Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
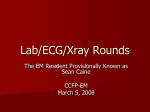
Clinical Profile and Significance of Delayed Enhancement in Hypertrophic Cardiomyopathy Martin S. Maron, MD; Evan Appelbaum, MD; Caitlin J. Harrigan, BA; Jacki Buros, BA; C. Michael Gibson, MD, MS; Connie Hanna, RN; John R. Lesser, MD; James E. Udelson, MD; Warren J. Manning, MD; Barry J. Maron, MD Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 Background—Contrast-enhanced cardiovascular magnetic resonance with delayed enhancement (DE) can provide in vivo assessment of myocardial fibrosis. However, the clinical significance of DE in hypertrophic cardiomyopathy (HCM) remains unresolved. Methods and Results—Cine and cardiovascular magnetic resonance with DE were performed in 202 HCM patients (mean age, 42⫾17 years; 71% male), DE was compared with clinical and demographic variables, and patients were followed up for 681⫾249 days for adverse disease events. DE was identified in 111 (55%) HCM patients, occupying 9%⫾11% of left ventricular myocardial volume, including ⬎25% DE in 10% of patients. The presence of DE was related to occurrence of heart failure symptoms (P⫽0.05) and left ventricular systolic dysfunction (P⫽0.001). DE was present in all patients with ejection fraction ⱕ50% but also in 53% (102/192) of patients with preserved ejection fraction (P⬍0.001); %DE was both inversely related to (r⫽⫺0.3; P⬍0.001) and an independent predictor of ejection fraction (r⫽⫺0.4; P⬍0.001). DE (7%⫾7% of left ventricle) was present in 54 patients who were asymptomatic (and with normal ejection fraction). Over the follow-up period, the annualized adverse cardiovascular event rate in patients with DE exceeded that in patients without DE but did not achieve statistical significance (5.5% versus 3.3%; P⫽0.5). Conclusions—In a large HCM cohort, DE was an independent predictor of systolic dysfunction but with only a modest relationship to heart failure symptoms. These data suggest an important role for myocardial fibrosis in the clinical course of HCM patients but are not sufficient at this time to consider DE as an independent risk factor for adverse prognosis. (Circ Heart Fail. 2008;1:184-191.) Key Words: heart failure 䡲 MRI 䡲 fibrosis 䡲 hypertrophic cardiomyopathy H ypertrophic cardiomyopathy (HCM) is the most common genetic heart disease and the leading cause of sudden cardiac death in the young and is also associated with heart failure, disability, and death at any age.1– 8 In HCM, left ventricular (LV) myocardial fibrosis provides a structural substrate, which has been implicated in promoting heart failure as well as risk for arrhythmic sudden death.9 –15 Contrast-enhanced cardiovascular magnetic resonance (CMR) with delayed enhancement (DE) imaging can reliably detect myocardial fibrosis in vivo and has been reported to be an important determinant of outcome in ischemic heart disease and nonischemic dilated cardiomyopathy.16 –28 However, the clinical significance of DE in HCM remains unresolved.25,26,29 Therefore, we sought to investigate DE in a large HCM cohort by characterizing its prevalence, morphological profile, and relation to clinical and demographic features and prognosis. Clinical Perspective see p 191 Methods Selection of Patients We prospectively evaluated 202 HCM patients presenting to centers at Tufts Medical Center (Boston, Mass) and the Minneapolis Heart Institute Foundation (Minneapolis, Minn) between April 2002 and November 2006. The initial clinical evaluation was defined as the time of the CMR examination at each institution. The duration of follow-up from CMR to the most recent evaluation (October 1, 2007) or death was 681⫾249 days; no patient was lost to follow-up. LV outflow tract obstruction was defined as a peak instantaneous outflow gradient ⱖ30 mm Hg, assessed by continuous-wave Doppler echocardiography under resting conditions.8 No study patient underwent an alcohol septal ablation or surgical septal myectomy procedure. We excluded significant atherosclerotic coronary artery disease (⬎50% stenosis in 1 major artery) as a cause of pre-existent Received January 22, 2008; accepted May 23, 2008. From the Hypertrophic Cardiomyopathy Center, Division of Cardiology, Tufts Medical Center, Boston, Mass (M.S.M., J.E.U.); Department of Medicine, Cardiovascular Division, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Mass (E.A., C.M.G., W.J.M.); PERFUSE Angiographic Core Laboratory and Data Coordinating Center, Harvard Medical School, Boston, Mass (E.A., C.J.H., J.B., C.M.G., W.J.M.); and the Hypertrophic Cardiomyopathy Center, Minneapolis Heart Institute Foundation, Minneapolis, Minn (C.H., J.R.L., B.J.M.). Guest editor for this article was Eric R. Bates, MD. Correspondence to Martin S. Maron, MD, Tufts Medical Center, #70, 800 Washington Street, Boston, Massachusetts 02111. E-mail [email protected] © 2008 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org 184 DOI: 10.1161/CIRCHEARTFAILURE.108.768119 Maron et al myocardial scars in study patients with DE by virtue of 2 specific clinical or CMR criteria: (1) no study patient experienced an acute coronary event associated with increased cardiac enzymes or Q waves on ECG and (2) in all patients with DE distributed in a single coronary vascular territory, hemodynamically significant