Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
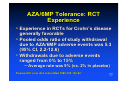
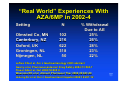
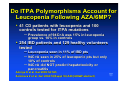
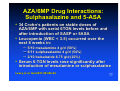
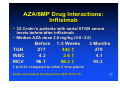
Azathioprine: Long-Term Side Effects Edward V Loftus, Jr, MD Division of Gastroenterology and Hepatology Mayo Clinic College of Medicine Rochester, MN Overview • “Real world” experiences with AZA • ITPA polymorphisms • Hematological – Drug interactions • Teratogenicity/Pregnancy Safety • Hepatic • Infectious – Combination therapy with infliximab • Neoplastic (e.g., lymphoma) AZA/6MP Tolerance: RCT Experience • Experience in RCTs for Crohn’s disease generally favorable • Pooled odds ratio of study withdrawal due to AZA/6MP adverse events was 5.3 (95% CI, 2.2-12.6) • Withdrawals due to adverse events ranged from 0% to 15% – Average rate was 9% (vs. 2% in placebo) Pearson DC et al, Ann Intern Med 1995;123:132-42 “Real World” Experiences With AZA/6MP in 2002-4 Setting Olmsted Co, MN Canterbury, NZ Oxford, UK Groningen, NL Nijmegen, NL N 102 216 622 318 50 % Withdrawal Due to AE 25% 26% 28% 23% 22% Loftus CG et al, Am J Gastroenterology 2003 abstract Gearry et al, Pharmacoepidemiol Drug Safety 2004;13:563-7 Fraser AG et al, Gut 2002;50:485-9 Weersma RK et al, Aliment Pharmacol Ther 2004;20:843-50 deJong DJ et al, Eur J Gastroenterol Hepatol 2004;16:207-12 Inosine Triphosphate Pyrophosphatase (ITPA): Role in AZA/6MP Metabolism 6-thio-IDP 6-thio-ITP 6MMP ITPA TPMT AZA 6MP HPRT 6-thio-IMP XO 6-thio-uric acid IMPDH TPMT Me-6-thio-IMP Marinaki et al, Pharmacogenetics 2004;14:181-7 6-TGNs Inosine Triphosphate Pyrophosphatase (ITPA) Polymorphisms May Explain Some “Idiosyncratic Reactions” to AZA/6MP • 62 IBD pts with adverse reactions to AZA, 68 pts who tolerated > 3 months • ITPA polymorphism (94C>A) significantly associated with adverse events overall • 94C>A 17% allele frequency vs. 4% in controls (OR, 4.2, 95% CI 1.6-11.5) – Flu-like symptoms: OR 4.7, 1.2-18.1 – Rash: OR, 10.3, 4.7-62.9 – Pancreatitis: OR, 6.2, 1.1-32.6 Marinaki et al, Pharmacogenetics 2004;14:181-7 Do ITPA Polymorphisms Account for Leucopenia Following AZA/6MP? • 41 CD patients with leucopenia and 100 controls tested for ITPA mutations – Prevalence of 94C>A was 15% in leucopenia group vs. 10% in controls • 254 IBD patients and 129 healthy volunteers tested – Leucopenia seen in 11% of IBD pts – 94C>A seen in 25% of leucopenic pts but only 10% of controls – 94C>A did NOT predict hepatotoxicity or pancreatitis Allorge D et al, Gut 2005;54:565 Zelinkova Z et al, Gut 2004;53(Suppl VI):A49 (UEGW abstract) Hematological Adverse Events • Variations in TPMT activity may explain only a small proportion of leucopenia, usually only early events • TPMT deficiencies explained only 27% of leucopenic events in a French study • Role of ITPA mutations remains unclear • Continued indefinite need for periodic monitoring of WBC even if counts have been stable Colombel JF et al, Gastroenterology 2000;118:1025-30. AZA/6MP Drug Interactions: Sulphasalazine and 5-ASA • 34 Crohn’s patients on stable doses of • AZA/6MP with serial 6TGN levels before and after introduction of SASP or 5ASA Leucopenia (WBC < 3.5) occurred over the next 8 weeks in: – 5/10 mesalamine 4 g/d (50%) – 6/11 sulphasalazine 4 g/d (54%) – 2/10 balsalazide 6.75 g/d (20%) • Serum 6-TGN levels rose significantly after introduction of mesalamine or sulphasalazine Lowry et al, Gut 2001;49:656-64. AZA/6MP Drug Interactions: Infliximab • 32 Crohn’s patients with serial 6TGN serum • levels before/after infliximab Median AZA dose 2.8 mg/kg (0.6–3.6) TGN WBC MCV Before 277 4.3 96.1 1-3 Weeks 442 † 3.6 † 98.3 † † p<0.01 compared to other 2 time points Roblin et al, Aliment Pharmacol Ther 2003;18:917-25. 