Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Human vestigiality wikipedia , lookup
Freediving blackout wikipedia , lookup
Cushing reflex wikipedia , lookup
Pre-Bötzinger complex wikipedia , lookup
Intracranial pressure wikipedia , lookup
Homeostasis wikipedia , lookup
Hemodynamics wikipedia , lookup
Biofluid dynamics wikipedia , lookup
Organisms at high altitude wikipedia , lookup
High-altitude adaptation in humans wikipedia , lookup
Circulatory system wikipedia , lookup
Physiology of decompression wikipedia , lookup
Haemodynamic response wikipedia , lookup
Exercise physiology wikipedia , lookup
Common raven physiology wikipedia , lookup
Cardiac output wikipedia , lookup
Alveolar macrophage wikipedia , lookup
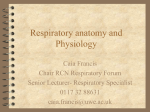
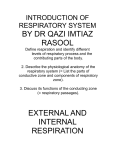
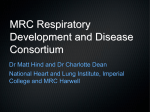
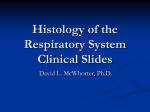
CHAPTER 1 Anatomy and physiology of the human respiratory system R.L. Johnson, Jr., & C.C.W. Hsia Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas, USA. Abstract A brief review of the anatomy and fundamental physiologic concepts of the human respiratory system is presented, including postnatal lung growth and development, mechanical function of the airway and lung parenchyma, alveolar gas exchange, ventilation-perfusion and diffusion-perfusion relationships, alveolar microvascular recruitment, pulmonary circulatory function and respiratory muscle energetics. The emphasis is placed on the close interactions among different respiratory components and between the heart and the lung, which are essential for optimizing oxygen transport in health and disease. 1 Postnatal growth and development 1.1 Anatomy of the adult lung In the right lung there are 3 lobes (upper, middle and lower), which are subdivided into 9 sublobular segments. In the left lung there are 2 lobes (upper and lower), which are subdivided into 8 sublobular segments. There are approximately 23 generations of airways (Z) that distribute respired air to and from the smallest gas-exchange units in the lung (alveoli) [1], Fig. 1. The path length and number of generations from trachea to different acini in the lung are not uniform owing to nonspherical asymmetry. Path lengths from trachea to acini can vary widely. Alveoli are small pockets that bud off of acinar airways, shaped like the cells of a beehive with a hexagonal mouth and a diameter of about 150 µm at birth. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) doi:10.2495/978-1-85312-944-5/01 2 Human Respiration Figure 1: Diagram of the branching airways. Z designates the order of generations with the trachea as zero, followed by bronchi (BR) and bronchioles (BL). On average the first 16 generations are conducting airways that do not participate in gas exchange. The last conducting airway is a terminal bronchiole (TBL), which empties into an acinus. In the acinus there are 3 generations of partially alveolated respiratory bronchioles (RBL) followed by alveolar ducts (AD) that are completely alveolated in adults and empty into an alveolar sac (AS). From Weibel [1]. 1.2 Postnatal development According to Hislop et al [2] conducting airways at birth are miniature versions of those in the adult. No new generations are added after birth; only size and length change during postnatal growth. This is not true of the acinus. Alveoli multiply by adding more alveolar ducts as well as by lengthening of existing ducts and increasing alveolization [3]. The number of alveoli continues to increase after birth (Fig. 2) [4–6], most rapidly in the first 2 years but continues up to age 5 to 8 years. Based on these measurements about 2/3 of the increase in acinar volume during postnatal growth is from an increase in number of alveoli within the first 5 to 8 years and the remaining 1/3 from a steady increase in alveolar size that continues until the lung reaches adult size. Rates of increase in size of the thorax and of the lung WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 3 Number of Alveoli (millions) 400 Adult 300 200 100 0 0 5 10 15 20 25 Years since birth Figure 2: Number of alveoli increase about 15-fold after birth. Alveolar diameter also increases linearly with time after birth until growth is complete [4]; alveolar diameters approximately double, causing an approximate 8-fold increase in volume. must remain exactly matched throughout postnatal growth and there probably exist mechanisms of feedback control between the lungs and thorax controlling this rate. 2 Conducting airways structure and function 2.1 Functional anatomy 2.1.1 Distribution of inspired air Conducting air passages distribute respired air to and from lung acini where gas exchange occurs; they constitute what is called anatomical dead space that must be displaced during inspiration before fresh air reaches the acinus where gas exchange occurs. Upper airways consist of the nasopharynx, oropharynx and glottis. Below the glottis, Fig. 1, there is the trachea followed by an average of 16 generations of dichotomously branching conducting airways down to terminal bronchioles, which average approximately 0.06 cm in diameter. Terminal bronchioles empty into acinar airways where gas exchange occurs in alveolated airways. In each acinus there are approximately 3 generations of respiratory bronchioles that are partially alveolated, and additional generations of alveolar ducts that are completely alveolated, finally ending in alveolar sacs, Fig. 2. Based on Weibel’s model of regular dichotomy [1] there are 65,000 terminal bronchioles in a 3/4 inflated lung to a volume of 4800 ml minus the volume of conducting airways (150 ml); hence, the average size of individual acini would be about 0.072 cm3 . These structures are made up of very fine alveolar septa where circulating red blood cells are separated from alveolar air by a distance of less than a µm [1]. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 4 Human Respiration 2.1.2 Air conditioning and filtering inspired air Another major function of conducting air passages is to humidify the inspired air [7] and filter out small particulate matter to protect this thin gas-exchange surface from dehydration and accumulation of inspired atmospheric debris [8, 9]. Particulates with an aerodynamic diameter larger than 10 µm are filtered out by inertial impact at airway branches and seldom reach an acinus; they are removed by retrograde ciliary transport in the conducting airways to be coughed out or swallowed. A fraction of smaller particulates may sediment out in the central portion of the acinus and be removed by scavenging macrophages or breathed out again without being deposited. There appears to be little difference between the adult and child’s lung in the efficiency of humidification and filtration of particulate matter. If anything, however, the child’s lung may be a little more efficient than the adult lung [2]. 