coronary artery disease was excluded by arteriography or computed tomography angiogram. In addition, among the 6 patients with transmural or subendocardial DE distributed across multiple coronary artery vascular territories, 4 were ⬍40 years of age with no coronary artery disease risk factors, whereas 2 were ⬎40 years of age and, because of an LV ejection fraction ⬍50% (ie, end stage), underwent coronary arteriography, which demonstrated in both the absence of significant coronary artery disease. All study patients signed a statement previously approved by the internal review boards of the respective participating institutions, agreeing to the use of their medical information for research purposes. The authors had full access to and take full responsibility for the integrity of the data. All authors have read and agreed to the manuscript as written. Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 Definitions Diagnosis of HCM was based on 2D echocardiographic and CMR documentation of a hypertrophied and nondilated LV in the absence of another cardiac or systemic disease capable of producing a similar magnitude of hypertrophy at some point in the clinical course of each patient.1,2,6,30 Sudden death was defined as sudden and unexpected collapse in patients who previously had a relatively uneventful clinical course. Progression of heart failure was defined as an advancement of at ⱖ1 New York Heart Association (NYHA) functional class during the follow-up period. In addition, potentially lethal events in which patients received appropriate implanted defibrillator interventions (shocks or antitachycardia pacing triggered by ventricular tachycardia/fibrillation) were regarded as equivalent to sudden death. CMR CMR imaging was performed (Gyroscan ACS-NT 1.5T, Philips, Best, the Netherlands, and Sonata 1.5T, Siemens, Erlangen, Germany) using steady-state, free-precession breath-hold cines in 3 long-axis planes and sequential 10 mm short-axis slices (no gap) from the atrioventricular ring to apex. DE images were acquired 15 minutes after the intravenous administration of 0.2 mmol/kg of gadolinium-DTPA (Magnevist, Schering; Berlin, Germany) with a breath-hold 2D segmented inversion-recovery sequence acquired in the same views as the cine images. The inversion time ranged from 240 to 300 ms and was chosen to null normal myocardial signal. LV volume, mass, and ejection fraction were measured using standard volumetric techniques and analyzed with commercially available software (MASS version 6.1.6, Medis, Inc, the Netherlands).31 Volume and mass measurements were indexed to body surface area. Maximal LV wall thickness was defined as the greatest dimension at any site within the LV wall. The LV was assessed according to the American Heart Association 17-segment model.32 To ascertain the presence of DE, all tomographic short-axis LV slices from base to apex were inspected visually to identify an area of completely nulled myocardium. The mean signal intensity (and SD) of normal myocardium was calculated, and a threshold ⱖ6 SDs exceeding the mean was used to define areas of DE.18,27,33,34 Areas of artifact (ie, blood pool, incomplete nulling of fat and pericardial fluid) were excluded from the analysis by manually adjusting the individual contours. Total volume of DE (expressed in grams) was calculated by summing the planimetered areas of DE in all short-axis slices and was expressed as a proportion of total LV myocardium (%DE). DE analysis was performed by 1 experienced reader (C.J.H.; 2 years of CMR experience, including the assessment of ⬎800 CMR studies, of which 600 involved the quantification of DE). These readings were reviewed and confirmed by a second expert reader (E.A.; ⬎7 years of CMR experience). Both these independent observers were blinded to patient identity and clinical profile. Any Delayed Enhancement in HCM 185 discrepancies between the 2 readers were adjudicated by a senior observer (W.J.M). To assess interobserver variability for the presence of DE, a second reader (E.A.) independently reanalyzed all CMR studies. Among the studies in which there was agreement between the 2 readers on the presence of DE, reader E.A. reanalyzed 20 randomly selected studies to determine the interobserver variability for extent of DE. To assess intraobserver variability, reader C.J.H. reanalyzed all 202 CMR studies 4 to 6 months after the initial interpretation, blinded to the previous results. Statistical Analysis Continuous data are expressed as mean⫾SD. Clinical and demographic characteristics of the 2 patient groups (DE and non-DE) were compared with the Wilcoxon rank-sum test for continuous variables and 2 or Fisher exact tests for categorical variables. Clinical features of the study patients were compared with the extent of DE with the Wilcoxon rank-sum test or Kruskal-Wallis equality-ofpopulations rank test for categorical variables and Spearman’s rank correlation coefficient () for continuous variables. The primary clinical end point used in this study was a composite of the following adverse cardiovascular events: sudden death, appropriate implantable cardioverter difibrillator (ICD) discharge, and progressive heart failure symptoms of ⱖ1 NYHA class. Patient-level characteristics were modeled as linear regressions in unadjusted and adjusted