Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Germ theory of disease wikipedia , lookup
Globalization and disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Gastroenteritis wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Urinary tract infection wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
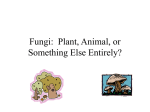
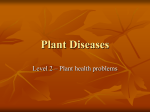
Weird Fungi Overall, more than 270 fungal species, some only weakly virulent, may produce disease in humans, particularly the immunocompromised John R. Perfect n the last decade, clinical practice has seen a boom in technology and therapeutic maneuvers to manage serious lifethreatening diseases. A consequence of this medical progress has been the frequent appearance of opportunistic infections among immunocompromised patients. This trend has been particularly noticeable in the appearance of medical mycoses. A common comment by clinicians in medical centers caring for severely immunosuppressed patients is “that is a weird fungus; is it causing disease?” There are no taxonomic terms for “weird fungi” or a specific species designation, but the axiom “you know them when you see them” usually applies. The definitions of weird include “of fate or destiny”; “suggestive of ghosts, evil spirits, unearthly, mysterious”; and “strikingly odd, strange, queer, bizarre.” These three definitions correspond to concepts that can be used to categorize these fungi in modern medicine. Beyond these terms, weird I • Even though some pathogenic fungi remain unfamiliar and appear “weird,” the basic principles of accurate diagnosis and creative treatment strategies still apply. • Immunocompromised individuals risk infections by more than 270 fungal species, with some only weakly virulent, and clinical outcome often reflects the seriousness of a patient’s underlying disease. • Foreign materials often foster fungal infections, and creative strategies may be needed to manage such infections, including the use of antiseptic solutions to treat topical infections or reconstituting immune responses to deal with recalcitrant internal infections. also embodies a useful mnemonic for clinicians and clinical microbiologists to keep in mind when confronting difficult cases: What is the epidemiology? Establish infection Invite experts to review these cases early Respond to infection with a plan Don’t ever give up with these infections unless underlying disease makes you. Even though such fungi tend to be viewed with too much awe because they are so unfamiliar, the basic principles of accurate diagnosis and creative treatment strategies still apply when it comes to managing complicated cases. Weird in Terms of Fate or Destiny First, it is important to emphasize that “weird fungi” may have institutional and geographical differences in their appearance. For instance, one medical center has described an impressive number of positive cultures for Fusarium species from a variety of environmental water sources. This environmental water contamination eventually led to cases of invasive fusariosis in neutropenic patients. In fact, with the use of molecular genotyping these environmental mould strains have been directly linked to clinical disease. However, it is important to emphasize that these fungi will not occur at the same frequency in all medical centers. Epidemiological differences between medical centers occur simply because environmental water contamination varies between institutions, and the risk population of patients may be significantly different. Second, persistently immunosuppressed patients cannot live in sterile environments. John R. Perfect is a Professor of Medicine in the Division of Infectious Diseases, Department of Medicine, Duke University Medical Center, Durham, N.C. Volume 71, Number 9, 2005 / ASM News Y 407 FIGURE 1 infection and even death. Therefore, the host frequently controls the destiny or fate of infection with these fungi. Finally, there is simply a lack of evidence-based studies for management of these “weird fungi.” The numbers of cases for each fungal species are simply too few, or cases are too complex, to allow any robust general statements about treatment strategies. Clinicians will frequently learn about management strategies one case at a time. Weird in Terms of of Ghosts, Evil Spirits, Unearthly, Mysterious Since many of these “weird fungi” are saprobes which might colonize nonsterile body sites or even contaminate cultures, it is important to have histological confirmation of infection and a positive culture from a sterile body site to document an etiologic agent for disease. For example, the histological appearance of uniform, septated hyphae A mixture of unicellular and multicellular elements caused uncertainty in the histologic diagnosis