Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
EEG REPORT
Patient: @NAME@
Age: @AGE@ MRN: @MRN@
Date: @ED@
Referring Provider: @REFPROD@
@EEGFLOW(3040141591,3040141592,3040141593,3040141594,3040141595,30401415
96,3040141597,3040141598,3040141599)@
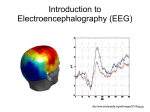
Introduction: This 21 channel standard 10-20 electrode routine {EEG length:304014049}
EEG was recorded with video-monitoring for a @AGE@ with a history of ***. This EEG
was performed to evaluate for focal and epileptiform abnormalities.
Current Medications: @NAME@ @CMEDPBRAND@
The patient {WAS,WAS NOT:23947:o} sleep deprived. Single lead EKG monitoring as
well as infraorbital electrodes were included.
Description: The dominant background activity during maximal recorded wakefulness
consisted of a ***Hz, *** uV {symmetric/unilateral/asymmetric:304014032}
{regular/irregular/disorganized:304014033} activity that was {reactive/nonreactive:304001168} to eye opening.
***Reactivity to {EEG reactivity:304014061} stimulation was ***.
***There was {ldprevalence:28138} *** Hz, *** uV, {ldrhythmic:28144},
{ldfrequency:28146} slowing over the {ldRLbilateral:28147} {EEG lobes:304014060}
region.
***There were {ldprevalence:28138}, {eeg :77378}, *** uV, {ldmorphology:28145} over
the {ldRLbilateral:28147} {EEG lobes:304014060} region. These occurred in
{ldrhythmic:28144} *** Hz runs lasting up to *** seconds.
***An electrographic seizure ***.
During drowsiness the background rhythm waxed and waned and there were periods of
slowing. During stage II sleep symmetric V waves, K complexes, and sleep spindles were
seen. There was appropriate diffuse delta activity during slow wave sleep.
Activation procedures {activation procedures:304014040}.
Photic stimulation – stepwise photic stimulation at 2-30 Hz was performed and
evoked {photic stimulation response:304014041}.
Hyperventilation – performed for {NUMBERS 1-4:25063} minutes, with {desc;
poor/fair/good/excellent:19665} effort by the patient. Changes noted included
{hyperventilation changes noted:304014042}.
Significant artifacts included {EEG significant artifacts:304014043}.
The EKG channel demonstrated {EKG channel:304014044}.
Interpretation:
This EEG was abnormal because of:
1. ***.
2. ***.
3. ***.
Clinical correlation:
This EEG was abnormal in {wakefulness_drowsiness_sleep_free:304014064}.
1. ***
2. ***
3. ***
***The disorganized background, with diffuse *** Hz slowing was consistent with a
mild/mild to moderate/moderate/moderate to severe/severe encephalopathy.
***The continuous focal slowing over *** was consistent with an underlying structural
lesion or a post-ictal state.
***The intermittent focal slowing over *** suggested underlying neuronal dysfunction.
The focal sharps/spikes/spike and wave complexes over *** conferred an increased risk
of focal seizures arising from this region.
***The generalized sharps/spikes/spike and wave complexes conferred an increased
risk of seizures with a generalized onset.
***The multifocal sharps/spikes/spike and wave complexes conferred an increased risk
of focal and generalized seizures.
***There were *** seizures recorded, clinically manifesting as ***, and with the
electrographic appearance of ***.
***There were *** events recorded, and there was no abnormal EEG change with these
events. These were not seizures.
***Overall, this EEG is improved/similar/worse compared to a previous EEG recorded
mm/dd/yyyy, because of ***.
***In view of the clinical picture, a recording including sleep/with reactivity testing
repeated/ with longer duration to capture spells, etc. could be useful. A normal
recording does not exclude the possibility of epilepsy, in this clinical setting, repeat
recording could be useful.
@MECREDENTIALNOREFRESH@
Epilepsy Fellow
This EEG was reviewed with epilepsy attending {ldattending:28131}. Please note this is a
preliminary report until signed by the attending.
Clinical Diagnosis Code:
{lddiagnosiscodesICD9-10:28354}