Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
HEMODYNAMIC DISORDERS
EDEMA
Normally,
60% of lean body weight = water
(2/3) intracellular.
(1/3)extracellular (interstitial fluid)
5% blood plasma.
edema = an accumulation of interstitial fluid within
tissues.
Edema ≠ Extravascular fluid collection in body cavities:
- pleural cavity (hydrothorax)
- the pericardial cavity (hydropericardium)
- peritoneal cavity (hydroperitoneum, or ascites).
Anasarca is severe, generalized edema marked by
profound swelling of subcutaneous tissues and
accumulation of fluid in body cavities.
1- Increased Hydrostatic Pressure
Impaired Venous Return
causes
of
edema
Congestive heart failure; Constrictive pericarditis; Ascites (liver
cirrhosis); Venous obstruction or compression; Thrombosis;
External pressure (e.g., mass); Lower extremity inactivity with
prolonged dependency
Arteriolar Dilation
Heat; Neurohumoral dysregulation
2- Reduced Plasma Osmotic Pressure (Hypoproteinemia)
Protein-losing glomerulopathies (nephrotic syndrome)
Liver cirrhosis (ascites); Malnutrition; Protein-losing
gastroenteropathy
3- Lymphatic Obstruction
Inflammatory; Neoplastic; Postsurgical; Postirradiation
4- Sodium Retention
Excessive salt intake with renal insufficiency
Increased tubular reabsorption of sodium; Renal hypoperfusion;
Increased renin-angiotensin-aldosterone secretion
5- Inflammation
Acute inflammation; Chronic inflammation; Angiogenesis
INCREASED HYDROSTATIC PRESSURE-CAUSES
Local
: -impaired venous return- e.g. DVT
Generalized: -congestive heart failure (most
common):
- reduced cardiac output leads hypoperfusion of the
kidneysrenin-angiotensin-aldosterone axis
sodium and water retention (secondary
hyperaldosteronism).
- fluid retention increased venous hydrostatic
pressures worsening edema=(vicious circle)
- Treatment of generalized edema includes:
salt restriction, diuretics, aldosterone antagonists.
REDUCED PLASMA OSMOTIC PRESSURE
common
causes:
1- albumin is lost from the circulation
e.g. nephrotic syndrome loss of albumin (and other
plasma proteins) in the urine .
2- albumin synthesized in inadequate amounts
e.g. severe liver disease (e.g., cirrhosis)
e.g. malnutrition
Unfortunately, increased salt and water retention by
the kidney not only fails to correct the plasma
volume deficit but also exacerbates the edema, since
the primary defect (low serum protein) persists.
LYMPHATIC OBSTRUCTION = LYMPHEDEMA
Causes:
1- localized obstruction by an inflammation or
infection (e.g. filariasis =elephantiasis)
2- neoplastic conditions (e.g. breast cancer:
Infiltration and obstruction of superficial
lymphatics cause edema of the breast’s overlying
skin peau d'orange (orange peel)).
3- post surgical (e.g. breast cancer after axillary
lymph node resection and/or irradiation upper
limb lymphedema
4- irradiation
SODIUM AND WATER RETENTION
leads
to edema by increasing hydrostatic
pressure (due to expansion of the
intravascular volume) and reducing
plasma osmotic pressure.
causes: diseases that compromise renal
function, including poststreptococcal
glomerulonephritis and acute renal failure
CLINICAL CORRELATION OF EDEMA
Subcutaneous edema:
-the most common
-it signals potential underlying cardiac or renal disease
-Can impair wound healing or the clearance of infections.
Pulmonary edema
Common causes: -LVF- renal failure - ARDS –lung
infections or inflammation.
can cause death if impeding oxygen diffusion
Brain edema
- life-threatening brain herniation through the
foramen magnum.
HEMORRHAGE
Hemorrhage is extravasation of blood from
vessels into the extravascular space.
