Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
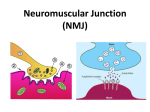
MUSCLE RELAXANTS Muscle relaxants are drugs that interrupt transmission of neural impulses at the neuromuscular junction History Involved research using Banded Krait (bungarotoxins) and cobra as well as curare from South American plants Banded Krait from Taiwan Most potent source of curare Clinical uses 1. Provide skeletal muscle relaxation to facilitate intubation of the trachea 2. Provide optimal surgical working conditions 3. In the intensive care setting to facilitate mechanical ventilation of the lungs Note MR lack anesthetic or analgesic effects and must not be used to render an inadequately anesthetized patient immobile The choice of MR is influenced by: 1. Its speed of onset 2. Duration of action 3. Rout of elimination 4. Associated side effects Neuromuscular junction Consist of a prejuctional motor nerve ending separated from the highly folded postjunctional membrane by synaptic cleft Neuromuscular transmission is initiated by arrival of an impulse at the motor nerve terminal with an associated influx of calcium and a resultant release of neurotransmitter acetylcholine Ach binds to nicotinic cholinergic receptors on postjunctional membrane, causing a change in membrane permeability to ions, principally K & Na ions Ach is rapidly hydrolyzed by enz. Acetylcholine esterase (true cholinesterase) Nicotinic cholinergic receptors 1.Prejunctional 2.Postjunctional 3.extrajunctional Neuromuscular Junction 50% recaptured by nerve terminal ACh ACh Ca2+ Ca2+ Voltage-dependent Ca2+ channels Ca2+ Acetate and choline ACh ACh (8-10,000 molecules) ~100mM nAChR Muscle fibre Muscle relaxants Depolarizing noncompetitive Nondepolarizing competitive Depolarizing (succinylcholine or Suxamethonium) Clinical use: - - - - - - Averse effects 1. 2. 3. 4. 5. 6. 7. 8. 9. Cardiac dysrthymia: Bradycardia, arrest Myalgia Myoglobinuria Increased Intraocular pressure Increased Intragastric pressure Increased Intracranial pressure Trismus Allergic reactions Trigger for malignant hyperthermia 10. Hyperkalemia • Denervation injury (spinal cord transection) • Unhealed skeletal muscle injury as produced by 3rd degree burn • Upper motor neuron injury • Multiple trauma Causes of delayed recovery from succinylcholine 1. 2. 3. 4. Sever liver disease Potent anticholine esterase (insecticides) Chemotherapy (cyclophosphamide) A typical pseudo cholinesterase Nondepolarizing competitive Nondepolarizing competitive Long acting (>30 min) Pancuronium D-tubocurarine Gallamine Intermediate acting (15-25 min) Vecuronium Cis (atracurium) rocuronuim Short acting (<15 min) Mivacurium Factors enhance effects of NDMR 1. 2. 3. 4. 5. 6. 7. 8. 9. Volatile anesthetics Aminoglycosides Antibiotics Mg Local analgesics Calcium channel blockers (verapamil) Cardiac antiarrythmias (quinidine) Hypothermia Acidosis Hypokalemia Drug-assisted antagonism of Nondepolarizing muscle relaxants Anti-choline esterase Neostigmine edrophonium pyridostigmine Anticholinesterase Drug accelerates the already established pattern of spontaneous recovery at the neuromuscular junction by inhibiting the activity of acetylcholinesterase leading to accumulation of ach. At nicotinic (neuromuscular junction) and muscarinic sites The competition between ach and a Nondepolarizing MR in favor of the neurotransmitter (Ach) and restores neuromuscular transmission • Anticholinesterase does not cross blood brain barrier • Peripheral muscarinic effects block by anticholinergic drugs like Atropine Thank you