analyses. Per-segment data clustered within a patient were assessed by linear mixed-effects models with a random intercept per patient. Probability values of ⬍0.05 were considered significant. Calculations were performed with Stata SE version 9.2 (StataCorp, College Station, Tex). Kaplan-Meier event rates were calculated to accommodate for differential length of follow-up between patients. The comparison of event rates among patients with and without DE was performed using a log-rank test for equality of survivor functions. Among patients with DE, the relationship between %DE and the likelihood of subsequent cardiovascular events was evaluated using a univariate Cox model. Results Patient Characteristics Baseline clinical and demographic characteristics of the 202 study patients at initial evaluation are summarized in Table 1. Mean age was 42⫾17 years; 144 (71%) were male. NYHA class was 1.5⫾0.7 and maximal LV wall thickness was 22⫾5 mm (range, 14 to 37 mm). Morphological Features of DE Prevalence and Extent DE was present in 111 (55%) of the HCM patients, and %DE was 9%⫾11% (range, 0.2% to 51%), which was equivalent to 19⫾21 g (range, 0.4 to 85 g) and included 11 patients (10%) with %DE ⱖ25% (Table 1). Location and Distribution DE was most commonly located in both the ventricular septum and LV free wall (n⫽35; 32%) but was also confined to the LV free wall (n⫽29; 26%), the septum (n⫽27; 24%), the area of right ventricular insertion into the ventricular septum (n⫽15; 13%), and the LV apex (n⫽5; 5%). DE was transmural (occupying ⱖ75% of LV wall thickness) in 58 patients (52%) in the following segmental distribution: septum (n⫽10), LV free wall (n⫽21), septum and LV free wall (n⫽25), and apex (n⫽2). In the remaining 53 patients (48%), DE was nontransmural in the following distribution: midmyocardial (n⫽17), right ventricular insertion areas (n⫽12), subendocardial (n⫽9), subepicardial 186 Circ Heart Fail Table 1. September 2008 Demographic and Clinical Characteristics of 202 HCM Patients with CMR Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 No. (%) of patients Age, y Male, n (%) Body surface area (g/m2) NYHA class, n (%) I II III/IV Mean EF, n (%) ⱖ60% 51%[en]59% ⱕ50% Basal LVOT gradient ⱖ30 mm Hg, n (%) Maximum LV thickness, mm LV mass, g LV mass index, g/m2 LA dimension, mm LVED dimension, mm DE (range), g % LV with DE (range) All Patients DE (⫹) DE (⫺) 202 (100) 42⫾17 144 (71) 1.97⫾0.3 111 (55) 43⫾17 78 (70) 1.96⫾0.3 91 (45) 40⫾18 66 (73) 1.99⫾0.3 123 (61) 54 (27) 25 (12) 1.5⫾0.7 61 (55) 31 (28) 19 (17) 1.6⫾0.8 62 (68) 23 (26) 6 (7) 1.4⫾0.6 182 (90) 10 (5) 10 (5) 48 (24) 22⫾5 211⫾80 107⫾34 67⫾11 52⫾7 N/A N/A 92 (83) 9 (8) 10 (9) 26 (23) 23⫾5 219⫾85 113⫾37 69⫾10 53⫾7 19⫾21 (0.4 to 85) 9⫾11 (0.2 to 51) 90 (99) 1 (1) 0 (0) 22 (24) 20⫾4 201⫾72 100⫾28 65⫾11 51⫾6 N/A N/A P value* – 0.3 0.7 0.6 0.05 0.03 0.001 0.9 ⬍0.001 0.114 0.02 0.027 0.097 – – LVOT indicates left ventricular outflow tract; LVED, left ventricular end-diastolic; N/A, not applicable. *Based on comparison between DE (⫹) and DE (⫺) patients. (n⫽8), and ⱖ2 of these nontransmural distributions (n⫽7) (Figure 1). Relation of DE to Heart Failure Symptoms A relationship was identified between presence of DE and heart failure symptoms. DE was most common in patients with severe (NYHA class III–IV; 19/25 [76%]) and moderate symptoms (NYHA class II; 31/54 [57%]) and was also present in 61 of 123 (50%) asymptomatic patients (P⫽0.05; Table 1 and Figure 2). %DE was 8.9%⫾9.6% in asymptomatic patients and 9.9⫾13.4% in those with heart failure symptoms (NYHA classes II–IV) (P⫽0.2; Figure 3). A B Patients with areas of transmural DE were no more likely to have heart failure symptoms than were patients with nontransmural DE (P⫽0.7). DE specifically confined to the area of right ventricular insertion into the ventricular septum was unrelated to heart failure symptoms (P⫽0.5). %DE in these areas was relatively small and less than in other patients with DE (3.0%⫾2.2% versus 10.2⫾12%; P⫽0.008). Relation of DE to Ejection Fraction DE was present in all 10 patients with ejection fraction (EF) ⱕ50% (ie, end-stage phase; each transmural), in 9 of 10 (90%) with EF 51% to 59%, and in 92 of 182 (51%) with EF C VS D E F LV VVS V S S RV Figure 1. LV short-axis delayedenhanced CMR images from 6 HCM patients showing diverse patterns of DE. A, Extensive transmural area in the anterior ventricular septum (VS) extending into the contiguous anterior free wall (arrow). A small focal area of DE is also present in the region of the right ventricular insertion into the posterior septum (double arrow). B, Multifocal midmyocardial distribution within the septum (arrows). C, Predominate transmural DE in the inferolateral LV free wall (arrows). D, DE on the right ventricular side of septum (arrows) and subepicardial area in the contiguous anterior free wall (double arrow). E, Subendocardial distribution within septum and anterior wall (arrows). F, Focal area (arrow) of DE at right ventricular insertion with posterior septum. % of Patients with DE Maron et al 187 LV Outflow Obstruction Patients with DE were no more likely to have LV outflow obstruction at rest than were patients without DE (P⫽0.9). Among patients with obstruction, there was no significant relationship between %DE and magnitude of LV outflow gradient at rest (r⫽0.2; P⫽0.23). 