of Phialophora richardsiae subcutaneous infection, until culture results became in tissue could represent several moulds available. GMS stain, cutaneous biopsy. such as Aspergillus, Fusarium, or Scedosporium species, making culture identification helpful in clarifying what mysterious fungus is producing disease. It is more common for clinicians to manage On the other hand, frequently ribbon-shaped, these severely immunocompromised cases as nonseptated hyphae are detected in tissue with outpatients, who will be more frequently exZygomycetes infections while subsequent tissue posed to some of the over 270 fungal species in cultures are negative. Thus, tissue histopatholthe environment known to produce human disogy is the primary mode of identification. Some ease. This environmental exposure can reach moulds, such as Fusarium spp., Paecilomyces from the barnyard to the hospital, and a variety lilacinus, Scedosporium prolificans, Aspergillus of weakly virulent fungal strains produce infecterreus, and some of the black moulds, may tion in immunocompromised hosts. Furtherappear as both yeast and hyphae in tissue, as more, in many cases of disease with these “weird they produce adventitial forms at the site of fungi,” the clinical outcome does not necessarily infection. A solid organ transplant recipient develcorrelate with the virulence of the strain or its oped an infection with Phialophora richardsiae appearance of drug resistance, but its damage to that led to a cystic lesion on one hand, vividly the host simply reflects how advanced the underdemonstrating the weird morphology that some of lying disease of the patient may be. these fungi can produce (Fig. 1). For example, Shahid Husain and colleagues at Accurate mycological identifications of the University of Pittsburgh, Pittsburgh, Pa., “weird fungi” are essential. For instance, a studied the outcome of solid organ transplant bronchoalveolar lavage (BAL) fluid with Penirecipients with mould infections. The survival of cillium species growing in it raises vastly differpatients infected with fungal species was the ent clinical concerns compared to BAL fluid opposite of what one would predict from direct with Dactylaria gallopava. The first fungus is virulence studies of the fungal pathogens in anlikely an airway colonizer, and the second imals, illustrating that the weakest host fremould may be producing disease. In fact, except quently allows the “weirdest” fungus to cause 408 Y ASM News / Volume 71, Number 9, 2005 for Penicillium marneffei, there are very FIGURE 2 few cases in which Penicillium species have caused disease, despite their frequent isolation in nonsterile clinical specimens. On the other hand, the uncommon isolation of a Dactylaria species from a clinical specimen and its known virulence potential both in animals and humans make it a much more likely pathogen. While there are clinical circumstances in which obtaining histopathology and culture from a sterile body site is simply not possible, such as in the case of a severely neutropenic/thrombocytopenic cancer patient, there is simply no substitute for accurate clinical mycology in patients that are immunocompromised and require antifungal management. Mysteriously, weird fungi will occasionally contribute to an outbreak of multiple infections. For example, four cases of Phialemonium infection leading to two deaths occurred in patients undergoing chronic hemodialysis. Another outbreak of Phialemonium curvatum was associated with contaminated injectable drugs. In an impotence clinic, a vasoactive cocktail of drugs was used for intraLeft panels: Skin lesions caused by Rhizomucor sps. on arm before therapy. Top and cavernous penile injection for impotence. middle right panels: Rhizomucor skin lesions after 5 days of ABLC treatment. Bottom Three patients using these self-adminisright panel: New skin lesion on arm caused by Aspergillus flavus at 7 days of ABLC treatment. tered injections developed endocarditis with this weird fungus, which was later directly recovered from the drug vials. Similarly, five cases of Wangiella dermatitidis must be under strict sterility control or weird meningitis resulted from contaminated injectable fungi may infect patients. Care must also be steroids for back pain. Two of these patients died, taken to ensure that invasive technology is sterbut three received an extended treatment course ile. For instance, even mushrooms will grow on with voriconazole, and their infections were sucvascular stents within the human body. Another cessfully managed. example of direct fungal implantation is fungal There are several properties of weird fungal keratitis either through contact lenses, LASIX infections to keep in mind. First, as in those surgery, or corneal transplants. The cornea, three outbreaks, most “weird fungi” need help with its reduced vascular supply and with the to produce infection. They can grow at body frequent use of corticosteroid drops for corneal temperatures, but many species poorly adapt to eye disease, has become a common site of infecthe harsh host environment. However, foreign tion with “weird fungi.” Finally, some soft tisbodies from insertion of catheters and stents to sue infections with weird fungi exhibit few trauma from wood twigs and other inanimate symptoms in the patients for months or years, objects are common modes of introducing these making it difficult to identify the environmental fungi into the bloodstream, skin, or soft tissue of source for them. an immunocompromised host. As cases involvIn the management of infections with “weird ing contaminated drugs demonstrate, the profungi,” identification to a species level can also cessing and dispensing of injectable material be helpful to clinicians when choosing antifun- Volume 71, Number 9, 2005 / ASM News Y 409 Key Concepts Regarding Weird Fungi • Fungi may travel by weird routes to sites where they cause infection, including by contaminated skin lotions, twigs, catheters, stents, injectable medications, and even oral medications and nutritional supplements • Fungi may use peculiar routes to gain access to unexpected sites in the body; for instance, fungi such as Acremonium strictum, Trichoderma longibrachiatum, and Mucor indicus can enter through the gastrointestinal tract • Some odd behaviors of infectious fungi elude ready explanation • Many times weird fungi produce more fright than bite (see table); for instance, Trichosporon beigelii in urine typically is benign and a sign of a contaminated catheter, but in neutropenic patients it might indicate disseminated disease Weird fungi that produce infections in humansa Species that Produce Infections at Relatively Greater Frequencies Acremomium spp. Lasiodilodia theobromae Alternaria alternate Malassezia furfur Apophysomyces elegans Paecilomyces lilacinus Aspergillus terreus Paecilomyces variotii Bipolaris spp. Penicillium marneffei Bipolaris spicifera Phialemonium curvatum Blastoschizomyces capitatus Phialophora parasitica Candida krusei Phialophora richardsiae Candida lusitaniae Ramichloridium spp. Cladophialophora bantiana Rhizomucor pusillus Cunninghamella bertholletiae Rhizopus rhizopodiformis Curvularia lunata Rhodotorula rubra Exserohilum rostratum Saccharomyces cerevisiae Fusarium moniliforme Scedosporium prolificans Fusarium solani Trichosporon beigelii (T. asahii) Hansenula anomala Wangiella dermatitidis Species that Produce Infections at Relatively Lower Frequencies Absidia corymbifera Hormonema dematioides Acremonium strictum Lecythophora hoffmannii Aspergillus nidulellus Lecythophora mutabilis Aureobasidium pullulans Nodulisporium spp. Botryomyces caespitosus Penicillium spp. Candida zeylanoides Phialemonium dimorphosporum Chaetomium globosum Phialemonium obovatum Chrysosporsium parvum Phoma spp. Conidiobolus coronatus Pseudomicrodochium spp. Conidiobolus incongruus Rhinocladiella spp. Dactylaria constrica var. gallopava Saksenaea vasiformis Exophiala moniliae Schizophyllum commune Exophiala spinifera Scopulariopsis spp. Fusarium chlamydosporum Scytalidum spp. a From Perfect and Schell, Clin. Infect. Dis. 22:112–118, 1996. 410 Y ASM News / Volume 71, Number 9, 2005 gal treatments. For example, Paecilomyces variotii is generally very susceptible to standard antifungals, but Paecilomyces lilacinus can be resistant. Similarly, Scedosporium apiospermum responds to treatment with drugs such as voriconazole and possibly caspofungin, but Scedosporium prolificans is intrinsically resistant to available antifungal agents. Although not specifically predictive of clinical outcome, in vitro mould susceptibility testing with the NCCLS M38A method can indicate whether a strain may be clinically susceptible to a specific drug. Ultimately, “weird fungi” may require creative treatment strategies such as a combination of systemic drugs or even the use of antiseptic solutions for topical administration at the site of infection (e.g., soft tissue; cornea) along with surgical debridement. Weird in Terms of Strikingly Odd, Strange, Queer, Bizarre Although the majority of cases with invasive “weird fungi” occur in immunosuppressed patients, not all of them do. For instance, brain abscesses with Cladophialophora bantianum or Ramichloridium species may strikingly appear in apparently normal individuals. The “weird fungus” on the cover of this issue was cultured from a traumatic soft tissue infection in an apparently normal 15year-old female. Fungi such as Paecilomyces species can strangely produce infection by contaminating lotions used on the skin of bone marrow transplant recipients. Bizarrely, papular