2.2 Viscous resistance to flow in upper airways, lungs and thorax In 1915 Fritz Rohrer [10] published a classic paper describing the quantitative anatomy of the irregular dichotomous branching of airways down to subsegmental airways 1 mm in diameter. These emptied into what he designated as a lobule, which, based on Weibel’s model [10], would be about 5 generations above the acinus. Between the carina of the trachea and lobules in different regions of the lung he measured the numbers of generations, airway diameters and lengths, angles of branching and changes in cross-sectional area at each branch point. Airways dimensions in the lobules were generated by an equation for regular dichotomy derived by von Recklinghausen [11]. Based on the anatomy of the branching airways system and physics of flow in tubes, Rohrer derived the pressure–flow relationships and distribution of ventilation in human airways. Distribution was not uniform because the dichotomous branching was not uniform. Path length from the carina to the lobules varied from 8 cm in the central regions of the lung to 14 cm in the more peripheral regions causing uneven distribution of resistance. The overall pressure drop from nasopharynx to alveoli required to generate increasing flow could be reduced to a single comprehensive equation of the following form: P = K1 V̇ + K2 (V̇ )2 , (1) where P is the pressure drop in cmH2 O across the lung; V̇ is gas flow in l/s; K1 is a constant derived from the summation of laminar-flow resistances in branching airways in cmH2 O/(l/s) and K2 is a constant derived from changing resistance from turbulence and from inertance at airway branch points and at changes in cross-sectional area of the airways; units are in cmH2 O/(l/s)2 . Results reported by Rohrer for resistances across the upper airways, lower airways and total are given in Table 1 [10]. Fifty years later K1 and K2 in eqn. (1) derived by Rohrer have been determined experimentally to describe viscous properties of lung airways, lung tissues and thorax, Table 2. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 5 Table 1: Pressure–flow relationships derived by Rohrer. P = 0.426 · V̇ + 0.714 · (V̇ )2 Upper airways Lower airways Bronchial Lobular P = 0.106 · V̇ + 0.080 · (V̇ )2 P = 0.258 · V̇ + 0.006 · (V̇ )2 Total P = 0.790 · V̇ + 0.800 · (V̇ )2 Table 2: Resistance to airflow in the respiratory system of an average normal person breathing through the mouth or nose [12]. Mouth breathing Flow Resistance Units Air flow Lung tissue Chest wall Resp. system Nasal breathing Laminar Turbulent Laminar Turbulent K1 cmH2 O/(l/s) 1.2 0.2 1.0 2.4 K2 cmH2 O/(l/s)2 0.3 0 0 0.3 K1 cmH2 O/(l/s) 1.8 0.2 1.0 3.0 K2 cmH2 O/(l/s)2 3.0 0 0 3.0 Thus, to describe the pressure in cmH2 O to generate a volume flow of V̇ l/s through the mouth would be P = 2.4V̇ + 0.3 · [V̇ ]2 and through the nose would be P = 3.0V̇ + 3.0·[V̇ ]2 . Results are close to those originally described by Rohrer, particularly when resistances imposed by viscoelastic properties of the lung and thoracic tissues are removed, since these are not a part of Rohrer’s estimates [10]. 2.3 Alveolar ventilation is not uniform even in the normal lung There are space-filling constraints within the lungs and thorax that prevent uniform distribution of ventilation even in the normal lung. As pointed out above, Rohrer found that resistance to flow is greater to peripheral lung lobules than to more central ones [10]. These regional differences in flow resistance do not necessarily mean that ventilation will be nonuniform. The rate at which a lung unit fills is not determined solely by flow resistance; it is in part determined by compliance of the unit (C), where C = the change in volume (V ) divided by the change in filling pressure (P) = V /P in l/cmH2 O. The product RC is the time constant for filling of the unit in seconds. Even if resistance to flow in peripheral units is greater than in more central units ventilation may be the same if RC constants are the same, in analogy to RC constants in an electrical circuit. If RC constants for filling peripheral lobular units are longer than for low-resistance central units, ventilation will become more and WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 6 Human Respiration more nonuniform as the frequency of breathing increases. If RC constants match between central and peripheral units, ventilation will remain uniform in spite of unequal resistances to flow. Rohrer did not measure regional compliances although he discussed this problem. Ross [13] compared measurements and calculations to those of Rohrer in plaster casts of the dog lung between the carina and airways down to 1.5 mm diameter. He also found that airway path lengths varied from 2 cm centrally to 13.7 cm peripherally, with corresponding differences in airway deadspace volumes. Anatomical dead-space volume is the volume of air in conducting airways that must be cleared during a breath before fresh air reaches the alveoli where gas exchange occurs. Alveolar ventilation (V̇A ) is related to total ventilation (V̇T ) as follows: V̇A = V̇T − fVD , where f is frequency of ventilation VD is deadspace volume between the inlet to the alveoli. Thus, even if ventilation to peripheral and central lobules is the same, alveolar ventilation to peripheral lobules will be less because of the larger dead-space volume that must be cleared. The effects of space-filling constraints on airway branching and distribution of ventilation extend all the way down to the alveolar ducts, as pointed out by the work of a number of investigators [13–16]. As pointed out by Johnson and Curtis [17], “because of these space-limiting constraints, irregular branching of the bronchial tree becomes necessary to pack the largest alveolar surface area into a limited space with the least power requirements for distribution of ventilation; the trade off is uneven ventilation.” 2.4 Elastic properties of the lungs and thorax The balance between the static elastic recoil forces in the lungs and thorax determines the pressure–volume relationships of the respiratory system when respiratory muscles are completely relaxed, Fig. 3 [18]. In Fig. 3, at the end of a normal breath when respiratory muscles are relaxed, the inspiratory pressure exerted by recoil of the chest wall exactly balances the expiratory pressure exerted by recoil of the lungs. The lung volume at this balance point is referred to as the functional residual capacity (FRC). The total pressure that is generated by the respiratory system at a given lung volume (excluding muscle) is the algebraic sum of the recoil pressure exerted by the chest and that exerted by the lungs. If the lungs are held at a given volume with the mouth open and unobstructed, the negative intrapleural pressure (i.e., the pressure in the virtual space between the adjacent surfaces of the lung and chest wall) reflects the expiratory recoil pressure of the lungs. We have discussed the pressure required to overcome flow resistance in the airways to inspire, eqn. (1). The additional pressure (P) required to inflate the lungs by a volume V against the elastic recoil pressure of the lungs and thorax is given by P = V /CRS , (2) where CRS is compliance of the lungs and thorax as defined in Fig. 3 and is expressed in l/cmH2 O. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 7 Figure 3: Static pressure–volume curves of lungs and thorax in a normal upright subject. The pressure generated by the total respiratory system at a given lung volume is represented by the heavy curved line. The two thin curved lines represent pressures exerted by the chest wall on the left and by the lungs on the right. A positive sign indicates an expiratory pressure; a negative sign indicates an inspiratory pressure. Reproduced from Miller et al [18]. 