Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
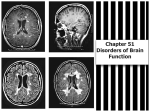
Increased Intracranial Pressure Mary Ann Reilly BSN, MS, CRRN Santa Clara Valley Medical Center, Rehab Nurse Manager • In 2004 the SJ Mercury wrote: "As he was giving his speech he stumbled slightly and then he started to perspire a bit. I thought almost immediately that something is not right.“ • His repeated vomiting prompted paramedics to treat him with oxygen and monitor his heart for half an hour -- routine care for a sudden foodborne illness • The initial suspicion that Mayor Ron Gonzales had food poisoning Wednesday night shows just how difficult some strokes are to detect -- and experts say it offers a warning to people who might find themselves with similar symptoms. • Gonzales' type of stroke is called an intraventricular hemorrhage. • This means that a blood vessel had broken and was leaking into the ventricle, which carries spinal fluid. So what’s the big deal? • Skull • Components of Cranial Vault – Meninges • Dura • Arachnoid • Pia – Brain • Brain tissue 80-88% – Blood • Blood 2-11% – CSF • CSF 9-10% http://learntech.uwe.ac.uk/neuroanatomy/neuro4_1.htm Blood – 15-20 of the cardiac output – 20-25% of all oxygen inspired – 750cc/min • 80% from carotid arteries • 20% from vertebral • Circle of Willis is collateral circulation – No sugar/fat/oxygen storage Autoregulation •When intra-cranial pressure begins to rise, the body’s own compensatory mechanisms include decreasing the production of CSF and restricting the blood flow to the brain(by vasoconstriction). Autoregulation • Self Regulated – PCO2 (carbon dioxide) vasodilator • For every 1mmHg change in PCO2 there is a 1-2cc change in blood flow per 100 GMs of brain – (1300-1400Gms avg. wt.) =s [750 +65] or [750 + 130] • Diameter of vessels – Hypercapnia: Increases CBF – Hypocapnia: Decreases CBF Intercrainial Pressure Regulation • When BP increases, cerebral arterioles constrict to keep blood entering brain at steady rate. • When BP falls, cerebral arterioles dilate to increase blood flow to brain Intercrainial Pressure Regulation • Metabolic regulation—changes in O2 and CO2: Low O2 and increased CO2 cause vasodilation CSF regulation—decreased production or increased reabsorption decreases ICP. Factors Affecting CBF • • • • Viscosity of the blood Seizures Anemia Drugs CSF • 125-150 cc clear fluid – 500cc produced per day – 20cc per hour – Replaced 4-7 times per day • Function – Protection, cushions – Waster disposal – Nutritional support (2/3 bodies BS) CSF Pressure • Norm – 1-15 mmHg or <200mm H2O • Low pressure – Dehydration • Increased pressure – Val Salva,Tumor, Subdural Hematoma, Subarachnoid Hemorrhage, Infections, Hydrocephalus Symptoms of Increasing ICP • • • • • • • Headache Visual changes Nausea Vomiting Behavior changes Changes in LOC Seizures Symptoms • Aniscoria • Hemiparesis • Vital sign changes – Cushing Triad Pulse Cardiac center is located in the medulla – compression may affect heart rate Temperature Raised indicates infection Hypothermia seen in drug overdose Blood Pressure Increase associated with sympathetic stimulation. Decrease rarely attributed to brain injury Respiration Increase may indicate damage to the midbrain. Decrease may indicate damage to lower pons and upper medulla Pupils One reacting the other not may indicate pressure on the to the 3rd cranial nerve caused by I-ICP or a lesion http://learntech.uwe.ac.uk/neuroanatomy/neuro4_4.htm Cushing’s Triad • Vital Sign Changes in ICP— • Systolic pressure increases (widened pulse pressure results). • Slowing of heart occurs—bradycardia (occurs as result of reflexive slowing in response to increased systolic pressure) • Respiration changes—becomes slowed Could it be? – – – – – – Difficulty speaking Blurred vision Hypertension Shallow rapid breathing Visual disturbances Paresthesia • Hypoglycemia OR? - Confusion – – – – Lethargy