Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Toxicodynamics wikipedia , lookup
Drug design wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Theralizumab wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
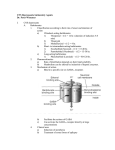
Non-selective CNS depressants ©2010 Mark Tuttle - Effect all CNS functions: motor, sensory, Respiration: depress all 3 mechanisms Tendon reflexes: Hyperreflexia-disinhibition intellectual, autonomic, respiratory, etc. - Neurogenic, CO2 (chemical), O2 (hypoxic) - Disinhibition of ARAS: ↓ filter unwanted Supplying 100% O2 may decrease hypoxic drive - Most sensitive: Fine, learned motor skills and stimuli - Need high dose for effect (unless COPD) higher integrative function - Even high doses: still respond to stimuli - Hyperreactivity of protective reflexis of airway Preferential action: o Consciousness is among most sensitive, (laryngospasm, hiccupping, gagging) disinhibition CNS > peripheral reason for usage Overdose: respiratory death - Least sensitive: Basic protective reflexes. Treatment of overdose: no selective antagonists (antidote), airway, breathing, cardio, drugs (alkaline diuresis, support circulation) NO respir!! Abuse: Used in ways that are not medically approved Tolerance: Escalation of dose to maintain effect Dependence: Drug now required for homeostasis - Barbiturates - Metabolic: induction of hepatic enzymes - Withdrawal syndrome - Ethanol o Hypnotic dose does this o Hyperexcitability of entire CNS - Other non-selective CNS depressants o Relatively unique to barbiturates o At worst: delirium, convulsions, death - Functional: ↓ sensitivity of neurons o Corresponds to pharmacokinetics of given drug o Small compared to other drugs - Requires great dose than required for hypnosis - Cross-tolerance: to all of each other - Psychological dependence (now called addiction) Drug Mechanism of action Side effects Pharmacokinetics BARBITURATES - ↑postsynaptic GABAA Receptors (inhibitory) Metabolism + excretion - pKa 7-8, so charged & uncharged in body In general o All types (unlike benzodiazepines) - Hepatic biotransformation - Good fat:water partition coefficient o Directly open the Cl- channel (not benzos) - Filtered, but nearly all is reabsorbed - Potency decreased if polar group is added to a - ↓ response to excitatory NTs, glutamate - Raising urine pH helps concentrate drug side chain hepatic biotransform. - No structural requirements, probably not a (since it is a weak acid) - No structural requirements, probably not a “lock “lock & key” mechanism of action & key” mechanism of action Sleep - ↑ porpharyn synthesis - Dose-response curves for all non-selective CNS ↓ time to onset of sleep Contraindicated w/porphyria depressants are parallel Prototype: barbital Subjective feeling of having slept well but NOT for benzodiazepines Thiopental - Can’t keep giving dose b/c it will build up - Very large fat: water partition coefficient and cease to depend on re-distribution - Hepatic biotransformation is slow and will start to depend on metabolism - RE-DISTRIBUTION determines duration Pentobarbital - Hepatic biotransformation determines duration Secobarbital Barbital Phenobarbital Long Med Short Non-selective CNS depressants In general Benzene ring confers some selectivity as anticonvulsant - Poor substrate for hepatic enzymes, 1/3 to ¼ is excreted unchanged in urine - Long t½: 2-5 days Others Drug Propofol Mechanism of action - ↑postsynaptic GABAA Receptors - Greater decrease in BP and ↓ contractility Side effects Pharmacokinetics - Lipid emulsion, (Fospropofol is H2O-soluble) - Rapid onset (like thiopental) - Brief duration of action, from distribution/metab - Rapid onset (like thiopental) - Brief duration of action, from distribution/metab - Etomidate - ↑postsynaptic GABAA Receptors Ketamine - NOT a non-selective CNS depressant - Used to produce “dissociative anesthesia” o Alalgesia, upresponsiveness, amnesia o Eyes often remain open o Involuntary limb movement o ↑ Sympathetic activity - Chloral hydrate (trichloroethanol active metabolite), ethchlorvynol, ethyprylon, meprobamate, methaqualone (no longer available) Usually used w/other drugs Non-barbiturate sedative hypnotics