80 p=0.05 70 Delayed Enhancement in HCM 60 50 40 30 20 10 0 I II III/IV NYHA Class at Study Entry Figure 2. Comparison of DE presence in HCM patients with NYHA classes I, II, and III/IV. Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 ⱖ60% (P⫽0.001) (Table 2). Also, %DE was more extensive in patients with EF ⱕ50% compared with those with EF 51% to 59% or ⱖ60% (27% versus 12% versus 7%, respectively; P⫽0.004) (Figure 4), and an inverse relationship was present between EF and %DE (r⫽⫺0.3; P⬍0.001). Multivariable Cox regression analysis (including LV outflow obstruction, maximal wall thickness, mass index, enddiastolic dimension, age, gender, left atrial size, and NYHA functional class) showed %DE as an independent predictor of EF (r⫽⫺0.4; 95% CI, ⫺0.6 to ⫺0.2; P⬍0.001). Of the 182 patients with EF ⱖ60%, 54 (30%) were both asymptomatic (NYHA class I) and had DE occupying 7%⫾7% (range, 1% to 34%) of LV myocardium (Table 2), including 26 with transmural DE. Twenty-three other patients (12%) with EF ⱖ60% experienced only mild symptoms (NYHA class II) had DE occupying 9%⫾12% of LV (range, 0.2% to 51%), including 9 with transmural DE. Relation of DE to Other Demographic and Clinical Variables Age and Gender Patients with DE were 43⫾17 years of age (range, 1 to 79 years), including 23 (21%) who were ⱕ30 years of age and 21 (19%) who were ⱖ60 years of age. Patients with and without DE did not differ significantly with respect to age (P⫽0.3); also, %DE was unassociated with age (r⫽0.05; P⫽0.8). Presence of DE did not differ with respect to gender (57% [female] versus 54% [male]; P⫽0.7) LV Wall Thickness and Mass Patients with DE had greater maximal LV wall thickness (23⫾5 mm) and LV mass index (113⫾37 g/m2) than patients without DE (20⫾4 mm and 100⫾28 g/m2; P⬍0.001 and P⫽0.02, respectively). A significant relationship was evident between DE and segmental LV wall thickness (P⫽0.002). DE was present in 15 of 112 (13%) LV segments ⱕ15 mm, 93 of 1216 (8%) LV segments 16 to 20 mm, 131 of 1216 (9%) LV segments 21 to 25 mm, 73 of 608 (12%) LV segments 26 to 30 mm, and 50 of 288 (17%) LV segments ⱖ30 mm. Reproducibility for the Presence and Extent of DE For presence of DE, the intraobserver and interobserver agreements were 96% and 93%, respectively. For the intraobserver and interobserver quantifications of DE extent, the mean differences in measurement were 1.4⫾9 g (11%) and 5.4⫾18 g (3.4%), respectively (⫽0.5 and ⫽0.2, respectively; both P⬍0.001). Relation of DE to Clinical Outcome Over the follow-up period, adverse cardiovascular events occurred in 11 patients, including 7 patients with DE (2 with sudden death, 2 with appropriate ICD discharge, and 3 with progressive heart failure symptoms) and 4 patients without DE (3 with sudden death and 1 with progressive heart failure). Annual cardiovascular event rate in HCM patients with DE exceeded that in patients without DE (5.5% versus 3.3%), although this comparison did not achieve statistical significance (P⫽0.5; hazard ratio, 1.45 [95% CI, 0.43 to 4.97]) (Figure 5). Extent of DE did not differ between patients with and without adverse cardiovascular events (9⫾11% versus 11⫾15%; P⫽0.97). Patients with transmural or nontransmural DE showed no difference in event rate (7% per year versus 6% per year; P⫽0.89). Discussion A B LV vs RV LV vs RV Figure 3. Midventricular short-axis delayed enhanced image from 2 HCM patients, both with extensive DE but with significantly different clinical courses. A, NYHA class III with an EF of 40% and 30% DE in LV. B, NYHA class I with an EF of 65% and 46% DE in LV. VS indicates ventricular septum; RV, right ventricle. Contrast-enhanced CMR imaging provides a novel and noninvasive method for in vivo identification and quantification of myocardial fibrosis.16 –18,20,21,35,36 In patients with dilated cardiomyopathy or after myocardial infarction due to coronary artery disease, the presence of DE has been reported to be an independent predictor of ventricular arrhythmias and cardiovascular mortality.22–24,28,36 In HCM, myocardial scars have been commonly reported in necropsy studies9 and by fixed defects on myocardial perfusion imaging15 and it has been suggested that DE represents myocardial fibrosis in this disease, 9,11–13,25,29,37– 42 as initially recognized by Choudhury et al.11 However, whether DE in HCM are associated with adverse clinical consequences similar to those in coronary artery disease and other nonischemic cardiomyopathies is unresolved. Therefore, we have sought here, in a sizeable 188 Circ Heart Fail Table 2. September 2008 Clinical and Demographic Findings According to EF in HCM Patients with DE Patients, n Age, y Total ⱖ60% 51%–59% ⱕ50% 111 92 9 10 43⫾17 43⫾17 46⫾17 43⫾22 0.9 P value – Male, n (%) 78 (70) 66 (72) 5 (56) 7 (70) 0.6 LV end-diastolic dimension, mm 53⫾7 52⫾6 53⫾9 58⫾9 0.14 Maximum LV thickness, mm 23⫾5 24⫾5 20⫾3 20⫾5 0.008 LV mass, g 219⫾85 226⫾89 171⫾31 203⫾70 0.08 LV mass index, g/m 113⫾37 116⫾37 91⫾21 110⫾43 0.08 DE, g 19⫾21 16⫾18 19⫾23 47⫾28 0.005 %DE 9⫾11 7⫾8 12⫾17 27⫾17 0.004 NYHA class, n (%) 0.4 61 (55) 54 (59) 4 (44) 3 (30) II 31 (30) 23 (25) 3 (33) 5 (50) III/IV 19 (17) 15 (16) 2 (22) 2 (20) DE pattern, n (%) 0.013 Transmural 58 (53) 44 (49) 4 (44) 10 (100) Nontransmural 53 (48) 48 (51) 5 (56) 0 (0) Only subepicardial 8 (7) 8 (9) 0 (0) 0 (0) Only midmyocardial 17 (15) 16 (17) 1 (11) 0 (0) Only subendocardial 9 (8) 9 (10) 0 (0) 0 (0) ⱖ2 nontransmural distributions 7 (6) 7 (8) 0 (0) 0 (0) 12 (11) 8 (9) 4 (44) 0 (0) Only at RV insertion into LV 0.006 0.029 RV indicates right ventricle. 