Nausea & Vomiting Coma Seizures • Syndrome of Inappropriate ADH OR? – – – – – – Changes in LOC Nausea & Vomiting Irritability Disorientation Personality changes Seizures • Fluid Overload OR? – – – – – Street drug Alcohol withdrawal Over dose Diabetic ketoacidosis Hypervitiaminosis A • Drug • www.merck.com/mrkshared/mmanual/section1/chapter3/3c.jsp Diagnosis of Increased Intracranial Pressure • • • • Overt symptoms Papilledema Nuchal rigidity Lumbar Puncture*** Lumbar Puncture • Contraindicated – – – – – Focal signs Intracranial mass Papilledema Cardiorespiratory compromise Infection of skin Rational for Contraindication • A simple analogy Performing a LP in the presence of I-ICP, may result in herniation Herniation • Tentorium – Midbrain and diencephalon through the tentorium • Uncal • Tonsillar – Cerebellar tonsils through the foramen magnum Diencephalic Stage • Confused and drowsy • Constricted pupils • Gaze palsies Mesencephalic Stage: • Unconscious • Decerebrate posturing • Dilated pupils • Hyperventilation Pontine Stage • Unconscious • Decerebrate posturing • Constricted pupils • Irregular breathing Decorticate posture • Indicated by rigidity, flexion of the arms, clenched fists, and extended legs. The arms are bent inward toward the body with the wrists and fingers bent and held on the chest. Presence of this type of posturing implies severe damage to the brain with immediate need for medical attention. Decerebrate Posturing • Internal rotation and extension of the arms & lower limb extension • Due to midbrain compression as the brainstem is further compressed Medullary Stage • Unconscious • Flaccid • Loss of homeostatic control: • Increase heart rate • Decrease blood pressure • Hyperthermia • Cheyne-Stokes breathing Cheyne-Stokes • Breathing describes a waxing and waning ventilation, sometimes with periods of apnea, that occur in cycles. • It is due to a delay in the medullary chemoreceptor response to blood gas changes 89 3 http://thediagram.com/3_6/ Common Causes of I-ICP • Vascular abnormalities – AV malformations, aneurisms, stroke • Diffuse cerebral ischemia – Closed head trauma, shaken baby, vasospasm • • • • CNS infections Tumors Trauma Obstruction of CSF flow Hydrochepalus Intra Cerebral Hemorrhage AV Malformation Crainal Defect Crainial defect with midline shift • The Monroe-Kelle Hypothesis states that an increase in the volume of one component (blood, brain tissue, CSF) must be accompanied by a decrease in another component if intracranial pressure is to remain constant. The CSF and blood volume are the compartments that most easily change to accommodate changes in pressure. Interventions to prevent secondary brain injury follows these principles and focuses primarily on cerebral blood flow and drainage. Management / Trauma • • • • • Rapid transportation Early intubation Aggressive resuscitation Immediate CT ICP monitoring CAT Scans • Sensitivity for visualizing blood approximately 96% • Visualizes – Fractures – Hematomas Operative Management • Burr holes • Intra-operative ultra sound • Surgical evacuation of mass lesion – Craniotomy – Craniectomy • Ventricular drainage http://www.trauma.org/neuro/neuromonitor.html Medical Management • Adequate cerebral perfusion – Dehydration – Hypovolemia – Hypoxia • Hyperventilation – Sepsis – Normal or hypothermia • Hyperthermia causes increased cellular metabolism (10-13%), increased lactic acid production, increased CO2 (vasodilatation) Osmotic Diuretics Mannitol • • • • Reduces ICP in 5-10 min. trough osmotic gradient BBB must be intact Removes H2O not Na Caution with – Hypotension – Coagulopathy – CHF Duiretics • Furosemide (lasix) – Loop of Henle, blocks transport of Cl & Na – Reduced CSF production 40-70% – Postssium depletion Other Medications • Corticosteroids • H2 Blockers • Sedation to control agitation, reduces metabolic needs • Analgesia • Barbiturates to suppress seizures, decreases metabolic