2.5 Work of breathing Ventilation requires energy to overcome both elastic and viscous forces in lungs and thorax. Incorporating both eqns. (1) and (2) the following approximations were derived by Otis et al [19]: P= 2 V + K1 V̇ + K2 · V̇ , CRS (3) where V is the volume above the functional residual capacity (FRC) and other symbols are as defined for eqns. (1) and (2). Multiplying both sides by V̇ we have the power requirement at any instant: Instantaneous Power = P V̇ = 2 V · V̇ + K1 · V̇ + K2 · [V̇ ]3 . CRS WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 8 Human Respiration If we assume that ventilation follows a sine-wave pattern, V̇ = V̇P sin(2πft) where V̇P is peak flow in l/s and we assume that energy is required only during inspiration since during quiet breathing the elastic energy during inspiration is stored and returned passively during expiration, we can derive the following equation for estimating energy requirements of quiet breathing: 2 3 Ẇ = Power = (1/2fC RS )[V̇E ]2 + 60 · (K1 /4) π2 V̇E + (2K2 /3) π2 · V̇E , (4) where V̇E has been converted from l/s in eqn. (3) to ventilation in l/min; f is respiratory rate in min−1 ; 60 is s/min so that power is now expressed as cmH2 O·l·min−1 . During exercise, when respiratory muscle energy is active throughout both inspiration and expiration, eqn. (4) can be modified as follows to approximate energy requirements of breathing during heavy exercise: 2 3 Ẇ = 2 · 60 · (K1 /4) π2 · V̇E + (2K2 /3) π2 · V̇E /100. (5) Dividing by 100 converts power from units of cmH2 O·l·min−1 to more familiar engineering units of kg·m·min−1 , Fig. 4. Ventilatory capacity may be limited in the patient because respiratory muscle mass is insufficient to generate the pressures required for a normal ventilatory effort. Another possible limitation of ventilation and exercise capacity in the patient concerns metabolic requirements, which will be considered later. Athlete Power Requirements (kg m/min) 250 Patient with asthma 200 150 100 50 0 0 50 100 150 200 250 Ventilation (l/min) Figure 4: Power requirements are plotted in an athlete assuming normal values of K1 and K2 for lungs and thorax from Table 2 compared to power requirements in a hypothetical patient with asthma assuming about a 5-fold increase of K1 and K2 during an asthmatic attack (i.e., K1 = 10 cmH2 O/(l/s) and K2 = 1.5 cmH2 O/(l/s)2 ). WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 9 3 Mechanisms of gas exchange 3.1 Convective and diffusive distribution and mixing in airways As a front of inspired air moves distally down the airways, the pattern of oxygen transport and mixing within this front changes from a combination of turbulent and laminar convection in the conducting airways to predominantly diffusive mixing as it moves into the acini and finally into the alveoli where alveolar capillary gas exchange occurs. Weibel’s branching model of the airways [1] provides the dimensions of each airway generation. From these dimensions there are two nondimensional numbers that can define critical change in flow patterns from laminar to turbulent, or where diffusive transport becomes faster than convective flow. These flow patterns are important in how inspired air is mixed during inspiration. 3.1.1 Relative importance of laminar and turbulent flow The relative importance of laminar and turbulent flow patterns at different generations in the conducting airways can be derived from the Reynolds number, which is a nondimensional ratio of inertial to viscous forces. The Reynolds number = (y · v)/(µ/ρ) where y = tube diameter in cm, v = linear velocity in cm/s, µ = fluid viscosity in poise and ρ = fluid density in g/cm3 (µ/ρ is called the kinematic viscosity). Turbulence develops normally at corners, sudden changes in direction or airway diameter as at branch points. Once developed, inertial forces tend to maintain turbulence, while viscosity tends to damp it out, depending on the balance between these two forces. Even in unbranched smooth tubes turbulence tends to become sustained when the Reynolds number exceeds 2000. Resistance to laminar flow in airways, K1 in eqn. (3), is directly proportional to viscosity (µ) and volume velocity (V̇ ). Resistance to turbulent flow, K2 , is directly proportional to fluid density and the square of the volume velocity, [V̇ ]2 , as in eqn. (3). Although turbulence increases the power requirements of breathing it is an important source of gas mixing, heat exchange, humidification, filtration of inspired particulate matter and gas mixing in the lung before it reaches the alveoli. 3.1.2 Relative importance of convection and diffusion in transport The relative importance of convective and diffusive transport in different generations of airways can be estimated from the Peclet number (Pe). Pe is a dimensionless ratio of rate of transport by convection down a concentration gradient to the rate of diffusion down the same concentration gradient, i.e., (v · x)/d where v = velocity of convective flow down the tube in cm/s, x = length of the tube in cm and d is the diffusion coefficient of oxygen in respired air given in cm2 /s. As Pe falls below 1.0 the rate of transport by diffusion begins to exceed that by convection. In the lower conducting airways and acini the combination of diffusion and convection provides an important source for mixing of gases not only within each acinus but also between acini. Table 3 summarizes these relationships. During quiet breathing turbulence is minimal except at airway branch points and diffusive transport is WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Trachea Bronchus TB RB1 RB2 RB3 AD1 AD2 AD3 AS Generation 0 6 16 17 18 19 20 21 22 23 131.23 84.17 1.852 0.967 0.467 0.211 0.078 0.035 0.016 0.008 Peak flow‡ cm/s 6151.5 295.9 1.194 0.533 0.214 0.082 0.025 0.010 0.004 0.002 Peclet number 1408.5 140.5 0.663 0.311 0.139 0.059 0.021 0.009 0.004 0.002 Reynolds number 1968.5 1262.6 27.778 14.509 7.011 3.166 1.176 0.530 0.240 0.120 Peak flow‡ cm/s 92273.6 4438.92 17.904 7.991 3.204 1.224 0.381 0.145 0.055 0.023 Peclet number 21128.8 2108.1 9.938 4.672 2.090 0.887 0.316 0.136 0.059 0.029 Reynolds number Exercise ventilation = 100 l/min ‡ Peak = terminal bronchiole entering the acinus; RB = respiratory bronchiole; AD = alveolar duct and AS = alveolar sac. flow during a respiratory cycle is about 3 times the average ventilation. Shaded areas under Peclet numbers designate airways at the given ventilation where rate of diffusive transport exceeds the rate convective transport. Shaded areas under the columns of Reynolds numbers indicate those airways at the given ventilation where turbulence tends to become sustained. ∗ TB Airway∗ Resting ventilation = 6 l/min Table 3: Convective and diffusive gas transport and mixing in the airways between trachea and alveoli. 10 Human Respiration WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 11 much faster that convection in the acinus. During heavy exercise sustained turbulence extends down to subsegmental bronchi and diffusive transport is still faster than convective transport in the alveolar ducts. 3.2 Alveolar gas exchange at equilibrium At steady state the alveolar CO2 and O2 tensions in the lungs are determined by the ventilation relative to the respective rates of CO2 output and O2 uptake. 3.2.1 CO2 equilibrium Thus, the alveolar equation for CO2 states PaCO2 = V̇CO2 · 863, V̇ a (6) where PaCO2 = alveolar CO2 tension, V̇CO2 = CO2 output, V̇ a = Alveolar ventilation and 863 = 760 (body temp. in Kelvin)/273. The difference between end-capillary CO2 content in mM/ml leaving the lung (Cc CO2 ) and mixed venous CO2 content (C v̄CO2 ) entering the lung multiplied by blood flow (Q̇) in ml/min equals the CO2 output (V̇CO2 ) in ml/min. This is the Fick equation for CO2 : V̇CO2 := Q̇(C v̄CO2 − CcCO2 ) · 22.2, where 22.2 = ml/mM. Combining eqns. (6) and (7) and rearranging we have V̇ a/Q̇ CcCO2 = C v̄CO2 − · PaCO2 , 19.2 (7) (8) which, for a given ratio of ventilation to blood flow, V̇ a/Q̇, and the mixed venous CO2 content (C v̄CO2 ) of blood entering the lung tells us the trajectory along which blood CO2 content must fall toward equilibrium with the alveolar CO2 tension (PaCO2 ). The point of equilibrium can be derived graphically from the intersection of this trajectory with the CO2 dissociation curve, Fig. 5. Thus, if we know the ratio of ventilation to perfusion, V̇ a/Q̇, in any region of lung and the mixed venous CO2 content we can estimate the CO2 content in blood leaving that region at equilibrium with the PaCO2 . 