Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
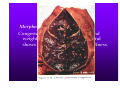
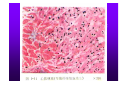
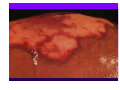
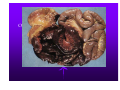
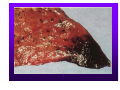
PATHOLOGY 周 韧 ZHOU REN Prof., M.D.,Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology, Zhejiang University Judicial Evidence & Evaluation Center Zhejiang University School of Medicine Chapter 3. Disorder of vascular flow Disorder of vascular flow may be divided into general and local categories. The local disorders contain: ①Derangement of local blood volume: hyperemia and ischemia, ②Derangement of blood properties and content: thrombosis, embolism and infarction. ③Derangements of vascular permeability and anatomic integrity: edema, hemorrhage. Hyperemia Def. Hyperemia refers to a local increased volume of blood caused by dilatation of the small vessels. 1. Arterial hyperemia (active hyperemia) It results from an augmented arterial inflow, such as occurs in the muscles during exercise, at sites of inflammation, and in the pleasing neurovascular dilatation termed blushing. Active hyperemia causes increase of the volume of local tissue, of the metabolism and function of the organ. It is beneficial to the organism. Active hyperemia of body surface shows red in color and increase in local temperature. 2. Venous hyperemia (passive hyperemia, congestion) It results from diminished venous flow such as follows cardiac failure or obstructive venous disease. Etiology (1)Compression on vein (2)Intravenous obstruction (3)Cardiac failure Morphology Congested organ increases in size and weight, solidifies in consistence, and shows dark color and capsular stiffness. Chronic congestion of lung Chronic congestion of liver Chronic congestion of liver Hemorrhage Def. Hemorrhage refers to extravasation of blood caused by rupture of blood vessel. Hematoma: Accumulation of large amount of blood within the tissue of the body. Hemothorax, hemopericardium, hemoperitoneum, hemarthrosis: blood accumulation in body cavities as thoracic cavity, pericardial cavity, Peritoneal cavity and arthritic cavity respectively. Petechiae: Minute hemorrhage into skin, mucous membrane or serosal surface. Purpura: Slight larger hemorrhage. Ecchymosis: A large subcutaneous hematoma. Thrombosis Def. Thrombosis refers to the process of formation of an adherent clotted mass of blood within the cardiovascular system in a living body. 1. Factors and mechanism of thrombosis (1)Endothelial injury On the one hand, endothelial cells possess antiplatelet, anticoagulant, and fibrinolytic properties; on the other hand they exert procogulant functions. Intact endothelium insulates the blood platelets and coagulation proteins from the highly thrombogenic subendothelial components, principally collagen. Damage to vascular endothelium is the dominant influence thrombogenesis, and the only one which, by and of itself, may lead to thrombus formation. It may occur in the following situations: ulcerated atherosclerotic plaques; vascular traumatic or inflammatory injury; endocardium in the site of myocardial infarction or myocarditis. (2)Alteration of blood flow (stasis and turbulence) In normal laminar blood flow, all of the formed elements are separated from the endothelial surface by a clear plasmatic zone. ①disrupt laminar flow and permit platelets to come into contact with the endothelium; ②prevent dilution of activated clotting factors to subcritical concentrations; ③retard the inflow of clotting factor inhibitors; ④permit the build-up of platelets aggregates and nascent fibrin either in the sluggish stream or in the pockets of stasis; ⑤promote endothelial cell hypoxia and injury, predisposing to platelet and fibrin deposition as well as reducing release of TPA; ⑥the turbulence is a mechanism for endothelial injury. (3)Hypercoagulability Hypercoagulability can be defined as an alteration of the blood or , specifically, the clotting mechanism that in some way predisposes to thrombosis. Hypercoagulability can be seen in many clinical settings such as severe trauma, burns, disseminated cancer, long term use of oral contraceptives. Morphogenesis of thrombi ①Endotbelial injury→platelets adhesion and aggregation. Platelets activation→release reaction (ADP, TxA2, 5-HT)→platelet aggregation. ②Intrinsic and extrinsic coagulation sequence: prothrombin→thrombin ↓ fibrinogen ———→fibrin White thrombus (head of thrombus): dry, friable gray mass transection: darker gray lines of platelets (Zahn’s line) H. Platelet trabeculae formation z mixed thrombus (body) White thrombus intermingled with red thrombus z Dark red in color, laminations are not well developed and composed of RBC and fibrin z red thrombus (tail) : 3. Types of thrombi (1)Arterial thrombi ①Mural thrombi ②Ball thrombi ③Occlusive thrombus (2)Venous thrombus (3)Vegetations The potential outcomes of thrombus: (1)Softening, liquefaction and absorption (2)Detachment of thrombus followed by thromboembolism (3) Organization and recanalization (3) Organization and recanalization (4)Calcification Microcirculatory Thrombosis(DIC) Def. Widespread thrombosis in the microcirculation is referred to disseminated intravascular coagulation(DIC). Etiology and mechanism DIC is not a primary disease, rather, it is a complication of some underlying diseases (trauma, severe infection, shock, carcinoma etc.) which activate the processes involved in blood clotting. The simplest mechanism involves the release of tissue factor into the circulation, for example, from the placenta in obstetric complication. Carcinomas may also release other thromboplastic substances such as proteolytic enzymes etc. Morphology The microthrombi are composed of platelets and fibrin and are found principally in the arterioles and capillaries of the kidney, adrenals, brain and heart. The bleeding tendency is probably attributable to the rapid consumption of platelets and clotting factors; hence DIC is sometimes also referred to defibrillation syndrome or consumption coagulopathy. Embolism Def. Embolism refers to occlusion of some part of the cardiovascular system by any foreign mass carried there in the blood stream. The transported mass is called as embolus. 