, Alm A. Costs of treating primary open-angle glaucoma and ocular hypertension: a retrospective, observational two-year chart review of newly diagnosed patients in Sweden and the United States. J Glaucoma 1998;95–104. 3. European Glaucoma Society. Terminology and Guidelines for Glaucoma. 2nd ed. Savona, Italy: DOGMA, Srl; 2003. 4. Zimmerman TJ, Harbin R, Pett M, Kaufman HE. Timolol and facility of outflow. Invest Ophthalmol Vis Sci 1977;16:623– 4. 5. Zimmerman TJ, Kaufman HE. Timolol. A beta-adrenergic blocking agent for the treatment of glaucoma. Arch Ophthalmol 1977;95:601– 4. 6. Coakes RL, Brubaker RF. The mechanism of timolol in lowering intraocular pressure. In the normal eye. Arch Ophthalmol 1978;96:2045– 8. 7. Arici MK, Sayici M, Toker M, et al. A short term study of the 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. additive effect of timolol and brimonidine on intraocular pressure. Eye 2002;16:39 – 43. Bucci MG, Italian Latanoprost Study Group. Intraocular pressure-lowering effects of latanoprost monotherapy versus latanoprost or pilocarpine in combination with timolol: a randomized, observer-masked multicenter study in patients with open-angle glaucoma. J Glaucoma 1999;8:24 –30. Diestelhorst M, Nordmann JP, Toris CB. Combined therapy of pilocarpine or latanoprost with timolol versus latanoprost monotherapy. Surv Ophthalmol 2002;47(suppl)S155– 61. Rulo AH, Greve EL, Hoyng PF. Additive effect of latanoprost, a prostaglandin F2 alpha analogue, and timolol in patients with elevated intraocular pressure. Br J Ophthalmol 1994;78: 899 –902. Toris CB, Camras CB, Yablonski ME. Effects of PhXA41, a new prostaglandin F2 alpha analog, on aqueous humor dynamics in human eyes. Ophthalmology 1993;100:1297–304. Diestelhorst M, Almegard B. Comparison of two fixed combinations of latanoprost and timolol in open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol 1998;236:577– 81. Higginbotham EJ, Feldman R, Stiles M, et al. Latanoprost and timolol combination therapy versus monotherapy: one-year randomized trial. Arch Ophthalmol 2002;120:915–22. Pfeiffer N, European Latanoprost Fixed Combination Study Group. A comparison of the fixed combination of latanoprost and timolol with its individual components. Graefes Arch Clin Exp Ophthalmol 2002;240:893–9. Diestelhorst M, Larsson LI, European Latanoprost Fixed Combination Study Group. A 12 week study comparing the fixed combination of latanoprost and timolol with the concomitant use of the individual components in patients with open angle glaucoma and ocular hypertension. Br J Ophthalmol 2004;88:199 –203. Alm A, Stjernschantz J, Scandinavian Latanoprost Study Group. Effects on intraocular pressure and side effects of 0.005% latanoprost applied once daily, evening or morning. A comparison with timolol. Ophthalmology 1995;102:1743–52. Konstas AG, Maltezos AC, Gandi S, et al. Comparison of 24-hour intraocular pressure reduction with two dosing regimens of latanoprost and timolol maleate in patients with primary open-angle glaucoma. Am J Ophthalmol 1999;128: 15–20. Konstas AG, Nakos E, Tersis I, et al. A comparison of once-daily morning versus evening dosing of concomitant latanoprost/timolol. Am J Ophthalmol 2002;133:753–7. Shin DH, Feldman RM, Sheu WP, Fixed Combination Latanoprost/Timolol Study Group. Efficacy