3 Months 279 4.1 95.3 AZA Effects on Fertility in Males • 18 men with IBD on AZA for > 3 months – Semen quality as measured by total sperm county, density, motility, and morphology was normal • 11 men with IBD started on AZA after first semen analysis – Baseline parameters slightly decreased – No worsening in parameters after mean 11 months AZA treatment • 6 men on AZA fathered 7 healthy children Dejaco et al, Gastroenterology 2001;121:1048-53. AZA/6-MP Teratogenicity • Metabolites can cross the placenta • Biggest/best studies in transplant and • rheumatology (SLE) literature 146 kidney transplant recipients on AZA/steroids or AZA alone – Low birth weights in 39% – Premature births in 52% – Congenital anomalies in 4% (background rate = 3%) • IBD-specific studies are hampered by small numbers Armenti et al, Transplantation 1994 AZA/6MP During Pregnancy in IBD New York 1950s-1997 A B1 B2 C Pregnancies, n 84 61 15 165 Full term (%) 63% 72% 67% 75% 5% 5% 27% 4% 23% 16% 7% 19% 15%–40% Congenital abnormalities (%) 4% 3% 7% 4% 2%–5% Neonatal/child infections(%) 1% 2% 13% 1% 2%–12% Neoplasia in child 0% 2% 0% 0% 0.1/106/yr Prematurity (%) Spontaneous abortion (%) Normal 7.1% Multivariate analysis: successful pregnancy outcome on 6MP, 0.8 (0.5-1.5) A=conceived after 6-MP; B1=stopped 6-MP when pregnant; B2=continued 6-MP while pregnant; C=pregnancy before starting 6-MP(control) Francella et al.Gastroenterology 2003;124:9-17 Pregnancy Following 6MP, New York, 1982-97 Group 1 n = 29 Pregnancies 72 Live Births 51 (71%) Spont Abs 16 (22%) Stillbirths 1 (1%) Ectopic 2 (3%) Prematurity 4 (8%) Low Birth Weight 4 (8%) Cong Anomaly 3 (6%) Fetal demise 29% Complications 15% Group 2 n = 75 140 120 (86%) 18 (13%) 2 (1%) 0 8 (7%) 8 (7%) 4 (3%) 14% 10% Zlatanic J et al, J Clin Gastroenterol 2003;36:303-9. Gen pop 85% 12% 1% 2% 11% 7% 5% 15% 16% Azathioprine and 6MP in PregnancyNorth Jutland, Denmark, 1991-2000 Low Birth weight Pre-term Birth Congenital Anomalies Perinatal Death First Entire Not Trim. Preg Exposed n=9 n=10 n=19,418 OR, All Controls (95% CI) 22% 30% 4.4% 3.8 (0.4-33) 2.3 (0.4-14) 22% 30% 5.5% 6.6 (1.7-26) 2.8 (0.4-19) 22% 20% 3.7% 20 (2.5-161) 3.2 (0.2-57) 11% 10% 0.6% 6.7 (1.4-32) 7.7 (0.6-102) Norgard et al, Aliment Pharmacol Ther 2003;17:827-34 OR, AZA/6MP Controls (95% CI) AZA/6MP: Infectious Complications • Lenox Hill Hospital 1980-99 (n = 410) • Infections, not necessarily related to leucopenia, may occur in up to 14% • Pneumonia 4% • Herpes zoster 3% • Cytomegalovirus infections (colitis, hepatitis, systemic illness) < 1% • Upper respiratory infections 7% Warman JI et al, J Clin Gastroenterol 2003;37:220-5. Combination Purine Analog and Anti-TNF Therapy: Does It Synergistically Increase Infection Risk? • Many centres advocate combination therapy to • • reduce formation of antibodies to infliximab Does this increase infection risk? 217 IBD patients from Stockholm – 18 severe infections (8%) – 2 sepsis deaths • 500 Crohn’s patients from Mayo – 41 infections (8%) – 2 sepsis deaths, 2 pneumonia deaths Ljung T et al, Gut 2004 Colombel JF et al, Gastroenterology 2004 AZA/6MP Hepatotoxicity • Overall prevalence of biochemical abnormalities: 3-4% • Most of these are dose-dependent – Related to over-accumulation of 6MMP due to high TPMT? Controversial – May resolve spontaneously or with dose reduction • 6-thioguanine: fewer allergic side effects, more hepatotoxicity (up to 26%) Dubinsky MC et al, Gastroenterology 2002;122:904-15 Dubinsky MC et al, Gastroenterology 2003;125:298-303 AZA/6MP Hepatotoxicity Less common but more serious: Nodular regenerative hyperplasia Veno-occlusive disease of liver True incidence of these events remains unknown Reticulin stain Holtmann M et al, Dig Dis Sci 2003 Daniel F et al, Gut 2004;53 (Suppl VI):A221 Baseline Risk of Lymphoma in IBD • Studies from referral centers indicate a twofold to six fold increase in risk – Referral bias? – Risk increases with increased severity? • Population-based studies indicate little or no increased risk, with few exceptions Population-Based