30 25 P=0.004 20 15 10 1.00 0.95 0.90 0.85 DE (-) DE (+) p=0.5 0.80 5 0 and the occurrence of heart failure symptoms. Indeed, ⬎75% of our HCM patients with advanced and disabling symptoms showed areas of DE, often involving extensive areas of LV myocardium. Furthermore, the present data demonstrate an inverse relationship between the presence and extent of DE and LV EF, with DE an independent determinant of systolic dysfunction (ie, end-stage phase, with EF ⱕ50%).43 Patients in the end stage showed transmural and extensive DE occupying on average ⬇25% of LV myocardium, greatly exceeding that in our patients with preserved LV function. These findings are consistent with 2 recent case reports in which the explanted hearts of patients in the end stage of HCM were analyzed in detail to show a morphological Event-free rate HCM cohort studied with CMR, to characterize the clinical significance of DE and to analyze its relationship to a variety of disease variables. DE by contrast-enhanced CMR was present in ⬇50% of patients in our HCM study cohort, a prevalence somewhat less than that previously reported by other investigators.11,38 In addition, when present, the extent of DE proved to be substantial, occupying on average ⬇10% of overall LV myocardial volume. This extent of DE observed in HCM is similar to that reported after myocardial infarction,19,23 raising the consideration of whether myocardial fibrosis or scarring in this genetic cardiomyopathy is a determinant of increased risk for sudden death or disease progression due to heart failure. In this regard, our data demonstrate a modest relationship between the presence (but not necessarily the extent) of DE % Myocardium with DE Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 I 0 ≤50 ≥60 51-59 Ejection Fraction (%) Figure 4. Comparison of %DE in HCM patients with EF ⱕ50%, 51% to 59%, and ⱖ60%. 0.5 1 1.5 2 2.5 3 Follow-up Duration (years) Figure 5. Kaplan-Meier survival estimates for the composite end-point of sudden death, appropriate ICD discharge, and progressive heart failure symptoms in patients with and without DE. Maron et al Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 correlation between CMR-DE and extensive areas of myocardial fibrosis.39,42 The recognition that CMR has the capability to identify the end-stage phase of HCM by virtue of calculated EF and myocardial fibrosis has important clinical implications, as end-stage patients experience a high rate of unfavorable disease consequences, including progressive heart failure (often requiring heart transplantation) and sudden unexpected death (prompting consideration for prophylactic defibrillator implantation).1,2,43 However, whether extensive DE identified by CMR will ultimately prove to be a primary marker and prospectively portend susceptibility for progression to the end stage before development of systolic dysfunction is presently unresolved. Nevertheless, taken together, the present data demonstrating an association between DE and both heart failure and systolic dysfunction suggest that myocardial fibrosis has an important role in symptom production and adverse remodeling among HCM patients. On the other hand, we also identified a sizeable and novel subgroup of asymptomatic patients with preserved EF in whom, paradoxically, extensive and often transmural myocardial DE was present. Furthermore, many of these patients with substantial amounts of DE have already achieved advanced ages, free of LV remodeling, arrhythmia-related events, or heart failure. That these patients have not experienced adverse consequences from their myocardial fibrosis over many years suggests that DE may result in very different clinical consequences within the broad clinical spectrum of this disease. Our findings also underscore the principle that complex and multifactorial pathophysiologic mechanisms are likely responsible for disease progression in HCM and that myocardial fibrosis may not be the sole or primary determinant of adverse consequences.4,44 Nevertheless, given the present data and uncertainty in this area, it would seem judicious for HCM patients with DE to undergo regular clinical surveillance (including serial CMR imaging) for prospective detection of changes in symptoms and LV remodeling. Moon et al,38 using HCM risk factors as surrogates for sudden death events in a retrospective study, suggested that DE may fulfill the aspiration as a predictor for future arrhythmic events and prognosis. However, whereas our prospective (short-term) outcome data obtained over an average of almost 2 years showed the adverse cardiovascular event rate to be numerically higher in association with the presence of DE, this difference did not achieve statistical significance. This outcome analysis was clearly underpowered considering the low event rate characteristic of HCM. A substantially longer follow-up period will be required in a particularly large patient population to achieve adequately powered positive or negative data in this respect. Therefore, it is possible that longer