3.2.2 O2 equilibrium The same set of equations can be derived for oxygen. The alveolar equation for O2 states that FiN2 PaO2 = (Pb − PH2 O ) · FiO2 − PaCO2 · FiO2 + , (9) R WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 12 Human Respiration End capillary blood Figure 5: CO2 equilibrium between alveolar air and blood leaving lung capillaries at a known mixed venous CO2 content and a ratio of ventilation to perfusion (V̇ a/Q̇) = 3. The solid straight line is eqn. (8) and the curved line is the CO2 dissociation curve. The point of intersection indicates equilibrium. where PaCO2 = alveolar O2 tension; Pb = barometric pressure; PH2 O = water vapor tension at body temperature (47 mmHg at 37◦ C); FiO2 = inspired O2 fraction (approximately 0.21 breathing room air at sea level); FiN2 = inspired N2 fraction (normally taken as 0.78 in room air at sea level). Furthermore, there is also a Fick equation for oxygen: V̇O2 = Q̇(ScO2 − S v̄O2 ) · Cap, (10) where ScO2 and S v̄O2 are fractional oxyhemoglobin saturation in the end-capillary and mixed venous blood, respectively, and Cap is the O2 capacity of blood in ml of O2 /ml blood. Then, combining eqns. (6), (9) and (10), ScO2 − S v̄O2 = PiO2 − PaO2 · FiO2 · V̇ a/Q̇ −· 863 · FiN2 · Cap V̇ a/Q̇ 863 · FiN2 · Cap · PaO2 . (11) Equation (11) determines the trajectory along which oxygen saturation rises from that in mixed venous blood toward equilibration with the alveolar O2 tension (PaO2 ) for a given ratio of V̇ a/Q̇. The point of equilibrium can be derived graphically from the intersection of this trajectory with the oxyhemoglobin dissociation curve, Fig. 6. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System a Oxygen Saturation (%) 100 Oxyhemoglobin dissociation curve Equilibrium VA/Q = 3 VA /Q = 6.0 b 100 13 SaO2 75 75 50 50 mixed venous VA/Q = 0.5 25 25 PAO2 PI O2 - K PaO2 0 0 0 25 50 75 100 125 Oxygen Tension (mmHg) 150 0 25 50 P A O2 75 100 125 150 Oxygen Tension (mmHg) Figure 6: (Panel a) O2 equilibrium between alveolar air and blood leaving lung capillaries at a known inspired O2 tension (PiO2 ) and mixed venous O2 saturation. The solid straight line is eqn. (11) at a ventilation perfusion ratio (V̇ a/Q̇) = 3. The curved line is the O2 dissociation curve. Equilibrium is at the point of intersection. (Panel b) The effect of uneven V̇ a/Q̇. This shows the effect of two regions of lung with equal blood flows but different V̇ a/Q̇ ratios of 6 and 0.5. A mixture of blood from the two regions will have an O2 saturation and PaCO2 approximately halfway between and a resulting increase in PaO2 − PaO2 as indicated in the diagram. After Hsia and Johnson [20]. 3.2.3 Effect of uneven V̇ a/Q̇ ratios in the lung The most efficient gas exchange is achieved when V̇ a/Q̇ ratios are uniform and the alveolar-arterial O2 tension and CO2 tension differences (PaO2 − PaO2 and PaCO2 − PaCO2 ) are zero. Increasing nonuniformity of ventilation with respect to blood flow causes these gradients to increase. Ventilation has to be increased in order to bring the arterial CO2 and O2 tensions back toward normal levels. 3.3 Alveolar capillary gas exchange and physiologic laws of diffusion 3.3.1 Diffusing capacity of the lung (DL ) DL is defined as the rate of transfer of a respired gas between alveolar air and binding sites on hemoglobin in capillary red cells divided by the driving pressure in mmHg and expressed in units of ml·(min·mmHg)−1 . Thus, for oxygen DLO2 = V̇O2 , PaO2 − PcO2 (12) where V̇O2 = Oxygen uptake in ml/min, PaO2 = Alveolar O2 tension and PcO2 = mean oxygen tension of capillary hemoglobin, both in mmHg. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 14 Human Respiration The difficulty with measuring DLO2 arises from the fact that PcO2 changes as blood passes through the lung. Although PaO2 and V̇O2 can be measured PcO2 cannot because it changes during transit until equilibrium is reached or leaves the capillary bed without being accessible to measurement. On the other hand, under conditions used for measuring DLCO changes in PcCO are negligible during transit. CO binds to hemoglobin so tightly that multiple measurements of DLCO can be made before PcCO rises significantly. DLCO can be measured essentially neglecting capillary CO tension as follows: DLCO = V̇CO . PaCO (13) To make this measurement during breath–holding, a test gas is made up containing a small concentration of CO and of an inert insoluble tracer gas such as He or CH4 mixed with a balance a balance of air or oxygen. A measured volume of this mixture is inspired. The breath is held for a measured time interval of about 10 s. Then an expired sample is collected to determine how much CO has disappeared with respect to the inert, insoluble tracer for calculation of DLCO . This is the breathholding technique and is the most common clinical measurement. The inspired breath can also be breathed back and forth in a reservoir bag while the disappearance of CO with respect to the tracer is followed with each breath by a rapid analyzer for calculation of DLCO . The latter is called the rebreathing technique and has the advantage of providing measurements during exercise. A small concentration of acetylene can also be added to the test gas for simultaneous measurement of cardiac output. Nitric oxide also reacts extremely rapidly with hemoglobin and is taken up much more rapidly by red cells than CO. DLNO can be measured by either the breath-holding or rebreathing method simultaneously with measurements of DLCO . However, before going further it is important to review the physical laws involved in these measurements. 3.3.2 Fick’s law of diffusion defines how diffusive transport moves down a concentration gradient The rate of diffusive transport of a gas in a uniform media such as plasma or the alveolar wall is described by Fick’s law of diffusion as follows: dQ ∂C = Ad , dt ∂x (14) where dQ = volume transfer of the gas in cm3 /s in the x direction; dt A = area in cm2 of the barrier through which diffusion is occurring. d = the diffusion coefficient in cm2 /s, and ∂C = concentration gradient through the barrier in the x direction in cm−1 ∂x WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 15 3.3.3 Krogh’s diffusion constant defines how a concentration gradient is translated into a more convenient pressure gradient [21] When a gas diffuses from one media into another where gas solubilities differ, e.g., from alveolar air into alveolar wall, the standard Fick equation does not work well; hence Krogh modified the standard Fick diffusion equation as follows: dQ 6·α·d ∂P =A· · , (15) dt 760 ∂x where dQ = volume transfer in cm3 /min from air through the alveolar wall dt A = surface area of the alveolar wall in cm2 α = Bunsen solubility coefficient in atm−1 d = diffusion coefficient in cm2 /s 6·α·d = Krogh’s diffusion constant in cm2 ·min−1 ·mmHg−1 , 760 ∂P = pressure gradient in mmHg/cm across the wall. ∂x Thus, using Krogh’s constant [21], diffusion is described as being driven by a pressure gradient instead of a concentration gradient. Furthermore, it allows us to translate a membrane-diffusing capacity measured for one gas into that for another gas of different molecular weight and solubility. 