Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
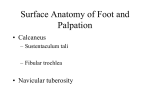
OrthopaedicsOne Articles 49 Plantar fasciitis Contents Introduction Anatomy Clinical Presentation Pathogenesis Physical Examination Imaging Conservative Treatment Operative Treatment Controversy References 49.1 Introduction Plantar heel pain is a common presenting condition. There are many causes of this malady, but one of the most common is plantar fasciitis. Unfortunately, plantar fasciitis is poorly understood and is frequently labeled and misdiagnosed as “heel spur syndrome.” Although heel spurs can occur with heel pain, recent research has found that they are not usually considered the cause. 19 The actual source of pain is still under debate. Some feel the pain is caused by trauma around the plantar calcaneal tuberosity from traction and shear forces from the plantar fascia, while others feel it is from a compressive neuropathy. Plantar fasciitis can be a painful and debilitating condition, which often frustrates not only the patient but also the treating physician because of its recalcitrant nature. The clinical presentation is well recognized, but there are no “gold standard” diagnostic tests to verify the diagnosis of plantar fasciitis. Typical findings of the condition include: Pain and palpable tenderness in the area of the medial calcaneal tuberosity Significant “start up pain” when taking the first few steps in the morning Worsening pain with prolonged weight-bearing In a small proportion of patients, the pain can radiate to the medial border of the heel, which is thought to be attributed to entrapment of the medial calcaneal branch of the posterior tibial nerve. No universally accepted treatment algorithm exists for this condition, but fortunately more than 90% of cases resolve with non-surgical conservative care.6 49.2 Anatomy Page 255 of 372 OrthopaedicsOne Articles The plantar fascia is a multilayered, fibrous aponeurosis located at the sole of the foot that originates from the plantar aspect of the calcaneus. It spreads broadly from the central third of the foot at the medial tuberosity of the calcaneus, then divides into five digital bands at the metatarsalphalangeal joints. Each band inserts into the base of the proximal phalanges, and fibers merge with the dermis, transverse-metatarsal ligaments, and flexor tendon sheaths. Three distinct compartments of intrinsic plantar muscles are also formed through strong vertical septa that divide the medial, central, and lateral portions of the plantar fascia. The terminal branches of the posterior tibial nerve and artery and the medial calcaneal, medial plantar, and lateral plantar supply cutaneous branches through the plantar aponeurosis. The plantar fascia can be said to be an anatomic extension of the Achilles tendon. It is essentially an inelastic structure with minimal elongation.8 During the toe-off phase of gait, the metatarsalphalangeal joints are dorsiflexed, which results in high tensile forces at the calcaneal origin of the plantar fascia. This has been referred to as the “windlass effect” of the plantar fascia.14 The plantar heel fat pad is a complex structure of multiple fibrous septa enclosed by adipose tissue that function as a shock absorber. This protects the underlying bone and soft tissue structures even with the heel absorbing 110% of body weight at heel strike and up to 200% while running.21 49.3 Clinical Presentation Obtaining a thorough history is extremely important in diagnosing plantar fasciitis and will often preclude the need for further imaging or diagnostic studies. A typical history of the condition begins with the patient describing the insidious onset of a sharp, stabbing inferior heel pain that localizes to the plantar medial aspect of the heel. The pain is at its greatest intensity when the patient takes the first few steps in the morning when arising from bed or from a chair after sitting for an extended period of time. The pain tends to lessen with activity, but worsens by the end of the day, especially after prolonged periods of weight-bearing. 10,22 The symptomatic patient will deny radiation of pain and will not usually have any associated parasthesia. Plantar fasciitis is primarily unilateral, accounting for 70% of all cases of the condition.3 Bilateral heel pain however, in conjunction with multiple sites of enthesopathy and joint pain, suggests a systemic rheumatologic disorder. The patient population between the ages of 40 and 60 is at the highest risk, along with those who describe themselves as running athletes or have occupations that require them to engage in prolonged periods of standing. Sudden increases in activity or training should lead the clinician to further investigate the possibility of a calcaneal stress fracture. Infection or neoplasm are the most likely cause of plantar heel pain when described as unrelenting or nocturnal pain or when accompanied by constitutional symptoms such as unplanned weight loss, fevers or chills. 