longitudinal observation periods (ie, ⬇5 to 7 years) will allow the presence (or extent) of DE to be fully analyzed and emerge as a possible independent risk factor for sudden death and disease progression. In addition, it is conceivable that novel CMR-based techniques for identifying specific areas of histologically abnormal myocardium, such as reported in coronary artery disease (using intermediate signal intensity thresholding to define the infarct border zone),23 may also emerge as a more reliable Delayed Enhancement in HCM 189 predictor in this patient population. Although it is premature at this early juncture to broadly apply DE by contrastenhanced CMR as a primary risk stratification strategy to HCM, it may nevertheless be reasonable in selected patients (and on a case-by-case basis) to assign weight to DE as an arbitrator in reaching difficult clinical decisions for primary prevention ICDs,45 particularly when ambiguity remains regarding risk level after the assessment of conventional risk factors.46,47 To define DE in this analysis, we chose a methodology which used the cutoff point of ⱖ6 SDs above the mean signal intensity of normal myocardium. At present, a general consensus is lacking on this criterion (particularly in nonischemic cardiomyopathy), with previous investigators using a variety of strategies for the identification of DE, including visual assessment (without thresholding)34,48 and also 2-SD34,48 and 6-SD thresholds.18,27,33,34,48 In our experience, the amount of DE quantified with the 6-SD technique most closely approximates that assessed by visual inspection, with the 2-SD cutoff point yielding 22% greater amounts of DE than 6 SDs.49 Therefore, our decision to use a 6-SD threshold was based on the view that it provides the highest specificity for detection and quantification of myocardial fibrosis.16,33,34 Indeed, considering the extensive amount of DE in the patients reported here using this methodology, it is unlikely that we have significantly underestimated the extent of fibrosis present in our HCM cohort. In conclusion, in a large hospital-based population of HCM patients, DE was common and often occupied significant proportions of LV myocardium. DE was associated with heart failure symptoms and a strong determinant of LV dysfunction (ie, end-stage phase). Paradoxically, significant amounts of DE were also present in many asymptomatic (or mildly symptomatic) HCM patients with preserved LV function. Therefore, DE (ie, myocardial fibrosis) appears to have an important role in the clinical course of many HCM patients but may also be associated with substantially different disease consequences. Nevertheless, at present, DE cannot yet be regarded as an independent risk factor for adverse disease outcome and risk for sudden death in HCM, and prudent restraint is justified before broadly applying the results of contrast-enhanced CMR to clinical decision-making strategies in this disease. These present data also underscore the necessity of long-term follow-up studies to ultimately define the prognostic significance of this newly identified CMRbased component of the cardiomyopathic process in HCM. Disclosures None. References 1. Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308 –1320. 2. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, III, Spirito P, Ten Cate FJ, Wigle ED. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Car- 190 3. 4. 5. 6. 7. 8. Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Circ Heart Fail September 2008 diology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42: 1687–1713. Wigle ED, Rakowski H, Kimball BP, Williams WG. Hypertrophic cardiomyopathy. Clinical spectrum and treatment. Circulation. 1995;92: 1680 –1692. Autore C, Bernabo P, Barilla CS, Bruzzi P, Spirito P. The prognostic importance of left ventricular outflow obstruction in hypertrophic cardiomyopathy varies in relation to the severity of symptoms. J Am Coll Cardiol. 2005;45:1076 –1080. Elliott PM, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava A, Mahon NG, McKenna WJ. Sudden death in hypertrophic cardiomyopathy: identification of high risk patients. J Am Coll Cardiol. 2000;36: 2212–2218. Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron BJ. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med. 2000;342:1778 –1785. Seidman JG, Seidman C. The genetic basis for cardiomyopathy: from mutation identification to mechanistic paradigms. Cell. 2001;104: 557–567. Maron MS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, Cecchi F, Maron BJ. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003; 348:295–303. Basso C, Thiene G, Corrado D, Buja G, Melacini P, Nava A. Hypertrophic cardiomyopathy and sudden death in the young: pathologic evidence of myocardial ischemia. Hum Pathol. 2000;31:988 –998. Lombardi R, Betocchi S, Losi MA, Tocchetti CG, Aversa M, Miranda M, D’Alessandro G, Cacace A, Ciampi Q, Chiariello M. Myocardial collagen turnover in hypertrophic cardiomyopathy. Circulation. 2003;108: 1455–1460. Choudhury L, Mahrholdt H, Wagner A, Choi KM, Elliott MD, Klocke FJ, Bonow RO, Judd RM, Kim RJ. Myocardial scarring in asymptomatic or mildly symptomatic patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;40:2156 –2164. Shirani J, Pick R, Roberts WC, Maron BJ. Morphology and significance of the left ventricular collagen network in young patients with hypertrophic cardiomyopathy and sudden cardiac death. J Am Coll Cardiol. 