1. Routes of embolus transportation (1)Arterial emboli induce embolism in brain, kiney, spleen and lower limbs. (2)Venous emboli usually lodge in the lung. (3)Paradoxical embolism: In case of congenital septum defect of the heart, venous emboli may enter from the right into the left heart chambers. (4)Retrograde embolism: Emboli occasionally may travel against the direction of blood flow. 2. Types of emboli (1)Thromboembolism ①Pulmonary embolism most commonly originates from thrombus of lower limb. The prognosis depends on the size of the occluded vessel and the status of the patient’s cardiovascular system. Large embolus: fatal. Mechanical obstruction + severe strain on the right side of the heart (acute cor pulmonale) + reflexive vascular and bronchial spasm. Small emboli obstruct small branches of pulmonary artery: The thrombi can be resolved and so of little significance. If bronchial circulation is insufficiency (chronic passive congestion of lung), small emboli may produce either pulmonary hemorrhage or infarction ②Arterial embolism Origin: Emboli usually arise from mural thrombi in the left ventricle or atrium, from vegetations on the left side valves, and occasionally from thrombi on the aorta. Morphology: They produce occlusion of blood stream most frequently in the spleen, the kidneys, the brain, and lower extremities, often with resultant infarcts in the organs and gangrene in the limbs. (2)Fat embolism Etiology: Fracture of the shafts of long bones, soft tissue trauma, burns. Morphology: Sequences: The prognosis of fat embolism depends on the quantity and site of embolism. ①Pulmonary fat embolism: 9~20g fat→75% pulmonary arteries are occluded→pulmonary edema, hemorrhage, atelectasis→asphyxia, right sided heart failure. ②Lung-brain-kidney-skin embolism syndrome (3)Gas embolism ①Air embolism Etiology: As a complication of trauma (chest), cardio-thoracic surgery, various diagnostic or therapeutic procedures, or rupture of veins during delivery. Sequences: Small volume: absorbed >100ml: acute distress. >300ml: fatal due to pulmonary embolism. ②Decompression sickness (cassion disease) Etiology and mechanism: Decompressed rapidly from high atmospheric pressure to a normal level of pressure (in deep sea divers, in underwater construction workers) or from normal atmospheric pressure to a low pressure (in aviators)→Gas comes out of solution in the blood, tissue fluid, and fat, in the form of minute bubbles which are composed of O2, CO2 and nitrogen. The nitrogen is of low solubility and persists as minute bubbles. (4)Amniotic fluid embolism Etiology and mechanism: After rupture of membranes, some of the amniotic fluid may be forced by vigorous uterine contractions between the membranes and the uterine wall and then up to the placentar margin to enter the uterine sinusoids. It is now suspected that vasoactive substances within the amniotic fluid such as prostaglandins may be the cause of pulmonary vasoconstriction. Morphology: The classic findings in the pulmonary arteries and capillaries at autopsy are epithelial squames from fetal skin, lanugo hairs, fat from vernix caseosa, and mucin, presumed to be from the fetal GIT. Infarction Def. Ischemic necrosis of tissue or organ caused by occlusion of either its arterial supply or its venous drainage is referred to infarct, the process of infarct formation is called as infarction. 1. Causes and factors that condition the development of an infarct (1)Nature of vascular supply ①Effective anastomosis ②Double blood supply (liver, lung etc) (2)Rate of development of occlusion (3)Vulnerability of the organ or tissue to hypoxia (nerve cells, myocardial muscle>fibroblasts) (4)Oxygen carrying capacity of blood: The anemia or cyanotic patient tolerates arterial insufficiency less well than does the normal person. 2. Types (1)White infarct: It result of arterial occlusion, commonly seen in compact, solid organs with less collateral circulation, such as the kidneys, spleen and heart. (2)Red infarct: Red infarct of intestine: Limited venous outflow due to vascular obstruction + by pass channels can’t develop. 3. Morphology G. All infarcts, red and white, tend to be wedge shape, the occluded vessel at the apex and the periphery of the organ forming the base. Shortly after the vascular obstruction, the area involved becomes red and congested as a result of dilatation of the vessels and flowing of blood into the part from adjacent vessels. Hemorrhage occurs as a result of ischemic damage to vessel wall. Compact organs have relative little hemorrhage, the necrotic area is gradually decolorized (rbc are lysed and removed from the area), and appears pale or yellow-white (white infarct). Organs of soft, loose tissue with double supply, infarcts tend to remain hemorrhagic (Red infarct) Pulmonary hemorrhagic infarct H. Necrotic tissue surrounding with hyperemic and hemorrhagic zone. * Septic infarct: When an infarct is produced by a septic embolus, the infarct is converted to an abscess. 4. Fate of infarct (1)Small infarct: softened, absorbed (2)Large infarct: organization and scar formation (3)Septic infarct: abscess formation (4)Infarction of brain, myocardium or lung: sometimes may cause sudden death.