49.4 Pathogenesis Page 256 of 372 OrthopaedicsOne Articles There is no widely accepted agreement as to the cause of plantar fasciitis, but mechanical derangements and restriction of motion are at the least contributory causes of both classic proximal fasciitis and the less-common distal plantar fasciitis. This is contrary to the popular belief that the presence of a heel spur is the causative factor in the development of plantar fasciitis. Recent studies, in fact, have suggested that only 50% of patients with heel pain will have heel spurs.7 Further, cadaveric dissections have revealed the presence of the spur within the flexor digitorum brevis as well as the abductor hallucis, rather than the plantar fascia itself.9 Thus, although heel spurs do indeed occur with heel pain, they are generally not considered the cause. The condition of plantar “fasciitis” denotes an inflammatory process, but histologic evidence is not in agreement with this notion. Findings demonstrate microtears in the fascia, myxoid degeneration, angiofibroblastic hyperplasia, and collagen necrosis.13 Such changes would suggest a non-inflammatory state of degenerative fasciosis secondary to chronic repetitive microtrauma of the plantar fascia. An inflammatory model of the development of symptomatic plantar fasciitis does, however, gain support in the concept that the inflamed plantar fascia tightens when the patient is at rest, especially as the foot and ankle assume an equinus position at night. Upon ambulation, with the foot and ankle in a now neutral and dorsiflexed position, the tissue contracts, producing heel pain typically at the origin of the plantar fascia with the first few steps in the morning or after prolonged rest. 49.5 Physical Examination The foot and ankle physical exam should be thorough and include inspection of the patient’s stance and gait. A pes planus or pes cavus foot deformity can increase loading through the plantar fascia. Obesity and limited ankle dorsiflexion are also risk factors for the development of the condition. A neurologic examination of the lower extremity and back should be done to explain paresthesias or abnormal sensation accompanying pain. The location of the pain is important in making the correct diagnosis. Pain associated with plantar fasciitis is most commonly linked with the origin of the plantar fascia in the area of the medial tubercle of the calcaneus. However, patients may experience pain more distal to the origin as the plantar fascia extends into the medial arch or branches into the five digital bands. Although possible, variations of the typical clinical finding of plantar medial heel pain should warrant further investigation of another diagnosis. Lastly, the diagnosis can be further identified through dorsiflexion of the toes, which typically exacerbates the pain in patients with symptomatic plantar fasciitis. 49.6 Imaging Page 257 of 372 OrthopaedicsOne Articles Imaging plays a limited role for the diagnosis of plantar fasciitis, as a thorough history and physical exam usually leads to the cause of the plantar heel pain. Although conventional radiographs are rarely needed for the diagnosis of plantar fasciitis, standing AP and lateral radiographs of the heel provide information about the osseous structures of the foot, as well as specific details of the calcaneus. A triple-phase bone scan may be warranted as an imaging study of choice when trying to differentiate plantar fasciitis from other plantar heel etiologies. This test can provide objective evidence of predictable increased uptake in the heel (medial calcaneal tubercle) that can differentiate the diagnosis of plantar fasciitis from calcaneal stress fracture. 17 Symptomatic improvement of the condition is also correlated with decrease in uptake over time.18 Magnetic resonance imaging (MRI) is seldom used for the confirmation of plantar fasciitis due to its low specificity. It will typically show increased signal intensity, thickening of the plantar fascia, and edema of surrounding structures. An MRI is useful, however, in excluding other causes of heel pain such as tumors and infection.20 Ultrasound is less expensive than an MRI and has been shown to be equally as effective as using a triple-phase bone scan in the diagnosis of plantar fasciitis.12 Ultrasound is also very quick and provides no radiation exposure, but is unfortunately user dependent. Typical findings include a thickened, hypoechoic plantar fascia with soft-tissue edema. Laboratory, electromyography (EMG) and nerve conduction velocity (NCV) studies can provide additional information for the clinician but are not routinely ordered. Laboratory studies are usually normal in the patient with plantar heel pain, but serum hematologic and immunologic testing can detect other systemic causes. HLA-B27, complete blood count, erythrocyte sedimentation rate, rheumatoid factor, antinuclear antibodies, and uric acid can be considered in patients with bilateral or atypical heel pain. 8 EMG/NCV studies are effective in identifying a spinal radiculopathy, peripheral neuropathy as well as local nerve entrapment. 