3.3.4 Diffusing capacity of the pulmonary membrane (DM ) and its relationship to the Krogh constant This is given by A 60 · α · d A DM = =K· , 760 x x (16) where A is the area and x the thickness of the barrier and DM is the membranediffusing capacity of the lung; α and d are assumed to be similar in tissue and plasma. Approximate values of the Krogh constant are given in Table 4 for different gases that are important in pulmonary physiology. If Krogh diffusion constants are known, measurements of DM for one gas can be translated into an estimate for another gas. For example: DMO2 DMCO = KO2 3.87 . = KCO 3.48 (17) 3.3.5 Rate of uptake of respired gases by red cells involving diffusion and chemical binding Diffusive uptake of respired gases is determined not only by the resistance of the alveolar capillary membrane to diffusion but also by the resistance imposed by WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 16 Human Respiration Table 4: Estimated Krogh diffusion constants (K) in cm2 min−1 · mmHg−1 . Respiratory gases Gases used to measure diffusing capacity Gas Diffusing in N2 ¶ In lung tissue, plasma or water O2 CO2 CO NO 1.79 · 10−2 1.26 · 10−2 1.65 · 10−2 1.59 · 10−2 3.87 · 10−8 # 64.5 · 10−8 ∗ 3.48 · 10−8 # 6.84 · 10−8 ‡ ¶ [22–24]. # Based on measurements in lung tissue; on measurements in plasma; ‡ Based on measurements in water [25]. ∗ Based Table 5: Rate of gas uptake by red cells in a ml of normal whole blood (θ) in (ml·min−1 )STPD ·mmHg−1 gas tension in surrounding plasma*. Gas θ in min−1 · mmHg−1 O2 CO2 CO NO 3.9 5.8 1/(0.73 + 0.0058 · PO2 ) approaching infinity References [28] [29] [26] [30] *θ is estimated for a normal hemoglobin concentration of 14.9 g/dl hence it must be corrected for a deviation from 14.9 by the product θ · [measured Hb/14.9]. diffusion into the red cells and rate of chemical binding to hemoglobin. Specific rates of gas uptake (referred to as θ) have been measured for O2 , CO2 , CO and NO using rapid reaction-rate techniques in red-cell suspensions and the results expressed in terms of [(ml/min)gas uptake/mmHg gas tension]/ml of blood having an O2 capacity of 20 ml/dl. Representative data are given in Table 5 with references. CO competes with O2 for binding sites on hemoglobin; hence, as oxygen tension increases θCO decreases as shown in Table 5 and has provided a method for measuring the true membrane-diffusing capacity for CO and pulmonary capillary blood volume by a technique devised by Roughton and Forster [26, 27]. There is no such competition with oxygen for binding sites by the other gases. 3.3.6 The Roughton–Forster method for estimating membrane-diffusing capacity (DM ) and pulmonary capillary blood volume (Vc ) [27] The Roughton–Forster equation [27] states that the total resistance to oxygen uptake by blood flowing through the lung capillary bed equals the reciprocal of the lung-diffusing capacity of the lung (1/DLO2 ), which in turn is the sum of the resistances in series imposed by the alveolar capillary membrane (1/DMO2 ) and that imposed by red cells in pulmonary capillary blood ((1/θO2 ) · (1/Vc )) as WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 17 summarized below: Total Resistance = Membrane Resistance + Red-Cell Resistance 1 DLO2 = 1 DMO2 + 1 θO2 · 1 . Vc (18) Similar equations can be set up for DLCO measured at two or more alveolar oxygen tensions, eqns. (19) and (20). As oxygen tension increases 1/θCO increases and the measured DLCO correspondingly falls, Table 5; hence at two different oxygen tensions the Roughton–Forster equation [27] yields two simultaneous equations with two unknowns that can be solved for DMCO and Vc . 1 1 1 1 + = · (19) DLCO O2 DMCO θCO O2 Vc 1 1 1 1 + = · . (20) DLCO Air DMCO θCO Air Vc The Krogh constants for O2 and CO from Table 4 and θO2 from Table 5 can then be used to estimate DLO2 from the DMCO and Vc derived from the two simultaneous equations, again using the Roughton–Forster equation as follows: 1 DLO2 = KCO 1 1 + · . KO2 DMCO θO2 Vc (21) More recently, methods have been developed to measure DLNO and DLCO simultaneously. NO reacts so rapidly with hemoglobin in red cells that the resistance imposed by the red cell to NO uptake approaches zero and DLNO is the same as DMNO . Based on this assumption DMCO and Vc can be estimated empirically from the following modification of the Roughton–Forster equation: 1 1 1 1 = + · . DLCO 2.4 · DLNO θCO Vc (22) 3.3.7 Recruitment of diffusing capacity during exercise During exercise all components of DLCO increase in an approximately linear relationship to cardiac output and a plateau is not reached within the physiological range, Fig. 7. DLO2 has been estimated indirectly from DMCO and Vc as illustrated in the previous sections and is about 50% higher at any given cardiac output than DLCO . DLO2 is higher primarily because the rate of uptake of oxygen by red cells is much faster than the rate of uptake of CO. DLNO is approximately 4 times DLCO at the same cardiac output primarily because of its greater solubility in lung tissue and because the red cells offer little resistance to NO uptake. 3.3.8 The importance of the relationship between DLO2 and cardiac output [20] If DLO2 did not increase as cardiac output increases during exercise arterial oxyhemoglobin desaturation would occur at relatively low levels of exercise. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 18 Human Respiration Figure 7: Diffusing capacity of the lung for CO, O2 and NO (not shown here) increase from rest to heavy exercise in a linear relationship with cardiac output and does not reach a plateau over the physiological range of measurement. From eqns. (10) and (12): V̇O2 = Q̇ ScO2 − S v̄O2 · Cap V̇O2 = DLO2 · PaO2 − PcO2 , it is possible to derive that the ratio of diffusing capacity to pulmonary capillary blood flow, DLO2 /Q̇c bears the following relationship to oxygen saturation of blood leaving lung capillaries (ScO2 ) when mixed venous oxygen saturation (S v̄O2 ) and alveolar oxygen tension (PaO2 ) are known: DLO2 Q̇c = Cap ScO S v̄O2 2 d(ScO2 ) . (PaO2 − PcO2 ) (23) In order to numerically integrate the right-hand side of eqn. (23) to calculate the relationship between ScO2 and DLO2 /Q̇c at rest and exercise the shape and position of the oxyhemoglobin dissociation curve must be known. This can be provided with reasonable accuracy by the Hill equation in the following form PcO2 = P50 [ScO2 /(1 − ScO2 )]0.37 . The P50 is the oxygen tension at which the hemoglobin saturation (ScO2 ) is 50%. The P50 represents the position of the curve that changes when body temperature, blood PCO2 , or pH change, for example with exercise. The shape of the curve remains fixed. Under normal resting conditions the P50 is 26.5 mmHg but increases during exercise as body temperature increases and pH falls. We have calculated the relationship between end-capillary oxygen saturation ScO2 and DLO2 /Q̇c as illustrated in Fig. 8. Results show that as DLO2 /Q̇c falls during exercise oxygen saturation of blood leaving the lung remains almost fixed until a critical level is exceeded when ScO2 WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 19 Figure 8: As the ratio of DLO2 /Q̇c moves below a critical point, there is a rapid fall of oxygen saturation of blood as it leaves the lung. The fall occurs earlier at a low alveolar oxygen tension such as at high altitude or when the P50 of hemoglobin falls as when the pH declines during heavy exercise or when body temperature rises. From Hsia and Johnson [20]. falls rapidly. Data was calculated to show the effect of changing alveolar PO2 between 110 to 80 mmHg, equivalent to that expected during exercise at sea level and at an altitude of 10,000 feet, respectively. Data was also calculated to show the effect of changing arterial pH from 7.4 to 7.2 as occurs from rest to heavy exercise. Now we can address the question of what would happen to arterial O2 saturation if DLO2 remained fixed from rest to exercise. At sea level, at rest, DLO2 /Q̇c would be about 7.5 and ScO2 would be in equilibrium with PaO2 at about 97.5%. By the time cardiac output reached 22 L/min ScO2 would have fallen to about 80%. At 10,000 feet arterial saturation would fall to between 70 and 80% at a cardiac output of 15 l/min if DLO2 failed to rise above its resting level. Why then doesn’t the system operate