and safety of the fixed combinations latanoprost/timolol versus dorzolamide/timolol in patients with elevated intraocular pressure. Ophthalmology 2004;111:276 – 82. Garcia-Sanchez J, Rouland JF, Spiegel D, et al. A comparison of the fixed combination of latanoprost and timolol with the unfixed combination of brimonidine and timolol in patients with elevated intraocular pressure. A six month, evaluator masked, multicentre study in Europe. Br J Ophthalmol 2004; 88:877– 83. Stewart WC, Stewart JA, Day D, Sharpe ED. Efficacy and safety of timolol maleate/latanoprost fixed combination versus timolol maleate and brimonidine given twice daily. Acta Ophthalmol Scand 2003;81:242– 6. Stewart WC, Stewart JA, Day DG, et al. Efficacy and safety of the latanoprost/timolol maleate fixed combination versus concomitant brimonidine and latanoprost therapy. Eye 2004;18: 990 –5. Martinez-de-la-Casa JM, Castillo A, Garcia-Feijoo J, et al. Concomitant administration of travoprost and brinzolamide 75 Ophthalmology Volume 113, Number 1, January 2006 versus fixed latanoprost/timolol combined therapy: threemonth comparison of efficacy and safety. Curr Med Res Opin 2004;20:1333–9. 24. Kass MA, Gordon M, Morley RE Jr, et al. Compliance with topical timolol treatment. Am J Ophthalmol 1987;103:188 –93. 25. Gurwitz JH, Glynn RJ, Monane M, et al. Treatment for glaucoma: adherence by the elderly. Am J Public Health 1993;83:711– 6. Appendix: Members of the European–Canadian Latanoprost Fixed Combination Study Group Canada Iqbal Ahmed, MD, Mississauga; Pierre Blondeau, MD, Sherbrooke; Shawn Cohen, MD, Montreal; Robert G. Douglas, MD, Burnaby; Oscar P. Kasner, MD, Montreal; Thomas Klein, MD, Brampton; Frederic Lord, MD, Montreal; Donald Nixon, MD, Barrie; Kevin Parkinson, MD, Coquitlam; Paul Rafuse, MD, Halifax; Aaron Wolfe Rifkind, MD, Hamilton; David Paul Tingey, MD, London; David B. Yan, MD, Mississauga. Germany Andreas Bayer, MD, Weilheim; Hartmut Benning, MD, Mainz; Thomas Christ, MD, Schorndorf; Michael Diestelhorst, MD, Köln; Joachin Floren, MD, Gladbach; Anselm Grundler, MD, Erlangen; Thomas Hamacher, MD, Starnberg; Cornelia Herschel, MD, Köln; Konstantin Papakostas, MD, Gummersbach; Klaus Rosbach, MD, Mainz; MariaLuise Scherzer, MD, Regenstauf. 76 Greece Konstandinos Georgakopoulos, MD, Rio Patra; Stavros Giannikakis, MD, Athens; Konstandinos Karabatsas, MD, Larissa; Emmanouil Vaikousis, MD, Piraeus. Italy Maria Teresa Dorigo, MD, Padova; Enrico Gandolfo, MD, Brescia; Leonardo Mastropasqua, MD, Chieti; Ugo Menchini, MD, Firenze; Nicola Orzalesi, MD, Milano. The Netherlands Catharina E. De Graaf-Kret, MD, Rijswijk; H. Ferdinand A. Duijm, MD, Zwolle; Jan-Peter Flipse, MD, Bergen op Zoom; Antoinette G. J. E. Niessen, MD, Schiedamse Vest; Erik J. G. M. van Oosterhout, MD, Eindhoven; Henricus G. N. Veraart, MD, Tilburg; Herman A. Wessels, MD, Roosendaal. Spain Alfonso Arias, MD, Madrid; Elena Arrondo, MD, Barcelona; Jose Isidro Belda, MD, Alicante; Julio De La Camara, MD, Barcelona; Soledad Jimenez, MD, Cádiz; Mercedes Lasso, MD, Vizcaya; Francisco Munoz Negrete, MD, Madrid; Aureli Rilo, MD, Barcelona; Ana Isabel Vazquez, MD, Málaga; Jaume Vila, MD, Manacor (Palma de Mallorca). Sweden Albert Alm, MD, Uppsala; Adnan Chatila, MD, Orebro; Enping Chen, MD, Stockholm; Mazhar Ghawji, MD, Skövde.