Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
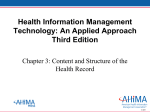
MEDICAL CERTIFICATION FOR MEDICAID LONG-TERM CARE SERVICES AND PATIENT TRANSFER FORM *Patient Name: *Last 4 SSN: *A. PATIENT INFORMATION *Gender: Male Female *Hispanic Ethnicity: Yes No *Race: White Black Other: *Language: English Other: *B. SIGHT HEARING Normal Deaf Impaired Normal Impaired R Hearing Aid L Blind C. DECISION MAKING CAPACITY (PATIENT) Capable to make healthcare decisions Requires a surrogate *D. EMERGENCY CONTACT Name: Name: Phone: Phone: *E. MEDICAL CONDITION *Primary diagnosis: *Other diagnoses: I. TRANSFERRED FROM Facility Name: Unit: Date: Fax: Phone: Discharge Nurse: Phone: Discharge Date: Admit Date: Discharge Time: AM PM AM PM Admit Time: J. TRANSFERRED TO Facility Name: Address 1: Address 2: Fax: Phone: K. PHYSICIAN CONTACTS Primary Care Name: Phone: Hospitalist Name: Phone: L. TIME SENSITIVE CONDITION SPECIFIC INFORMATION Medication due near time of transfer / list last time administered Script sent for controlled substances (attached): Yes No PM AM Anticoagulants Date: Time: PM AM Antibiotics Date: Time: PM AM Date: Time: Insulin PM AM Other: Date: Time: Has CHF diagnosis: Yes No If yes; new/worsened CHF present on admission? Yes No Last echocardiogram: Date: LVEF % On a proton pump inhibitor? Yes No If yes, was it for: In-hospital prophylaxis and can be discontinued Specific diagnosis: If Hospitalized: Primary diagnosis at discharge: Reason for transfer: Surgical procedures performed: F. INFECTION CONTROL ISSUES PPD Status: Positive Negative Not known Screening date: Associated Infections/resistant organisms: MRSA Site: Site: VRE Site: ESBL MDRO Site: Site: C-Diff Other: Site: Isolation Precautions: None Contact Droplet Airborne *G. PATIENT RISK ALERTS *None Known *Harm to self *Difficulty swallowing *Seizures *Elopement *Harm to others *Pressure Ulcers *Falls *Other: RESTRAINTS: Yes No Types: Reasons for use: ALLERGIES: Latex Allergy: None Known Yes Yes, List below: No Dye Allergy/Reaction: H. ADVANCE CARE PLANNING Please ATTACH any relevant documentation: Advance Directive Yes No Living Will Yes No DO NOT Resuscitate (DNR) Yes No DO NOT Intubate Yes No DO NOT Hospitalize Yes No No Artificial Feeding Yes No Hospice Yes No Yes On one or more antibiotics? If yes, specify reason(s): *DOB: Yes No Any critical lab or diagnostic test pending at the time of discharge? Yes No If yes, please list: M. PAIN ASSESSMENT: Pain Level (between 0 - 10): AM Time: Last administered: Date: PM *N. FOLLOWING REPORTS ATTACHED No Physicians Orders Treatment Orders Discharge Summary Includes Wound Care Medication Reconciliation Lab reports EKG Discharge Medication List X-ray MRI PASRR Forms CT Scan Social and Behavioral History History & Physical *ALL MEDICATIONS: (MUST ATTACH LIST) (JUN 2016) AHCA Form 5000-3008, ________________, incorporated by reference in Rule 59G-1.045, F.A.C. *Data required for Medicaid MEDICAL CERTIFICATION FOR MEDICAID LONG-TERM CARE SERVICES AND PATIENT TRANSFER FORM *Last 4 SSN: *Patient Name: O. VITAL SIGNS Date: Time Taken: WT: HT: Temp: BP: HR: RR: *P. PATIENT HEALTH STATUS *Bladder: Continent Incontinent Ostomy Catheter Type: FEET AM T. SKIN CARE – STAGE & ASSESSMENT Pressure Ulcers (Indicate stage and location(s) of lesions using corresponding number: PM INCHES / 1. Sp02: 2 3. date inserted: Foley Catheter: Yes No If yes, date inserted: Indications for use: Urinary retention due to: Monitoring intake and output Skin Condition: Other: Attempt to remove catheter made in hospital? Date Removed: *Bowel: Continent Incontinent Ostomy List any other lesions or wounds: Yes *U. MENTAL / COGNITIVE STATUS AT TRANSFER Alert, oriented, follows instructions Alert, disoriented, but can follow simple instructions No Alert, disoriented, and cannot follow simple instructions Not Alert V. TREATMENT DEVICES Heparin Lock - Date changed: IV / PICC / Portacath Access - Date inserted: Type: Internal Cardiac Defibrillator Pacemaker Wound Vac Other: Respiratory - Delivery Device: CPAP BiPAP Nebulizer Other: Nasal Cannula Mask: Type Oxygen - liters: % PRN Continuous Trach Size: Type: Ventilator Settings: Suction Date of Last BM: Immunization status: Influenza: Yes No Date: Pneumococcal: Yes No Date: *Q. NUTRITION / HYDRATION *Dietary Instructions: Tube Feeding: G-tube J-tube PEG Insertion Date: Supplements (type): TPN Other Supplements: Self Assistance Difficulty Swallowing Eating: R. TREATMENTS AND FREQUENCY PT - Frequency: OT - Frequency: Speech - Frequency: Dialysis - Frequency: *S. PHYSICAL FUNCTION Ambulation: *Ambulation: *Transfer: Self Not ambulatory Assistance Ambulates independently 1 Assistant Ambulates with assistance 2 Assistants Ambulates with assistive device Devices: Weight-bearing: Wheelchair (type): Left: Appliances: Full Partial None Prosthesis: Right: Lifting Device: Full Partial None *Y. PHYSICIAN CERTIFICATION W. PERSONAL ITEMS Artificial Eye Contacts Eyeglasses Dentures U L Partial Printed Name: Rehab Potential (check one) Good Fair Poor *Physician/ARNP/PA License #: *Date: *Phone Number: *Printed Physician/ARNP/PA Name & Title: Name: Walker Other Signature: *Physician/ARNP/PA Signature: Z.PERSON COMPLETING FORM Prosthetic Cane Crutches Hearing Aids L R X. COMMENTS (Optional) *I certify the individual requires nursing facility (NF) services. The individual received care for this condition during hospitalization. *I certify the individual is in need of Medicaid Waiver Services in lieu of nursing facility placement. *Effective date of medical condition: *DOB: Phone Number: (JUN 2016) AHCA Form 5000-3008, ________________, incorporated by reference in Rule 59G-1.045, F.A.C. Date: * Sections required for Medicaid