with the pulmonary capillary bed fully recruited at rest? As will be discussed in the next section, part of the explanation arises from the fact that the pulmonary circulation must operate at low pressures. In the upright position the pulmonary artery pressure at rest or light exercise is too low to completely recruit the upper lobes of the lung. 4 Pulmonary circulation 4.1 A low-pressure system The pulmonary circulation is a low-pressure system relative to the systemic circulation, Fig. 9. It has to operate at a relatively low pressure level in order to sustain rapid diffusive gas exchange between inspired air and the cardiac output as it is pumped at a high rate through thin walled capillaries. The high rate of diffusion requires a thin WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 20 Human Respiration 50 Mean Pulmonary Vascular Pressures (mmHg) Pulmonary Artery Capillary Wedge 40 30 20 10 0 0 10 20 30 Cardiac Output (l/min) Figure 9: Mean vascular pressures are much lower in the lung than in the systemic circulation. This is necessary to avoid stress failure of the pulmonary capillaries during exercise. membrane that must be protected from pressure damage. For proper perspective it helps to visualize the actual dimensions within which this gas exchange occurs. The pulmonary capillary bed contains 100 to 200 ml of blood enclosed within a thin membrane wall of about 1 µm average thickness and spread over a surface area that is the size of a tennis court. At rest it operates at a mean pulmonary artery (PA) pressure of about 15 mmHg (compared to a mean systemic arterial pressure of about 90 mmHg) and at peak exercise rises to between 30 to 40 mmHg. Pulmonary capillary wedge (PCW) pressure may approach between 20 to 25 mmHg. Capillary pressures not too much higher than that can cause pulmonary edema and hemorrhage by stress failure in pulmonary capillaries [31]. 4.2 The pulmonary vascular waterfall and lung zones The top of the upright human lung is about 25 to 30 cm above the mid-right ventricle (RV). Thus, at rest the RV must generate a PA pressure head of about 18 to 22 mmHg to reach the top of the lung; however, at rest it operates at a PA pressure of only about 15 mmHg. Hence, at rest the perfusion pressure to the apical 20% of the lung is zero and this region is only perfused by the bronchial circulation that operates at systemic pressure and keeps the region viable. Because the pulmonary circulation operates at such low pressures it is considered to be functionally divided into 3 pressure zones. In a region where PA pressure is lower than arterial hydrostatic pressure, capillary perfusion pressure is zero and the region operates under zone-1 conditions. In a region where RV pressure exceeds both arterial hydrostatic and alveolar pressures but venous hydrostatic pressure is lower than alveolar pressure, a waterfall condition occurs. Capillary blood exits the alveoli down a waterfall to the lower venous pressure. The capillary perfusion pressure becomes arterial minus WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 21 Figure 10: Uneven distribution of blood flow (Q̇c /VA ) and diffusing capacity (DL /VA ) from lung apex to base owing to the high hydrostatic pressure relative to right ventricular pressure at rest. The upper 20% of the lung is not perfused at rest except by the high-pressure bronchial circulation (i.e., Q̇c /VA = 0). From Michaelson et al [36]. alveolar pressure (Part – Palv ); this is a zone-2 condition. In a region where both arterial and venous pressures exceed hydrostatic and alveolar pressure, perfusion pressure becomes arterial minus venous pressure (Part – Pven ); this is a zone-3 condition. These kinds of zones are unique to the lung where blood vessels are collapsible and changes in alveolar pressure can collapse or dilate the capillaries to change their resistance or where at zero alveolar pressure capillaries can collapse in a region where hydrostatic pressure is less than zero; blood will be sucked out as if falling down a waterfall [32, 33]. Regions operating under zone-1 conditions do not participate in gas exchange. The capillary bed is only partially open under zone-2 conditions but may be completely open in zone-3. These zone conditions create an uneven distribution of blood flow and diffusing capacity imposed by gravitational stresses from the top to the base of the lung [34, 35] even in normal subjects, Fig. 10. During exercise, zone 3 moves up as pulmonary arterial and capillary wedge pressure increase. More capillaries open and this is one source of capillary recruitment and increase in diffusing capacity but probably not the major source. There may be even greater recruitment, however, within isogravitational planes [37]. 5 Respiratory muscles 5.1 Innervation and muscle mass of respiratory muscles Inspiratory and expiratory muscle groups are shown in Fig. 11 along with their segmental innervation. Inspiratory muscles receive most of their segmental innervation WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 22 Human Respiration Figure 11: Respiratory muscles and their segmental innervation. The intercartilagenous portions of the internal intercostals supplied by T1 to T4 (parasternals) are inspiratory muscles. After Miller et al [18]. from cervical and thoracic segments, expiratory muscles from thoracic and lumbar segments. Systematic measures of respiratory muscle mass in humans is only available for the diaphragm at post mortem [38]. For humans with sedentary occupations, diaphragm weight (g) = 4.18 · body weight (kg) – 21.8. Muscle mass and capability for generating power of all respiratory muscles have been measured in dogs where the diaphragm weight (g) = 5 · body weight (kg), on average about 28% higher than in sedentary humans [39, 40]. However, in humans with occupations requiring heavy labor, the weight of the diaphragm is only about 10% lower than in the dog. Segmental innervations are the same in humans and dogs. Hence studies on muscle mass and power capabilities of respiratory muscles in dogs probably provide a good first approximation to respiratory muscle function in humans. The diaphragm is the most important respiratory muscle in both species. In the dog, the diaphragm constitutes only 9% of the respiratory muscle mass but supplies 30 to 40 per cent of the ventilatory power. Inspiratory muscles in general constitute only 40% of the respiratory muscle mass but deliver more than 70% of the total power for breathing during exercise. 5.2 Oxygen requirements of breathing Oxidation of carbohydrates yields approximately 5 cal/mlO2 and one (kg·m) of mechanical energy is equivalent to 2.33 cal of heat energy, hence 0.5 ml of oxygen would be needed to support one (kg·m) kg m of mechanical work if all of the energy generated by burning carbohydrate could be utilized (100% efficiency). Mechanical efficiency of the respiratory muscles has been measured at 20 to 25% in both the dog and human [41, 42]; this is essentially the same as other exercising skeletal muscle. Hence, assuming 25% efficiency, each (kg·m) of mechanical work generated will WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 23 require approximately 2 ml of oxygen uptake. Respiratory muscles are an essential part of the oxygen-transport system to provide oxygen for exercise. However, respiratory-muscle function comes at a metabolic cost measured by the oxygen cost of breathing. From the data used to generate Fig. 4 describing power requirements of ventilation Tables 6 and 7 have been set up to show oxygen requirements of breathing and possible mechanisms whereby muscles of breathing can limit exercise. 