2000;35:36 – 44. Varnava AM, Elliott PM, Sharma S, McKenna WJ, Davies MJ. Hypertrophic cardiomyopathy: the interrelation of disarray, fibrosis, and small vessel disease. Heart. 2000;84:476 – 482. Fassbach M, Schwartzkopff B. Elevated serum markers for collagen synthesis in patients with hypertrophic cardiomyopathy and diastolic dysfunction. Z Kardiol. 2005;94:328 –335. O’Gara PT, Bonow RO, Maron BJ, Damske BA, Van Lingen A, Bacharach SL, Larson SM, Epstein SE. Myocardial perfusion abnormalities in patients with hypertrophic cardiomyopathy: assessment with thallium-201 emission computed tomography. Circulation. 1987;76: 1214 –1223. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100:1992–2002. Fieno DS, Kim RJ, Chen EL, Lomasney JW, Klocke FJ, Judd RM. Contrast-enhanced magnetic resonance imaging of myocardium at risk: distinction between reversible and irreversible injury throughout infarct healing. J Am Coll Cardiol. 2000;36:1985–1991. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. Mahrholdt H, Wagner A, Holly TA, Elliott MD, Bonow RO, Kim RJ, Judd RM. Reproducibility of chronic infarct size measurement by contrast-enhanced magnetic resonance imaging. Circulation. 2002;106: 2322–2327. Pennell DJ. Cardiovascular magnetic resonance: twenty-first century solutions in cardiology. Clin Med. 2003;3:273–278. Lima JA, Desai MY. Cardiovascular magnetic resonance imaging: current and emerging applications. J Am Coll Cardiol. 2004;44: 1164 –1171. Assomull RG, Prasad SK, Lyne J, Smith G, Burman ED, Khan M, Sheppard MN, Poole-Wilson PA, Pennell DJ. Cardiovascular magnetic resonance, fibrosis, and prognosis in dilated cardiomyopathy. J Am Coll Cardiol. 2006;48:1977–1985. 23. Yan AT, Shayne AJ, Brown KA, Gupta SN, Chan CW, Luu TM, Di Carli MF, Reynolds HG, Stevenson WG, Kwong RY. Characterization of the peri-infarct zone by contrast-enhanced cardiac magnetic resonance imaging is a powerful predictor of post-myocardial infarction mortality. Circulation. 2006;114:32–39. 24. Kwong RY, Chan AK, Brown KA, Chan CW, Reynolds HG, Tsang S, Davis RB. Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. Circulation. 2006; 113:2733–2743. 25. Mahrholdt H, Wagner A, Judd RM, Sechtem U, Kim RJ. Delayed enhancement cardiovascular magnetic resonance assessment of nonischaemic cardiomyopathies. Eur Heart J. 2005;26:1461–1474. 26. Rochitte CE, Tassi EM, Shiozaki AA. The emerging role of MRI in the diagnosis and management of cardiomyopathies. Curr Cardiol Rep. 2006; 8:44 –52. 27. Nazarian S, Bluemke DA, Lardo AC, Zviman MM, Watkins SP, Dickfeld TL, Meininger GR, Roguin A, Calkins H, Tomaselli GF, Weiss RG, Berger RD, Lima JA, Halperin HR. Magnetic resonance assessment of the substrate for inducible ventricular tachycardia in nonischemic cardiomyopathy. Circulation. 2005;112:2821–2825. 28. Kramer CM. The expanding prognostic role of late gadolinium enhanced cardiac magnetic resonance. J Am Coll Cardiol. 2006;48:1986 –1987. 29. Kim RJ, Judd RM. Gadolinium-enhanced magnetic resonance imaging in hypertrophic cardiomyopathy: in vivo imaging of the pathologic substrate for premature cardiac death? J Am Coll Cardiol. 2003;41:1568 –1572. 30. Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. 31. Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU, Pennell DJ. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90:29 –34. 32. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, Pennell DJ, Rumberger JA, Ryan T, Verani MS. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Int J Cardiovasc Imaging. 2002;18: 539 –542. 33. Beek AM, Kuhl HP, Bondarenko O, Twisk JW, Hofman MB, van Dockum WG, Visser CA, van Rossum AC. Delayed contrast-enhanced magnetic resonance imaging for the prediction of regional functional improvement after acute myocardial infarction. J Am Coll Cardiol. 2003; 42:895–901. 34. Bondarenko O, Beek AM, Hofman MB, Kuhl HP, Twisk JW, van Dockum WG, Visser CA, van Rossum AC. Standardizing the definition of hyperenhancement in the quantitative assessment of infarct size and myocardial viability using delayed contrast-enhanced CMR. J Cardiovasc Magn Reson. 2005;7:481– 485. 35. Tandri H, Saranathan M, Rodriguez ER, Martinez C, Bomma C, Nasir K, Rosen B, Lima JA, Calkins H, Bluemke DA. Noninvasive detection of myocardial fibrosis in arrhythmogenic right ventricular cardiomyopathy using delayed-enhancement magnetic resonance imaging. J Am Coll Cardiol. 2005;45:98 –103. 36. Bello D, Fieno DS, Kim RJ, Pereles FS, Passman R, Song G, Kadish AH, Goldberger JJ. Infarct morphology identifies patients with substrate for sustained ventricular tachycardia. J Am Coll Cardiol. 2005;45: 1104 –1108. 37. Knaapen P, van Dockum WG, Bondarenko O, Kok WE, Gotte MJ, Boellaard R, Beek AM, Visser CA, van Rossum AC, Lammertsma AA, Visser FC. Delayed contrast enhancement and perfusable tissue index in hypertrophic cardiomyopathy: comparison between cardiac MRI and PET. J Nucl Med. 2005;46:923–929. 38. Moon JC, McKenna WJ, McCrohon JA, Elliott PM, Smith GC, Pennell DJ. Toward clinical risk assessment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance. J Am Coll Cardiol. 