49.7 Conservative Treatment Non-surgical treatment is the mainstay of treating plantar fasciitis, with an array of conservative strategies available to treat the condition. Non-surgical treatment is very effective, at a reported success rate of 85-90%.6,23 Common non-surgical treatments include: Achilles and plantar fascia stretching Activity modification Orthotic devices Short-term non-steroidal anti-inflammatory drug (NSAID) therapy Night splint use Formal physical therapy Immobilization via cast or boot Steroid injections Extracorporeal shock wave therapy A daily home stretching program focusing on Achilles and plantar fascia stretching exercises and eccentric Achilles strengthening exercises should be the initial treatment offered for the patient with plantar fasciitis (Figures 1-4) The patient should also be advised to modify his/her activities and minimize overuse by cross-training and losing weight. Page 258 of 372 OrthopaedicsOne Articles Figure 1. Gastroch stretch. Note that the back knee is straight and the back foot is internally rotated. Figure 2. Plantar fascia deep tissue massage Figure 3. Soleous stretch. Note that the back knee is bent and the back foot is internally rotated. Page 259 of 372 OrthopaedicsOne Articles Figure 4. Step stretch Concurrent NSAID therapy is often appropriate as studies have shown successful outcomes with its use, 1 although no study has specifically examined the effectiveness of this treatment alone. Steroid injections are commonly given for the symptomatic patient; evidence shows that injections give temporary relief but provide minimal long-term beneficial effect in most patients.15 In addition, complications of long-term use of steroid injections include plantar fascia rupture and fat pad atrophy, but these complications can be minimized by limited use and by placing the needle superior to the fascia on the medial side. Shoe inserts may also serve as an adjunctive therapy in helping to relieve symptomatic pain associated with plantar fasciitis. Orthotic devises such as a heel pad or cup, custom arch supports, and UCBL orthoses can optimize biomechanical loading of the foot and off-load the plantar fascia at its origin, as well as recreate the shape of the heel pad. Formal physical therapy can guide the patient with Achilles and plantar fascia stretching, as well as provide other therapies such as icing, heat, massage, iontophoresis, and taping. The use of a night splint offers symptomatic benefit and can alleviate morning start-up pain by managing fascia stretching during sleep. In the small percentage of patients with continued symptoms despite the therapies discussed above, casting and extracorporeal shock wave therapy (ESWT) can be beneficial. Application of a short leg walking cast or boot for 4-6 weeks may minimize repetitive microtrauma by unloading the heel and immobilizing the plantar fascia. The efficacy of immobilization in relieving plantar fasciitis has been supported in several retrospective studies.4,10 ESWT is a new treatment for recalcitrant plantar fasciitis and is based on lithotripsy technology to utilize powerful shock waves in breaking up scar tissue to enable the inflamed fascia to heal. That being said, ESWT is indicated only after the failure of three conservative therapies as well as recalcitrant proximal plantar heel pain for at least 6 months. ESWT therapy is well tolerated by most patients but should not be a treatment choice for patients with coagulopathies, hemophilia, malignancy, or open physes. 49.8 Operative Treatment Page 260 of 372 OrthopaedicsOne Articles All conservative options should be offered and tried for 6 months to 1 year before surgical intervention is considered. An open or endoscopic release of the plantar fascia remains a common method of surgical correction for patients with severe recalcitrant plantar fasciitis. Decompression of the first branch of the lateral plantar nerve can be done along with partial plantar fascia release if suspicion of entrapment of the calcaneal branches of the tibial nerve exists. The success of partial plantar fascia release remains a topic of debate, as some studies show an acceptable success rate,5,7 whereas others show a long-term patient satisfaction rate after plantar fasciotomy of less than 50%.11 Because of the high incidence of lateral foot pain and detrimental effects to the stability of the arch, it is recommended that less than 40% of the plantar fascia be released.2 Complications from release of the plantar fascia include prolonged healing and rehabilitation