needs, vasoactive effects Hypothermia • • • • • Decreased cellular metabolism Brain temp is ~ 2.0o F higher than body Reduces inflammatory process Reduces cerebral metabolism Limits secondary brain injury Nutrition • Energy requirement 125-200% ABOVE normal • Early feeding has a favorable effect on survival • TPN & PPN Nursing Care • • • • • • Assessment Touch Oxygen Control pain Medicate prior to administering care Break up activities Care • • • • Decrease stimulation Positioning Bowel Bladder Glascow Coma Scale Verbal Eye opening Motor Score Score Score Finding 5 4 3 2 1 Finding Normal fluent appropriate Confused but fluent Mumbling occasional word recognizable Vocalizations but no words No vocalizations or verbalizations Finding 6 5 4 3 Eyes open without stimulation Eyes open to loud noise 4 3 2 Eyes open to pain only 2 1 No eye opening 1 Follows commands Locates pain stimulus Pulls away from pain Flexion posture to pain Extension posture to pain No motor response 1. 2. 3. 4. 5. 6. 7. 8. www.rad.usuhs.mil/rad/herniation www.thridage.com/health/adam/ency/article www.homestead.com/emguidemaps/files/coma.html www.classes.kuma.edu/sm/nurs420 www.emguidemaps.homestead.com/files/anisocoria.html www.annals.org/cgi/content/full/130 /5/427/F1 www.med.harvard.edu/AANLIB/home.html http://thediagram.com/3_6/ http://www.sophysa.com/patient/hydrocephalus/hydrocephalus3.htm Lumbo-Peritoneal Shunt LEONARDO DA VINCI - Drawing of the cerebral ventricles after they have been injected with a dye Speech arrest Fluent Aphasia This large cerebral infarct occurred in the setting of atrial fibrillation and caused a dense fluent aphasia. The CT scan shown here was obtained 5 days after the onset of stroke symptoms. View the temporal movie of this slice to see the evolution of the lesion over the 5 day period. Significant swelling in the infarcted area produces obvious shift of the midline by day 5. This corresponded clinically to a diminished level of arousal, which resolved after 2 days. Can’t read Hesitating Speech Loss of sensation Chronic Subdural Cavenous angioma AV Malformation with MRA Acute Stroke sudden onset of right body weakness and trouble speaking Diffusion-weighted MR showed a large area of abnormal signal in the region clinically suspected: the portion of left hemisphere supplied by the middle cerebral artery. Normal aging brain Normal aging Normal Aging coronal plane http://www.med.harvard.edu/AANLIB/home.html Cerebral Hemorrhage MS Look at the large round white spot in the right frontal region. This is a relatively new lesion, and you can see how it enlarges very rapidly over the next weeks. Look at the timeline cine. With time, the lesion enlarges, there is a "halo" of white (high) signal which surrounds the lesion. This probably represents the edema which forms in reaction to the acute damage. At the end of the movie, you can see that the lesion has nearly disappeared, with another lesions appearing http://www.neuroland.com/default_old.htm http://www.neuroland.com/nm/neuropathic_pain.htm Burst arteries cause Increased ICP by • Increased Intracrainal PressureNormal intracrainal pressure—less than 15mm Hg or 180mm H20. ^ICP considered when pressure ^than this. When ICP^ ischemia and hypoxia results and damages neural tissue. If ICP^ continues—can cause herniation syndrome. • Causes of ICPBrain tumors, abscesses, cerebral edema from injuries. CSF obstruction—produces hydrocephalus Communicating vs. non-communicating Cerebral vasodilation—compensatory mechanism for conditions of hypoxia (when pCO2 ^, cerebral vasodilation will occur). • Head InjuriesSkull fractures—linear, comminuted, depressed or basilar Basilar (occurs at base of skull)—produces hemorrhage from nose, pharynx, ears Bruising over mastoid bone—Battle’s sign May cause CSF leaking from ears, nose Brain Injuries--Concussion vs. Contusion Intracranial Hemorrhage—Epidural vs. Subdural Hematoma • Epidural