2003; 41:1561–1567. Maron et al Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 39. Papavassiliu T, Schnabel P, Schroder M, Borggrefe M. CMR scarring in a patient with hypertrophic cardiomyopathy correlates well with histological findings of fibrosis. Eur Heart J. 2005;26:2395. 40. Wilson JM, Villareal RP, Hariharan R, Massumi A, Muthupillai R, Flamm SD. Magnetic resonance imaging of myocardial fibrosis in hypertrophic cardiomyopathy. Tex Heart Inst J. 2002;29:176 –180. 41. Rickers C, Wilke NM, Jerosch-Herold M, Casey SA, Panse P, Panse N, Weil J, Zenovich AG, Maron BJ. Utility of cardiac magnetic resonance imaging in the diagnosis of hypertrophic cardiomyopathy. Circulation. 2005;112:855– 861. 42. Moon JC, Reed E, Sheppard MN, Elkington AG, Ho SY, Burke M, Petrou M, Pennell DJ. The histologic basis of late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2004;43:2260 –2264. 43. Harris KM, Spirito P, Maron MS, Zenovich AG, Formisano F, Lesser JR, Mackey-Bojack S, Manning WJ, Udelson JE, Maron BJ. Prevalence, clinical profile, and significance of left ventricular remodeling in the end-stage phase of hypertrophic cardiomyopathy. Circulation. 2006;114: 216 –225. 44. Maron MS, Zenovich AG, Casey SA, Link MS, Udelson JE, Aeppli DM, Maron BJ. Significance and relation between magnitude of left ventricular hypertrophy and heart failure symptoms in hypertrophic cardiomyopathy. Am J Cardiol. 2005;95:1329 –1333. Delayed Enhancement in HCM 191 45. Maron BJ MM, Lesser JR, Hauser RG, Haas T, Harrigan CJ, Appelbaum E, Main ML, Roberts WC. Sudden death events in hypertrophic cardiomyopathy can occur in the absence of criteria for high risk status. Am J Cardiol. In press. 46. Maron BJ, Estes NA, III, Maron MS, Almquist AK, Link MS, Udelson JE. Primary prevention of sudden death as a novel treatment strategy in hypertrophic cardiomyopathy. Circulation. 2003;107:2872–2875. 47. Maron BJ, Spirito P, Shen WK, Haas TS, Formisano F, Link MS, Epstein AE, Almquist AK, Daubert JP, Lawrenz T, Boriani G, Estes NA III, Favale S, Piccininno M, Winters SL, Santini M, Betocchi S, Arribas F, Sherrid MV, Buja G, Semsarian C, Bruzzi P. Implantable cardioverterdefibrillators and prevention of sudden cardiac death in hypertrophic cardiomyopathy. JAMA. 2007;298:405– 412. 48. Amado LC, Gerber BL, Gupta SN, Rettmann DW, Szarf G, Schock R, Nasir K, Kraitchman DL, Lima JA. Accurate and objective infarct sizing by contrast-enhanced magnetic resonance imaging in a canine myocardial infarction model. J Am Coll Cardiol. 2004;44:2383–2389. 49. Harrigan CJ, Maron MS, Maron BJ, Peters DC, Gibson CM, Manning WJ, Appelbaum E. Accuracy and reproducibility of quantifying myocardial fibrosis in hypertrophic cardiomyopathy using delayed enhancement cardiovascular magnetic resonance techniques. J Cardiovasc Magn Reson. 11th Annual SCMR Scientific Sessions. 2008;2027:281. CLINICAL PERSPECTIVE In hypertrophic cardiomyopathy (HCM), a myocardial substrate of fibrosis and scarring has been implicated in promoting heart failure and providing a nidus for the generation of ventricular tachyarrhythmias. Contrast-enhanced cardiovascular magnetic resonance with delayed enhancement (DE) now provides a novel, noninvasive method for detecting myocardial fibrosis in vivo in HCM patients. These data report on the clinical profile and significance of DE (ie, fibrosis) in a large cohort of HCM patients. DE was identified in the majority of HCM patients (55%), occupying on average 10% of total left ventricular mass. The extent of DE was inversely related to (r⫽⫺0.3; P⬍0.001) and an independent predictor of (r⫽⫺0.4; P⬍0.001) LV systolic function; patients showing systolic dysfunction (ejection fraction ⬍50%) demonstrated the greatest amount of DE. The presence of DE was modestly related to the occurrence of heart failure symptoms (P⫽0.05), with DE in ⬎75% of patients with advanced limiting symptoms. Paradoxically, substantial amounts of DE were also identified in patients with normal systolic function, many of whom had achieved advanced ages, free of adverse disease consequences. Over a short-term follow-up period, patients with DE experienced more adverse disease events than those without DE, although this difference did not achieve statistical significance. These data demonstrate that DE may result in different clinical consequences within the broad HCM clinical spectrum and strongly support the need for further follow-up studies to more definitively define the prognostic significance of DE in this complex disease. Clinical Profile and Significance of Delayed Enhancement in Hypertrophic Cardiomyopathy Martin S. Maron, Evan Appelbaum, Caitlin J. Harrigan, Jacki Buros, C. Michael Gibson, Connie Hanna, John R. Lesser, James E. Udelson, Warren J. Manning and Barry J. Maron Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 11, 2017 Circ Heart Fail. 2008;1:184-191; originally published online June 23, 2008; doi: 10.1161/CIRCHEARTFAILURE.108.768119 Circulation: Heart Failure is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2008 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 1941-3297 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circheartfailure.ahajournals.org/content/1/3/184 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Heart Failure can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Heart Failure is online at: http://circheartfailure.ahajournals.org//subscriptions/