Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
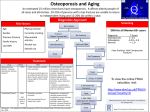
Short report on the Clinical Update Session: Management of osteoporosis By Bo Abrahamsen This session provided a thorough and systematic update on fundamental aspects of diagnosis and management of osteoporosis for clinicians and allied health professionals. Make the right diagnosis and understand risk assessment tools Professor Juliet Compston introduced secondary causes of osteoporosis and differential diagnoses, along with a presentation of the panel of clinical and paraclinical investigations available to the clinician and their respective limitations. A broad laboratory work-up aimed at ruling out vitamin D deficiency, genetic, endocrine and malignant diseases may be warranted, especially perhaps in younger patients who present with osteoporosis in the absence of strong risk factors. A presentation on risk factors, the extent of prescription of osteoporosis drugs relative to the expected burden of osteoporosis in various European countries and the development of FRAX was given by Dr Helena Johansson. There was a lot of interest from the audience and a number of critical questions about potential limitations to FRAX and gaps in the evidence base when it comes to selecting patients for treatment based on FRAX score, evidence that mainly builds on post-hoc analyses of trials that were designed before the development of FRAX. However, it was also argued that a high FRAX risk score is strongly associated with low BMD, the inclusion criterion generally used in the RCTs. The justification of the built-in mortality adjustment or death function in FRAX was also commented upon, in particular if this meant that FRAX was ageist and if the possibility that osteoporosis treatment could reduce mortality, as suggested by a number of recent studies, should perhaps count in favour of targeting treatment to patients at high risk of dying rather than the opposite. Consider new strategies for inhibiting the osteoblast yet allowing formation of new bone After the discussions on diagnosis and risk stratification, the session moved on to cover antiresorptive treatment (Professor Lorenz Hofbauer) and anabolic treatment (Professor Östen Ljunggren). The kinetics of anti-resorptives differ; some have only a short stay and bone while others are strongly bound and cleared very slowly. It is possible that the mechanism by which osteoclasts are made unavailable or unable to resorb bone may have an impact even on osteoblast activity. Professor Hofbauer proposed that kathepsin K inhibitors could be viewed as “uncoupling antiresorptives” with the capacity to maintain normal backcoupling from the osteoclast to the osteoblast, permitting continued bone formation despite the reduction in bone resorption. Taking up from there, Professor Ljunggren suggested that we should think about the possibility that we may have hit the ceiling with bisphosphonates, whereas we may still be able to obtain additional reductions in fracture risk with bone anabolic agents. After all, it is unclear how long we should be using anti-resorptives for in the individual patient, and the only other options seem to be building new bone and/or tackling sarcopenia and falls. Professor Juliet Compston commented that we should bear in mind that no evidence is available to demonstrate that anabolic treatment reduces the risk of hip fractures and that there is a loss of cortical BMD, at least in the early stages of treatment with PTH analogues. Though treatment is effective at group level, it may still need to be individualized to be effective in some patients. In the last lecture of the update session, Professor Richard Eastell discussed the concept of personalized osteoporosis treatment. The efficacy of osteoporosis drugs in preventing fractures have been clearly demonstrated at group level in RCTs, but how do we select the best treatment for the individual patient and how can we determine – if possible at an early stage – if treatment works in the patient and that fracture risk will be reduced? The currently available bone markers offer many advantages over the first generation markers. They have much better precision and can be used to identify suboptimal treatment responses or poor adherence to treatment. In future, we may be able to tailor individual treatment duration from bone turnover markers, perhaps giving long acting bisphosphonates such as zoledronic acid at much longer intervals so long as turnover markers remain in the therapeutic range. There is clearly a lack of good data on the optimum treatment duration and this is likely to be different for different medications as their half life in bone and duration of action is not the same.