skin lesions may appear in immunocompromised hosts that, upon biopsy, show yeast even though cultures are negative. In such cases, clinicians must consider Malassezia species as a cause since these fungi need extra lipids to grow in commonly used clinical media. In some severely immunosuppressed patients, “weird fungi” can illustrate how some patients have become “human Petri dishes.” For instance, more than one fungal pathogen can cause infection at the same time in the same patient, making it necessary to biopsy two different skin lesions for histopathology and culture. Detection of more than one fungus might even lead to a change in management strategy, since we now have several different systemic antifungal drugs to use. In one case, a farmer with myelofibrosis progressing to leukemia developed several lesions on his arm after working in his garden (Fig. 2). These skin lesions were caused by Rhizomucor species. As therapy with amphotericin B lipid complex (ABLC) started to help heal these lesions, a new lesion started to grow on the arm that was caused by Aspergillus flavus. The treatment was changed to posaconazole, after which all skin lesions cleared. In considering individual cases of weird fungi, several important clinical issues stand out. First, there is no substitute for a correct diagnosis, and it may require both histopathology and culture confirmation. Second, reconstituting immune function may be essential to clear an established infection with a weird fungus, even when the in- fection is treated with very active antifungal agents. Third, in some cases, the burden of weird fungi may be so high that no antifungal therapy or immune reconstitution can control the infection. Finally, some of these weird fungi have caused so few reported cases of disease and are so refractory to standard treatments that a multilayer approach may be necessary for successful management. Infections with weird fungi at times need to be treated with weird therapeutic regimens. These regimens may entail combining topical and systemic antifungal agents (azoles, flucytosine, polyenes, candins, and allylamines), possibly with surgery and occasionally with immunomodulation therapy, such as gamma interferon and colony stimulating factors. The important feature for the final cure of these infections is frequently to correct or control the underlying disease and/or decrease immunosuppression. ACKNOWLEDGMENT The figures on fungal morphology, including the cover, were supplied by Wiley Schell from his photographic collection. SUGGESTED READING Anaissie, E. J., R. T. Kuchar, J. H. Rex, et al. 2001. Fusariosis associated with pathogenic fusarium species colonization of a hospital water system: a new paradigm for the epidemiology of opportunistic mold infections. Clin. Infect. Dis. 33:1871– 1878. Centers for Disease Control and Prevention. Exophiala infection from contaminated injectable steroids prepared by a compounding pharmacy. United States. 2002. Morbid. Mortal. Weekly Rep. 51:1109 –1112. Husain, S., B. D. Alexander, P. Munoz, R. K. Avery, S. Houston, T. Pruett, R. Jacobs, E. A. Dominguez, J. G. Tollemar, K. Baumgarten, C. M. Yu, M. M. Wagener, P. Linden, S. Kusne, and N. Singh. 2003. Opportunistic mycelial fungal infections in organ transplant recipients: emerging importance of non-Aspergillus mycelial fungi. Clin. Infect. Dis. 37:221–229. Itin, P. H., R. Frei, S. Lautenschlager, et al. 1998. Cutaneous manifestations of Paecilomyces lilacinus infection induced by a contaminated skin lotion in patients who are severely immunosuppressed. J. Am. Acad. Dermatol. 39:401– 409. Liu, K., D. N. Howell, J. R. Perfect, and W. A. Schell. 1998. Morphologic criteria for the preliminary identification of Fusarium, Paecilomyces, and Acremonium species by histopathology. Am. J. Clin. Pathol. 109:45–54. Lyratzopoulos, G., M. Ellis, R. Nerringer, et al. 2002. Invasive infection due to penicillium species other than P. marneffei. J. Infect 45:184 –195. Oliver, M. R., W. C. Van Voorhis, M. Boeckh, et al. 1996. Hepatic mucormycosis in a bone marrow transplant recipient who ingested naturopathic medicine. Clin. Infect. Dis. 22:521–524. Perfect, J. R., and W. A. Schell. 1996. The newer fungal opportunists are coming. Clin. Infect. Dis. 22(Suppl.):112–118. Proia, L. A., M. K. Hayden, P. L. Kammeyer, J. Ortiz, D. A. Sutton, T. Clark, H. J. Schroers, and R. C. Summerbell. 2004. Phialemonium: an emerging mold pathogen that caused 4 cases of hemodialysis-associated endovascular Infection. Clin. Infect. Dis. 39:373–379. Strahilevitz, J., G. Rahav, H. J. Schroers, et al. 2005. An outbreak of Phialemonium infective endocarditis linked to intracavernous penile injections for the treatment of impotence. Clin. Infect. Dis. 40:781–786. Volume 71, Number 9, 2005 / ASM News Y 411