times, alteration of the biomechanics of the foot leading to a decrease in arch height, increased strain of the plantar ligaments’ cuboid attachment areas, and increased stress to the midfoot and metatarsal bones. Postoperatively, patients may experience acute plantar fasciitis, heel numbness, neuroma formation and infection. A new, less-invasive surgical technique has been described that utilizes bipolar radiofrequency microtenotomy (Topaz Procedure) to treat recalcitrant plantar fasciitis.16 Studies indicate that the radiofrequency in wound healing could lead to increased angiogenesis. Patients have reported a rapid recovery with pain relief though 24 months. Unfortunately, this technique has not been subject to prospective, randomized trials and further studies need to be undertaken to solidify its efficacy. 49.9 Controversy Controversy surrounds the effectiveness of a new treatment technique of utilizing platelet-rich plasma (PRP) injections to increase the concentration of growth factors at the site of injury and augment the natural healing process of chronic plantar fasciitis. The evidence for the use of this technique is limited; however, it does show compelling promise for clinical use if deemed successful by future clinical studies. Surgical intervention, especially endoscopic surgery, is also controversial due to the inherent risks of surgery as well as the relatively low long-term satisfaction rate of those that undergo this mode of treatment. This reality further necessitates the need to have the patient with plantar fasciitis undertake all non-surgical intervention for a period of 6 months to 1 year before entertaining the option of surgical correction. 49.10 References 1. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992; 279:229-236. 2. Berkowitz JF, Kier R, Rudicel S: Plantar fasciitis: MR imaging. Radiology 1991; 179:665-667. 3. Buchbinder R: Clinical practice: Plantar fasciitis. N Engl J Med 2004;350: 2159-2166. 4. Chen HS, Chen LM, Huang TW: Treatment of painful heel syndrome with shock waves. Clin Orthop Relat Res 2001; 387:41-46. 5. Conflitti JM, Tarquinio TA: Operative outcome of partial plantar fasciectomy and neurolysis to the nerve of the abductor digiti minimi muscle for recalcitrant plantar fasciitis. Foot Ankle Int 2004; 25:482-487. Page 261 of 372 OrthopaedicsOne Articles 6. Crawford F, Atkins D, Young P, et al: Steroid injections for heel pain: Evidence of short-term effectiveness. A randomized controlled trial. Rheumatology 1999; 38:974-977. 7. Davies MS, Weiss GA, Saxby TS: Plantar fasciitis: How successful is surgical intervention? Foot Ankle Int 1999; 20:803-807. 8. Donley BG, Moore T, Sferra J, et al: The efficacy of oral nonsteroidal anti-inflammatory medication (NSAID) in the treatment of plantar fasciitis: A randomized, prospective, placebo controlled study. Foot Ankle Int 2007; 28:20-23. 9. Forman WM, Green MA: The role of intrinsic musculature in the formation of inferior calcaneal exostoses. Clin Podiatr Med Surg 7(2):217-223, 1990. 10. Gill LH: Plantar fasciitis: Diagnosis and conservative treatment. J Am Acad Orthop Surg 1997; 5:109-117. 11. Hicks JH: The mechanics of the foot: II. The plantar aponeurosis and the arch. J Anat 1954; 88:25-30. 12. Kenzora JE: The painful heel syndrome: An entrapment neuropathy. Bull Hosp J Dis Orthop Inst 47:178-189, 1987. 13. Landorf KB, Keenan A, Herbert RD: Effectiveness of foot orthoses to treat plantar fasciitis: A randomized trial. Arch Intern Med 2006; 166:1305-1310. 14. Levy JC, Mizel MS, Clifford PD, et al: Value of radiographs in the initial evaluation of nontraumatic adult heel pain. Foot Ankle Int 2006; 27:427- 430. 15. Mizel MS, Marymont JV, Trepman E: Treatment of plantar fasciitis with a night splint and shoe modification consisting of a steel shank and anterior rocker bottom. Foot Ankle Int 16. Ogden JA, Alvarez R, Levitt R, et al: Shock wave therapy for chronic proximal plantar fasciitis. Clin Orthop Relat Res 2001; 387:47-59. 17. Saxena A, Fullem B: Plantar fascia ruptures in athletes. Am J Sports Med 2004; 32:662-665. 18. Sewell JR, Black CM, Chapman AH, et al: Quantitative scintigraphy in diagnosis and management of plantar fasciitis (calcaneal periostitis): Concise communication. J Nucl Med 21(7): 633-636, 1980. 19. Shmokler RL, Bravo AA, Lynch FR, et al: A new use of instrumentation in fluoroscopy controlled heel spur surgery. J Am Podiatr Med Assoc 78:194-197, 1988. 20. Snook GA, Chrisman OD: The management of subcalcaneal pain. Clin Orthop 82:163-168, 1972. 21. Tisdel CL: Heel pain, in Orthopaedic Knowledge Update: Foot and Ankle 22. Vohra PK, Giorgini RJ, Sobel E, et al: Long-term follow-up of heel spur surgery: A 10-year retrospective study. J Am Podiatr Med Assoc 1999;89:81-88. 23. Wolgin M, Cook C, Graham C, et al: Conservative treatment of plantar heel pain: Long-term follow-up. Foot Ankle Int 1994;15:97-102. Page 262 of 372