May be:
1. External hemorrhage.
2. Within a tissue (=hematoma)
3. hemorrhage into body cavities;
a. Hemothorax: Blood in the pleural cavity.
b. Hemopericardium: Blood in pericardium.
c. Hemarthrosis : Blood in joints.
4. Small bleeds
I. Petechiae are minute 1-2 mm bleeds in skin or
mucous membranes
II. Purpura are 3 to 5 mm bleeds
III. Ecchymoses : Larger (1- to 2-cm) subcutaneous
hematomas (bruises).
CLINICAL SIGNIFICANCE OF HEMORRHAGE
DEPENDS ON:
1. The volume of and Rate of bleeding
a. Rapid loss of < 20% of the blood volume, or slow
losses of even of larger amounts, may be
insignificant.
b. Greater losses can cause hemorrhagic
(hypovolemic) shock .
2. Site of bleeding:
-Bleeding that would be trivial in the subcutaneous tissues
can cause death if located in the brain .
- Note: Chronic or recurrent external blood loss ( peptic
ulcer or menstrual bleeding) may result in iron deficiency
anemia.
HEMOSTASIS AND THROMBOSIS
Hemostasis
: tightly regulated processes that
maintain blood in a fluid, clot-free state in
normal vessels while inducing the rapid
formation of a localized hemostatic plug at the
site of vascular injury.
The pathologic form of hemostasis is
thrombosis.
Thrombosis: blood clot (thrombus) formation in
uninjured vessels or thrombotic occlusion of a
vessel after relatively minor injury.
Both hemostasis and thrombosis involve three
components: the vascular wall, platelets, and
the coagulation cascade.
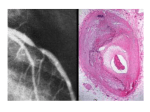
CAUSES OF THROMBOSIS
Virchow's triad:
(1) endothelial
injury
(2) stasis or
turbulence of
blood flow
(3)hypercoagulability
1- Causes of Endothelial injury
1.
2.
3.
4.
5.
6.
7.
8.
9.
Valvulitis (heart valve inflammation)
MI (myocardial infarction)
Atherosclerosis
Traumatic or inflammatory conditions
Increased Blood Pressure
Endotoxins (infections)
Hypercholesterolemia
Radiation
Smoking
2- Stasis and turbulence
-
-
Stasis is a major factor in venous thrombi.
Normal blood flow is laminar (platelets flow centrally in
the vessel lumen, separated from the endothelium by a
slower moving clear zone of plasma).
Stasis and turbulence cause the followings:
3- HYPERCOAGULABILITY
A- Inherited causes of hypercoagulability:
Mutations in the factor V gene and the prothrombin gene are
the most common.
Deficiencies of anticoagulants such as protein C or protein S
(rare)
B. Acquired hypercoagulability
1.Oral contraceptive use and hyperestrogenic state of
pregnancy .
2.Prolonged bed rest or immobilization .
3.Myocardial infarction.
4. Disseminated cancers (e.g. release of mucin in
adenocarcinoma predisposes to thrombus formation
(migratory thrombophlebitis, or Trousseau's syndrome).
FATE OF THE THROMBUS
1. Propagation: accumulation of additional platelets and
fibrin.
2. Embolization: Fragment of thrombus is transported
elsewhere in the vasculature.
3. Dissolution: In newly formed thrombus, due to
activation of fibrinolysis.
4. Organisation and recanalization: Older thrombi
become fibrosed and capillary channels may form and
establish the continuity of the original lumen.
5. Bacterial seeding of thrombus serve as a culture
medium, and the resulting infection may weaken the
vessel wall, leading to formation of a mycotic aneurysm
CLINICAL CORRELATIONS: VENOUS VERSUS
ARTERIAL THROMBOSIS
1- Venous thrombi by obstructing the venus drainage can
cause swelling and edema, but are most worrisome
because they can embolize to the lungs and cause death.
2- Arterial thrombi can embolize. However, they mainly
obstruct vessels (in coronary and cerebral arteries ) to
cause myocardial and cerebral infarction.