Studies of Lymphoma in IBD Author Ekbom Persson Karlen Loftus Palli Bernstein Lewis Askling Setting Uppsala Patients CD 1655 UC 3121 Stockholm CD 1251 Stockholm UC 1547 Olmsted Co CD 216 UC 238 Florence CD 231 UC 689 Manitoba CD 2857 UC 2672 GPRD, UK CD 6605 UC 10391 Mult Swedish CD 20120 cohorts UC 27559 RR 0.4 1.2 1.4 1.2 2.4 0 2.5 9.3* 2.4 1.0 1.4 1.2 1.3 1.0 (95% CI) (0 - 2.4) (0.5 - 2.4) (0.4 - 3.5) (0.3 - 3.5) (0.1 - 13) (0 - 6.4) (0.3 - 9) (2.5 - 24) (1.2 - 5) (0.5 - 2.2) (0.5 - 3.4) (0.7 - 2.1) (1.0 - 1.6) (0.8 - 1.3) * Hodgkin lymphoma (RR not signif elevated for non-Hodgkin) Ekbom, Cancer 1991; Persson, Gastroenterology 1994; Karlen, Am J Gastroenterol 1999; Loftus, Am J Gastroenterol 2000; Palli, Gastroenterology 2000; Bernstein, Cancer 2001; Lewis, Gastroenterology 2001; Askling, Gut 2005 Lymphoma Risk in IBD Patients on AZA/6MP: Meta-Analysis Study Setting N Obs Exp SIR (95% CI) Kinlen U.K. 321 2 0.16 12.5 (1.2 - 46) Connell London 755 0 0.52 0 Farrell Dublin 238 2 0.05 37.5 (3.5 - 138) Fraser Oxford 626 3 0.65 4.6 (0.9 - 13.7) Korelitz New York 486 3 0.61 4.9 (0.9 - 14.5) Lewis GPRD 1465 1 0.64 1.6 (0.001 - 9) 3891 11 2.63 4.2 (2.1 - 7.5) Pooled Sensitivity analyses: when papers with highest or lowest SIRs were excluded, results remained significant (range, 3.5 - 5.2) Kandiel et al, DDW abstract 2004 and Gut 2005 (in press) Epstein-Barr Virus and Lymphoma B-cell lymphoma EBV in-situ hybridization Dayharsh et al, Gastroenterology 2002;122:72 EBV Virus Load 138 Crohn’s patients with serial EBV viral load measurements 2 pts had viral loads in dangerous range (i.e., risk for lymphoma) No clear relationship between immunosuppressive therapy and EBV loads Reijasse et al, Inflamm Bowel Dis 2004;10:85 Risk-Benefit of AZA/6MP for Crohn’s: Decision Analysis • Markov model of quality-adjusted life year gain of AZA • • • for Crohn’s in a 35 year-old patient Base case assumed 3 fold increased lymphoma risk and a 50% reduction in Crohn’s related mortality 10 years of AZA resulted in gain of 1.25 qualityadjusted months AZA was no longer beneficial if: – – – – Risk of death from severe flare < 0.06% Lymphoma risk is > 8 times normal Background risk of lymphoma in Crohn’s > 4 times normal Fear of AZA-related lymphoma results in > 1% decrease in utility (proxy for QOL) Lewis JD et al, Gastroenterology 2000;118:1018-24. Does Prolonged Leukopenia Increase Cancer Risk With 6MP? • 600 IBD pts treated with 6MP at Lenox Hill • • • Hospital, New York 31 pts developed sustained leukopenia (WBC < 4 for at least 2.5 wks) 93 matched controls without leukopenia 8 developed cancers (26%) versus 8% in controls (p = 0.017) – Leukemia in 2 – Non-Hodgkin lymphoma in 1 – No colorectal cancers DiSanti et al, Am J Gastroenterol 2004;99:S252 (ACG abstract) Risk of Other Cancers With AZA/6MP • Non-melanoma skin cancer, especially squamous cell cancer – In transplant literature, RR is 6 to 65 – Might increase further with addition of ciclosporin • Many IBD cohort studies show increased risk of colorectal cancer following AZA/6MP, but this is to be expected given the extent and duration of colitis Conclusions (1) • Tolerance of AZA/6MP in the “real world” may • • • not be as good as RCT data (22 – 28% withdrawal rates) “Newer” polymorphisms such as ITPA may explain some toxicity such as fever and pancreatitis – data are conflicting Drug interactions between AZA/6MP and 5ASA or infliximab may result in leucopenia Data on safety in pregnancy are sparse – may be a small but real risk of adverse outcome – discuss with the patient Conclusions (2) • Most hepatotoxicity is mild and reversible but rarely more serious injury may occur • Most population-based studies of lymphoma in IBD suggest little to no increased relative risk • Relative risk of lymphoma with AZA/6MP use is likely increased, up to fourfold absolute risk remains low • Epstein-Barr virus typically found in lymphomas in IBD pts on AZA/6MP