Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
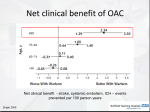
Risk assessment for bleeding complications The assessment of the overall risk of bleeding will depend on the INR, (where we know the relative risk increases significantly and exponentially from an INR of 4), and patient risk factors outlined below. Risk is a spectrum and your clinical decisions should be guided by all patient factors and INR. Risk factors can be additive. Patients with two or three risk factors have a much higher incidence of warfarin-associated bleeding than those with none or one. The reversal guidelines use low and high risk as criteria when considering patient factors, low would be where there are no risk factors listed below and high one or more. Risk Factor Category Specific Risk Factors Age > 65 years Cardiac Uncontrolled hypertension (SBP >160mmHg) Gastrointestinal Neurological History of gastrointestinal haemorrhage, active peptic ulcer disease, hepatic insufficiency, high alcohol ingestion ( 8 drinks/week). Liver disease (cirrhosis, bilirubin >2x normal, AST/ALT/AP >3x normal) Thrombocytopenia (platelet count < 50 x109 / L), platelet dysfunction, coagulation defect, underlying malignancy. Prior history of sever haemorrhage. Predisposition to bleeding (antiplatelets, NSAIDs, COX-1 inhibitors) History of stroke, cognitive or psychological impairment Renal Renal insufficiency, dialysis, transplant, creatinine >200 mol/L Trauma Recent trauma or major surgery in previous 2 weeks, history of falls (> 3 within previous treatment year, recurrent or injurious falls) Aspirin, antiplatelets, COX-1 inhibitors. Amiodarone, antibiotics, anticonvulsants and some complementary medicines may have caused the raised INR and may make correction and control difficult Unstable or high INRs. Time in the therapeutic range < 60% Haematological / Oncological Medications Labile INR Link to the HAS BLED Calculator Developed by the ECI from “Warfarin reversal: consensus guidelines on behalf of the Australasian Society of Thrombosis and Haemostasis” Ross I Baker, Paul B Coughlin, Alex S Gallus, Paul L Harper, Hatem H Salem and Erica M Wood,2004, Medical Journal of Australia, 181(9), 492-497 Updated June 2016