HematomaBlood collects in the epidural space Expanding hematoma causes rapid symptoms of I.C.P. and is considered medical emergency Treatment—surgical openings through skull (burr holes) to decrease I.C.P., craniotomy may be necessary to remove clot and control bleeding • Subdural HematomaCollection of blood between dura and the brain May be venous in origin, may be acute, subacute, or chronic depending on size of vessel and amount of bleeding Acute—cause is major head injury, symptoms develop over 24-48 hrs. Subacute—less severe trauma, symptoms develop over 48 hrs. to 2 weeks Chronic—cause is minor trauma, seen in elderly, symptoms develop over 3 weeks to 3 months • Treatment of ICPHyperventilation—blow off CO2. Osmotic diuretics--^serum osmolarity Mannitol (Osmitrol) Hypertonic Glucose Loop diuretics Steroids—IV or p.o. Dexamethosone (Decadron) Methylprednisolone (Solu-Medrol) • Treatment of ICP cont.Anticonvulsants— prevent seizures IV fluids—keep moderately dehydrated GIVE 0.45% to 0.9% NaCl AVOID 5% Dextrose Barbiturates may be used in extreme cases in order to induce coma and decrease metabolic demands on brain. • Brain tumors Classified by site, histologic cell type, degree of malignancy Gliomas—arise from neuroglia tissue Medulloblastoma—malignant tumor of cerebellum Menigiomas—arise from meniges, slow growing Acoustic neuromas—arise from 8th cranial nerve Pituitary—arise from pituitary gland, slow growing Location of tumors (in cerebral lobes) account for specific symptoms • Symptoms of Brain Tumors Classic symptoms of I.C.P. Headache may be worse in A.M. Seizures are common with all types of brain tumors Other symptoms depends on location of tumor within the cerebral lobes (occipital, frontal, parietal, temporal, cerebellar) • Treatment of brain tumorsTumor reduction—surgery, radiation, chemotherapy Manage and prevent symptoms of I.C.P. Crainotomy Supratentorial approach—above the tentorium (fold of dura separating cerebral cortex from cerebellum and brainstem Infratentorial approach---below the tentorium • Pre-op Nursing CareShaving head—permit needed, save hair, provide cap Teach deep breathing and leg exercises (no coughing) Pre-op enema is controversial Excellent baseline assessments necessary pre-op • Post-op Nursing Care—Supratentorial ApproachH.O.B. 30-45 degrees Pillow under head and shoulder, align neck Avoid positioning on operative side Monitor for cranial nerve dysfunction II-visual deficits III-ptosis IV, V—deficits in extraocular movements • Post-op Nursing Care for Infratentorial ApproachH.O.B. flat, keep client off back Small pillow under head, neck alignment Monitor for cranial nerve dysfunction III, IV, VI—ocular movements VII—absent corneal reflex, paralysis of facial muscles VIII—decreased hearing, nystagmus IX, X—gag and swallowing reflex decreased • Nursing Care Common to both surgical approachesContinuous neuro assessments, especially for I.C.P. Anticonvulsants, seizure precautions Body temperature regulation, prevent hyperthermia Turn, deep breath q. 2 hrs. Reinforce dressings—check for CSF on drainage Pain management— use of Codeine • S.I.A.D.H. Posterior pituitary secretes ADH to regulate water balance Too much ADH causes S.I.A.D.H. where kidneys will retain H2O and blood serum will be hypotonic Signs and symptoms: Changes in L.O.C., headache, nausea and vomiting Decreased urinary output • Treatment of S.I.A.D.H.Fluid restriction 500cc or less in 24 hrs. IV fluids 3% or 5% saline with appropriate electrolyte replacements (K, Mg) Diuretics (Lasix) Lithium Carbonate • Diabetes InsipidusFailure of ADH secretion and failure of kidneys to store H2O. Signs and symptoms: Urinary output increased with specific gravity of urine decreased Client will have dehydration Treatment: Use of Vasopressin (Pitressin), given I.M. or s.c. http://academic.luzerne.edu/aisaacs/webversion/nur204-2003/03increasedintracrainalpressure_files/frame.htm