5.3 Possible limits imposed by respiratory muscles in Olympic athletes Calculations in Table 6 are based on measurements in an Olympic bicyclist with a maximal O2 uptake of 6.14 l/min, maximal ventilation of 200 l/min and a maximal cardiac output of about 35 l/min [43]. We used eqn. (5) to calculate the mechanical power required to support ventilation as bicycle workload increases, assuming normal K1 and K2 for mouth breathing, Table 2. Mechanical power was converted to oxygen requirements assuming carbohydrate metabolism for which 2 ml of oxygen are required to support each 1 kg·m of mechanical work at mechanical efficiency of 25%. Based on these calculations at maximal bicycle workload O2 requirements of respiratory muscles would be 0.334 l/min, which would be 5.4% of the total O2 uptake. Blood-flow requirements of respiratory muscles necessary to supply oxygen needs were calculated assuming an arterial O2 saturation of 95% with 95% extraction of oxygen delivered. Based on these calculations blood flow to respiratory muscles at maximal O2 uptake would be 1.76 l/min, 5% of the cardiac output. If the diaphragm were generating 30% of the mechanical work of breathing, as has been measured in the dog, diaphragm blood flow would be 528 ml/min. If the diaphragm weight is 5 gram/kg body weight, blood flow to the diaphragm of this 75-kg athlete would be 1.4 ml/min/g of muscle. The highest blood flow that we have seen in the dog diaphragm under extreme conditions of inspiratory loading averaged 2 ml/min/g of muscle [39]; hence this estimated diaphragm blood flow at peak exercise is a reasonable magnitude in the athlete but might be approaching an upper limit. More than likely in the Olympic athlete all transport steps, maximal cardiac output, maximal power development by the respiratory muscles and maximal power from exercising skeletal muscles are approaching upper limits at the same time. 5.4 Possible limits imposed by respiratory muscles in a patient with asthma The situation is different in the asthmatic patient described in Table 7 where similar calculations have been made to those in Table 6, except that K1 and K2 are assumed to be 5-fold higher for estimating the greater power requirements of breathing in asthma and mechanical efficiency is less. Note in the last column of the table that in this patient the oxygen requirements of the respiratory muscles become so great that any attempt to increase ventilation above 100 l/min provides no further increase in oxygen for the rest of the body including locomotor muscle. Exercise could not be sustained at this level. Total body oxygen uptake that could be sustained would WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 60 80 100 120 140 160 180 200 12.6 15.7 18.9 22.1 25.3 28.5 31.7 34.9 0.019 0.036 0.061 0.095 0.138 0.191 0.256 0.334 1.0 1.5 2.0 2.6 3.2 3.9 4.6 5.4 0.1 0.192 0.323 0.499 0.724 1.000 1.350 1.760 0.8 1.2 1.7 2.3 2.9 3.9 4.3 5.0 1.82 2.41 3.01 3.59 4.15 4.72 5.26 5.81 *Assuming K1 = 2.4 cmH2 O/(l/s) and K2 = 0.3 cmH2 O/(l/s)2 in eqn. (5), an alveolar ventilation 80% of the total so that each 20 l/min increase in ventilation provides 0.61 l/min utilizable O2 , 25% mechanical efficiency for muscles of breathing, O2 capacity of 0.2 l O2 /l of blood and 95% O2 extraction by exercising muscles. 1.94 2.45 3.07 3.68 4.29 4.91 5.52 6.14 Total O2 uptake Ventilation Cardiac output RM O2 uptake RM O2 uptake RM blood flow RM blood flow O2 available for (l/min) (l/min) (l/min) (l/min) (% of total) (l/min) (% of total) exercise (l/min) Table 6: Total O2 uptake during exercise in an athlete plus per cent of the total required by respiratory muscles (RM) for energy requirements of breathing and that left over for sustaining exercise*. 24 Human Respiration WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 20 40 60 80 100 120 140 160 180 5.0 7.9 9.0 11.0 13.0 15.0 16.9 19.0 20.9 0.018 0.083 0.207 0.403 0.685 1.066 1.558 2.175 2.93 4.7 10.8 18.0 26.3 35.7 46.3 58.1 70.8 84.9 0.10 0.44 1.09 2.12 3.61 5.61 8.20 11.45 15.42 2.0 6.3 12.1 19.3 27.8 37.4 48.5 60.3 73.8 0.36 0.69 0.94 1.13 1.24 1.23 1.12 0.89 0.52 *Assuming K1 = 10 cmH2 O/(l/s) and K2 = 1.5 cmH2 O/(l/s)2 in eqn. (5), alveolar ventilation = 50% of total ventilation so that each increment 20 l/min ventilation provides 0.35 l/min of utilizable O2 , 10% mechanical efficiency for muscles of breathing, an O2 capacity of 0.2 l O2 /l of blood and 95% O2 extraction by exercising muscles. 0.38 0.77 1.15 1.53 1.92 2.30 2.68 3.07 3.45 Total O2 uptake Ventilation Cardiac output RM O2 uptake RM O2 uptake RM blood flow RM blood flow O2 available for (l/min) (l/min) (l/min) (l/min) (% of total) (l/min) (% of total) exercise (l/min) Table 7: Total O2 uptake during exercise in an asthma patient plus per cent of the total required by respiratory muscles (RM) for energy requirements of breathing and that left over for sustaining exercise*. Anatomy and Physiology of the Human Respiratory System WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 25 26 Human Respiration probably be less than 1 l/min. Exercise is clearly limited by the respiratory muscles and high energy requirements of breathing. 6 Interactions of heart and lungs The lungs, thorax and heart constitute two interactive pumps, one pumping air (lungs and respiratory muscles of the thorax) and the other pumping blood (the right ventricle pumping blood through the lung for adding oxygen and removing carbon dioxide from blood returning from the periphery and the left ventricle pumping blood into peripheral organs to provide substrate and oxygen. The two pumps must interact efficiently within the gas-exchange region of the lungs to maintain normal arterial blood gases leaving the lung. Furthermore, since the heart pump lies entirely within the thoracic pump they must interact mechanically in a way that does not impede the function of the other pump, despite the fact that they pump at different rates and stroke volumes in a limited amount of space [44]. In fact, the interaction in many instances is probably beneficial. The pumping action of the heart causes pressure fluctuations in conducting airways and gas-exchange regions of the lung that may enhance uniformity of gas mixing in the lung. The diaphragm is the major inspiratory pump in the thorax and operates like an inspiratory piston that moves downward in upright humans to pull air into the lung during inspiration. In humans the diaphragm has a firm connection with the heart, which holds the diaphragm up against the pull of gravity at the end of a normal breath; at the end of a breath it is in position to exert its piston-like function for the next inspiration. Quadrupeds who normally run in a horizontal orientation do not have this connection between heart and diaphragm; consequently when they assume an upright position the diaphragm is not held up in a position necessary for an effective inspiratory stroke. These mechanical interactions between heart, lungs and thorax are not well understood in health or disease and need further study. Acknowledgement Figure 1 is reprinted with kind permission from Springer Science and Business Media ([1], Figure 82, page 111). Figure 10 is reprinted with permission from The American Society for Clinical Investigation ([36], Figure 5, page 364). Figures 3 and 11 [18], and Figures 6 and 8 [20] are reprinted with permission from Elsevier. The authors wish to acknowledge the assistance of D. Merrill Dane and Jeanne-Marie Quevedo on this chapter. References [1] Weibel, E.R., Morphometry of the Human Lung. Springer-Verlag: Berlin, 1963. [2] Hislop, A., Muir, D.C., Jacobsen, M., Simon, G. & Reid, L., Postnatal growth and function of the pre-acinar airways. Thorax, 27(3), pp. 265–274, 1972. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] 27 Hislop, A. & Reid, L., Development of the acinus in the human lung. Thorax, 29(1), pp. 90–94, 1974. Dunnill, M.S., Postnatal growth of the lung. Thorax, 17, pp. 329–333, 1962. Davies, G. & Reid, L., Growth of the alveoli and pulmonary arteries in childhood. Thorax, 25, pp. 669–681, 1970. Meyrick, B. & Reid, M.R., Ultrastructure of alveolar lining and its development. Development of the Lung, ed. W.A. Hodson, Marcel Dekker: New York and Basel, 1977. Proctor, D.F., Physiology of the upper airway. Handbook of Physiology, Section 3: Respiration, eds. A. Wallace, O. Fenn, & H. Rahn, American Physiological Society: Washington, 1964. Gonda, I., Particle deposition in the human respiratory tract. The Lung, Scientific Foundations, eds. R.G. Crystal, J.B. West, E.R. Weibel & P.J. Barnes, Lippincott–Raven: Philadelphia and New York, pp. 2289–2294, 1997. Johnson, R.L. Jr., Relative effects of air pollution on lungs and heart. Circulation, 109, pp. 5–7, 2004. Rohrer, F., Der Stromungswiderstand in den mensachlichens Atemwegen und Verzeigung des Bronchialsystems auf denAtmungsverlauf in verschiedenen Lungenbezwirken. Pfluger’s Archiv fur die gesamte Physiologie, 162, pp. 225–299, 1915. von Recklinghausen, H., Uber die Atemgrosse des Neugebhorenen. Pfluger’s Archiv fur die gesante Physiologie, 62, pp. 451–493, 1894. Mead, J. & Agostoni, E., Dynamics of breathing. Handbook of Physiology, Section 3 Respiration, eds. A. Wallace, O. Fenn & H. Rahn, American Physiological Society: Washington, p. 411–428, 1964. Ross, B.B., Influence of bronchial tree structure on ventilation in the dog’s lung as inferred from measurements of a plastic cast. Journal of Applied Physiology, 10(1), pp. 1–14, 1957. Fung, Y.C., A model of the lung structure and its validation. Journal of Applied Physiology, 64(5), pp. 2132–2141, 1988. Mercer, R.R. & Crapo, J.D., Three dimensional reconstruction of the rat acinus. Journal of Applied Physiology, 63(2), pp. 785–795, 1987. Denny, E. & Schroter, R.C., A mathematical model of the morphology of the pulmonary acinus. Journal of Biomechanical Engineering, 118, pp. 210– 215, 1996. Johnson, R.L. Jr. & Curtis, S.E., Experimental approaches to the study of gas exchange. Lung Biology in Health Disease, vol. 148: Pulmonary and Peripheral Gas Exchange in Health and Disease, eds. J. Roca, R. Rodriguez-Roisin & P.D. Wagner, Marcel Dekker: New York and Basel, pp. 45–119, 2000. Miller, W.F., Johnson, R.L. Jr. & Cushing, I.E., Mechanics of breathing. Clinical Cardiopulmonary Physiology, ed. B.L. Gordon, Grune & Stratton: New York, pp. 568–603, 1960. Otis, A.B., The work of breathing. The Handbook of Physiology. Section 3: Respiration, eds. A. Wallace, O. Fenn & H. Rahn, American Physiological Society: Washington, Vol. 1, ch. 17, pp. 463–476, 1964. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) 28 Human Respiration [20] [21] [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] [32] [33] Hsia, C.C.W. & Johnson, R.L. Jr., Exercise physiology and lung disease. Pulmonary and Critical Care Medicine, Update 5, ed. R.C. Bone, Mosby: St. Louis, Vol. 1, Sec. B.5, pp. 1–20, 1998. Krogh, M., The diffusion of gases through the lungs of man. Journal of Physiology, 49, pp. 271–300, 1914. Worth, H., Nusse, W. & Piiper, J., Determination of binary diffusion coefficients of various gas species used in respiratory physiology. Respiration Physiology, 32(1), pp. 15–26, 1978. Grote, J., Die Sauerstoffediffusionscostanten im lungengewebe und wasser und ihre temperaturebhangikeit. Pfluger’s Archiv fur die gesante Physiologie, 295, pp. 245–254, 1967. Power, G.G., Solubility of O2 and CO in blood and pulmonary and placental tissue. Journal of Applied Physiology, 24(4), pp. 468–474, 1968. Wilhelm, E., Balting, R. & Wilcock, J., Low pressure solubility of liquid gases in water. Chemical Reviews, 77, pp. 219–262, 1977. Roughton, F.J.W., Forster, R.E. & Cander, L., Rate at which carbon monoxide replaces oxygen from combination with human hemoglobin in solution and in the red cell. Journal of Applied Physiology, 11, pp. 269–276, 1957. Roughton, F.J.W. & Forster, R.E., Relative importance of diffusion and chemical reaction rates in determining the rate of exchange of gases in the human lung, with special reference to true diffusing capacity of the pulmonary membrane and volume of blood in lung capillaries. Journal of Applied Physiology, 11, pp. 290–302, 1957. Yamaguchi, K., Nguyen, P.D., Scheid, P. & Piiper, J., Kinetics of O2 uptake and release by human erythrocytes studied by a stopped-flow technique. Journal of Applied Physiology, 58(4), pp. 1215–1224, 1985. Constantine, H.P., Craw, M.R. & Forster, R.E., Rate of reaction of carbon dioxide with human red blood cells. American Journal of Physiology, 208(4), pp. 801–811, 1965. Meyer, M., Schuster, K.D., Schulz, H., Mohr, M. & Piiper, J., Pulmonary diffusing capacities for nitric oxide and carbon monoxide determined by rebreathing in dogs. Journal of Applied Physiology, 68(6), pp. 2344–2357, 1990. West, J.B., Tsukimoto, K., Matthieu-Costello, O. & Predilleto, R., Stress failure in pulmonary capillaries. Journal of Applied Physiology, 70, pp. 1731–1742, 1991. Permutt, S., Bromberger-Barnea, B. & Bane, H.N., Alveolar pressure, pulmonary venous pressure, and the vascular waterfall. Medicina Thoracis, 19, pp. 239–260, 1962. Butler, J., Reflections on waterfalls in the chest. The Pulmonary Circulation and Gas Exchange, eds. W.W. Wagner, Jr. & E.K. Weir, Futura Publishing: Armonk NY, pp. 389–401, 1994. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line) Anatomy and Physiology of the Human Respiratory System 29 [34] West, J.B. & Dollery, C.T., Distribution of blood flow and ventilation-perfusion ratio in the lung measured with radioactive CO2 . Journal of Applied Physiology, 15(3), pp. 405–410, 1960. [35] West, J.B., Regional differences in gas exchange in the lung of erect man. Journal of Applied Physiology, 17(6), pp. 893–898, 1962. [36] Michaelson, E.D., Sackner, M.A. & Johnson, R.L. Jr., Vertical distributions of pulmonary diffusing capacity and capillary blood flow in man. Journal of Clinical Investigation, 52(2), pp. 359–369, 1973. [37] Glenny, R.W., Bernard, S., Robertson, H.T. & Hlastala, M.P., Gravity is an important but secondary determinant of regional pulmonary blood flow in upright primates. Journal of Applied Physiology, 86(2), pp. 623–632, 1999. [38] Arora, N.S. & Rochester, D.F., Effect of body weight and muscularity on human diaphragm muscle mass, thickness, and area. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 52(1), pp. 64–70, 1982. [39] Robertson, C.H. Jr., Foster, G.H. & Johnson, R.L. Jr., The relationship of respiratory failure to the oxygen consumption of, lactate production by, and distribution of blood flow among respiratory muscles during increasing inspiratory resistance. Journal of Clinical Investigation, 59(1), pp. 31–42, 1977. [40] Hsia, C.C., Takeda, S.I., Wu, E.Y., Glenny, R.W. & Johnson, R.L. Jr., Adaptation of respiratory muscle perfusion during exercise to chronically elevated ventilatory work. Journal of Applied Physiology, 89(5), pp. 1725– 1736, 2000. [41] Reid, M.B. & Johnson, R.L. Jr., Efficiency, maximal blood flow, and aerobic work capacity of canine diaphragm. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 54(3), pp. 763–772, 1983. [42] Milic-Emili, G. & Petit, J.M., Mechanical efficiency of breathing. Journal of Applied Physiology, 15(3), pp. 359–362, 1960. [43] Blomqvist, C.G., Johnson, R.L. Jr. & Saltin, B., Pulmonary diffusing capacity limiting human performance at altitude. Acta Physiologica Scandinavica, 76(3), pp. 284–287, 1969. [44] Butler, J., The heart is in good hands. Circulation, 67(6), pp. 1163–1168, 1983. WIT Transactions on State of the Art in Science and Engineering, Vol 24, © 2006 WIT Press www.witpress.com, ISSN 1755-8336 (on-line)