Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
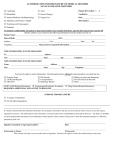
QUARTERLY THERAPIST REPORT HAVEN ID #: ___________________ Quarterly Report: January to March April to June July to September October to December (Circle applicable period) 1. State the frequency of therapy sessions. ____________________________________________________________________________ 2. Has the frequency of therapy sessions been changed in the last quarter, and if so, is this change based on your recommendation? ____________________________________________________________________________ 3. Please list the current medications identified in your records for this professional? ____________________________________________________________________________ 4. Has this health care professional been compliant with treatment and therapy? ____________________________________________________________________________ 5. Since the last report, have you referred this health care professional to any other health care professional for care and treatment? ____________________________________________________________________________ 6. If you have made such a referral, please state the name and address of the professional to whom referral was made and the reason for referral. ____________________________________________________________________________ ____________________________________________________________________________ 7. From a therapeutic perspective, is this professional able to practice with reasonable skill and safety? ____Yes _____No Please use the space below and or attach an additional page to provide a confidential statement regarding this professional’s ability to practice with reasonable skill and safety. ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ _________________________________ _________________________________ Printed Name and Title of Person Completing Report Signature Date: ____________________________ Address: ________________________________ ________________________________________ Telephone: _________________________ Fax: _______________________________ Reports are due following the completion of each quarter, by April 15, July 15, October 15, and January 15, respectively. Please submit reports to: HAVEN, 835 West Queen St. 2nd Floor Southington, CT 06489 (860) 276-9196 Dedicated Fax (860) 276-9202 This information has been disclosed to you from records protected by State and Federal confidentiality rules including 42 CFR Part 2 and Conn. Gen. Stat. Sec. 19a-12a. State and Federal rules prohibit you from making any further disclosure of this information unless further disclosure is expressly permitted by the written consent of the person to whom it pertains or as otherwise permitted by 42 CFR Part 2 and State law. A general authorization for the release of medical or other information is NOT sufficient for this purpose. The Federal rules restrict any use of the information to criminally investigate or prosecute any alcohol or drug abuse patient. This information is also protected from disclosure under State law and information contained herein may not be reproduced or disclosed unless otherwise required by law.