Also cardiac thrombi in the setting of myocardial
infarction can give systemic embolization (brain,
kidneys, and spleen).
VENOUS THROMBOSIS
1. Superficial venous thrombi:
- Arise in the saphenous vein particularly in varicose
veins; these rarely embolize but can cause edema from
impaired venous outflow, leading to varicose ulcers.
II. Deep venous thromboses ("DVTs") : Occur in the
larger leg veins at or above the knee ( popliteal, femoral,
veins). May be asymptomatic. Serious because they can
embolize.
EMBOLISM
An
embolus = a detached intravascular solid, liquid, or
gaseous mass that is carried by the blood to a site
distant from its point of origin.
99% of all emboli = a dislodged thrombus
(thromboembolism).
1% = Air embolism, fat embolism, amniotic fluid
embolism.
The consequences of thromboembolism include
ischemic necrosis (infarction) of downstream tissue.
Two
forms of thrmoboembolism:
1.Pulmonary thromboembolism.
2.Systemic thromboembolism
PULMONARY THROMBOEMBOLISM
In 95% of cases, venous emboli originate from DVT.
They are carried through progressively larger channels and pass
through the right side of the heart before entering the pulmonary
vasculature.
clinical features of pulmonary thromboembolism:
a. Clinically silent: 60% to 80% of emboli esp. small ones.
b. Sudden death or right sided heart failure (acute cor
pulmonale):A large embolus that blocks a major pulmonary
artery or pulmonary trunk (saddle embolus)
c. Pulmonary hemorrhage
d- Pulmonary hypertension and chronic right ventricular
failure (chronic cor pulmonale): Multiple emboli occurring
over long time.
SYSTEMIC (ARTERIAL)THROMBOEMBOLISM
-80% arise from intra-cardiac thrombi.
-The remainder originate from aortic aneurysms and
thrombi overlying ulcerated atherosclerotic
plaques.
Common arterial embolization sites :
a. The lower extremities (75%).
b. Central nervous system (10%).
c. Intestines, kidneys, etc : are less common.
-Arterial emboli often cause infarction
INFARCTION
An
infarct is an area of ischemic necrosis caused by
occlusion of either the arterial supply or the venous
drainage in a particular tissue.
99% of all infarcts result from thrombotic or embolic
events.
Infarcts are classified on the basis of their color
(reflecting the amount of hemorrhage) and the
presence or absence of microbial infection. Therefore,
infarcts may be either:
1- Red (hemorrhagic)
2- White (anemic)
also, infarcts may be septic or bland.
Red infarcts
(1) With venous occlusions (such as in ovarian torsion).
(2) In loose tissues (such as lung).
(3) In tissues with dual circulations such as lung and
small intestine.
(4) In tissues that were previously congested because of
sluggish venous outflow.
(5) When flow is re-established to a site of previous
arterial occlusion.
White infarcts
Arterial occlusions or in solid organs (such as heart,
spleen, and kidney), where the solidity of the tissue
limits the amount of hemorrhage
SHOCK
-is the final common pathway for several
potentially lethal events, including hemorrhage,
extensive trauma or burns, MI, pulmonary
embolism, and sepsis, characterized by systemic
hypoperfusion of tissues
- shock initially is reversible, however, prolonged
shock eventually leads to irreversible tissue
injury that often proves fatal.
-The typical signs of shock are low blood
pressure, rapid heart rate, and signs of poor endorgan perfusion (i.e.: low urine output,
confusion, or loss of consciousness).
THE MOST COMMON FORMS OF SHOCK
1- Cardiogenic shock: results from low cardiac output
due to myocardial pump failure. It may be caused
by myocardial damage (infarction), ventricular
arrhythmias, extrinsic compression (cardiac
tamponade)
2- Hypovolemic shock: most common type. Results from
low cardiac output due to loss of blood or plasma
volume (e.g., due to hemorrhage or fluid loss from
severe burns
3- Septic shock: results from arterial vasodilation and
venous blood pooling that stems from the systemic
immune response to microbial infection.